
Abstract
Background Forearm loop arteriovenous grafts most commonly fail because of stenosis, with thrombosis at the venous anastomosis. Treatment begins with identification of the stenotic lesion causing thrombosis, followed by either a percutaneous method using thrombolytic agents with possible balloon angioplasty and mechanical evacuation or surgical thrombectomy.
Case Report We present a case of thrombosis in a forearm loop graft with successful percutaneous thrombectomy. Preservation of this access site was only possible because of an unusual finding of collateral circulation, with the median cubital vein acting as a conduit to the basilic vein.
Conclusion The choice of surgical vs percutaneous methods for treating a thrombosed graft remains controversial. Yet the success rates of pharmacologic thrombolysis and the percutaneous approach are comparable to those of surgical thrombectomy. Our case of successful percutaneous thrombectomy illustrates the value of preserving the median cubital vein whenever possible in the placement of forearm arteriovenous grafts.
INTRODUCTION
Access for hemodialysis is best accomplished with the use of an arteriovenous fistula or graft. Fistulas are preferred over grafts because of lower rates of infection and thrombosis.1-3 However, arteriovenous grafts offer greater ease of placement and shorter time between placement of the graft and initiation of cannulation for hemodialysis. The treatment for access site thrombosis includes clot management using pharmacologic and/or mechanical evacuation techniques and stenotic lesion management using balloon angioplasty or surgical revision.1,2 We report the case of a patient who presented with thrombosis of a forearm loop arteriovenous graft and underwent successful percutaneous thrombectomy. Interestingly, the patient had developed an unusual adaptation via the median cubital vein to preserve his hemodialysis access.
CASE REPORT
A 79-year-old man with a history of end-stage renal disease on hemodialysis, secondary to hypertension and diabetes mellitus, was referred for a fistulogram because of suspected graft thrombosis. The patient had had a forearm loop graft placed 1 year prior and had had a declotting procedure 6 months prior in which a cephalic stent was placed because of cephalic arch stenosis. His medication regimen included insulin, levothyroxine, lisinopril, rosuvastatin, and aspirin. Pertinent physical examination findings of the arteriovenous graft revealed no thrill or bruit on auscultation. No upper arm edema was present, and the patient had strong bilateral radial pulses.
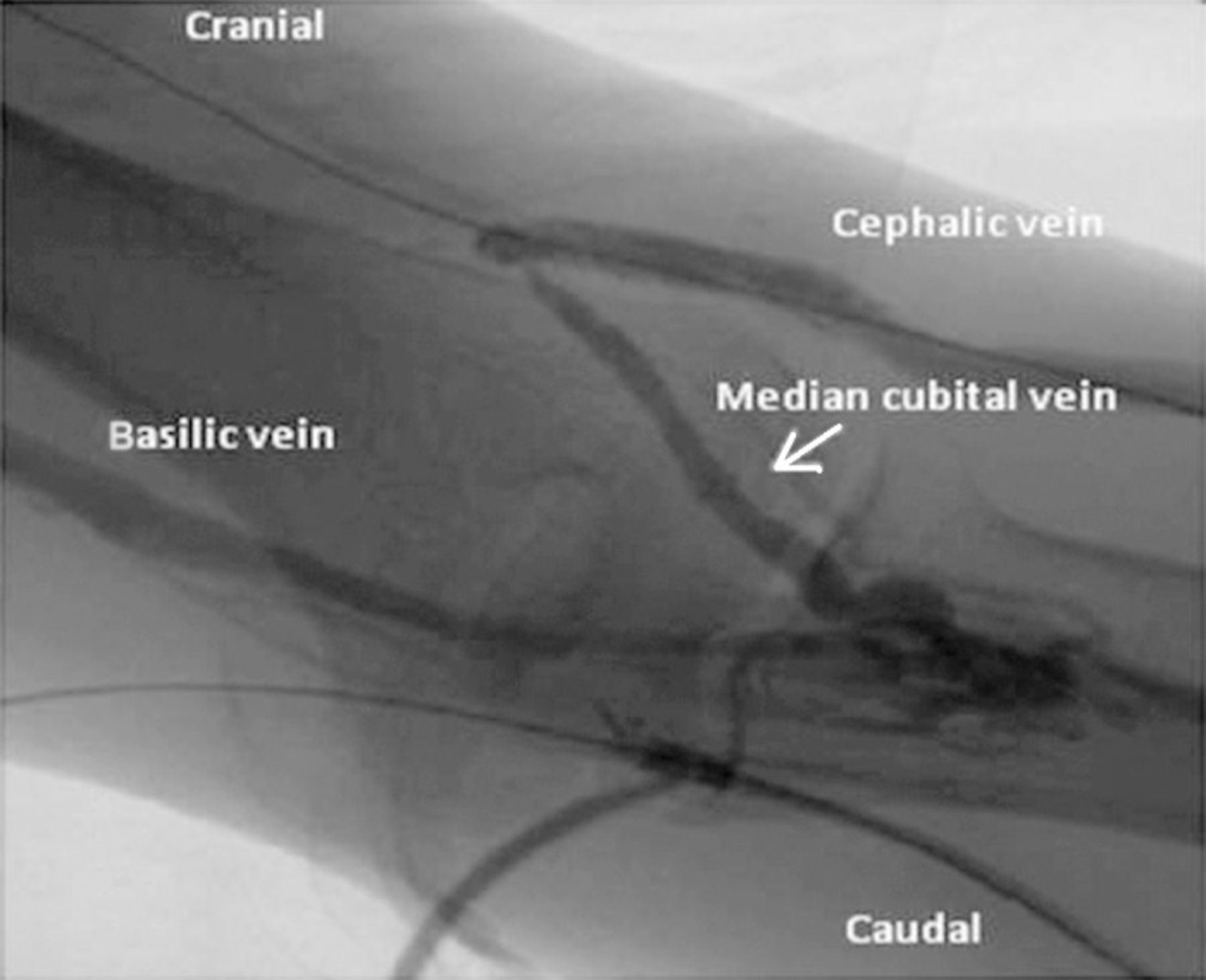
The arteriovenous graft was opened with intragraft administration of tissue plasminogen activator, venous angioplasty, and thrombectomy using an over-the-wire Fogarty catheter technique. The guidewire could not be successfully passed beyond the cephalic arch into central circulation because of an obstruction at the previously placed upper arm cephalic vein stent. Postthrombectomy fistulogram (Figures 1 and 2) revealed complete thrombosis of the cephalic vein at this venous stent. Interestingly, the arteriovenous graft was maintaining patency via the median cubital vein and a small accessory vein proximal to the cephalic vein stent (Figures 2 and 3).

Fistulogram displays the flow of dye (arrows) along the arteriovenous graft and the collateral blood flow in the cubital fossa.

Fistulogram shows the completely blocked stent across the cephalic vein (thin arrow) and the small accessory vessel heading into the basilic vein (thick arrow).

Fistulogram shows the blocked cephalic vein and collateral flow through the median cubital vein (arrow) into the basilic vein.
At 10 months postthrombectomy, the patient had no recurrent thrombosis or other arteriovenous graft complications. The graft maintained blood flow rates on dialysis averaging 450 mL/min, an average venous pressure of 230 mmHg, and adequate clearance with a recent Kt/V urea of 1.58 and urea reduction ratio of 77%. His medication regimen remained the same. No indication presented that necessitated adding another antiplatelet medication or starting anticoagulation.
DISCUSSION
Most arteriovenous graft failures are caused by intraluminal stenosis that is most frequently encountered at the venous anastomosis.4 The pathophysiology is somewhat similar to the restenosis seen in coronary arteries after revascularization, with histology revealing an inflammatory process and intimal hyperplasia.2,3 Blood flow rate and velocity, shear force, and compliance within a graft are thought to have a strong influence on the inflammatory response and the initiation and development of intimal hyperplasia.3,4 Several published studies and ongoing research address the prevention of stenosis, although an optimal strategy has yet to be identified.4
The mainstays of treatment of arteriovenous graft thrombosis are clot management using pharmacologic and/or mechanical evacuation techniques, identification of stenotic lesions causing the thrombosis, and management of significant stenotic lesions using either balloon angioplasty or surgical revision. The choice of surgical vs percutaneous methods for treating a thrombosed graft remains controversial. Yet the success rates of pharmacologic thrombolysis and the percutaneous approach are comparable to those of surgical thrombectomy.1-3 According to the 2006 National Kidney Foundation Kidney Disease Outcomes Quality Initiatives guidelines, the clinical success rate of arteriovenous graft thrombosis treatment should be 85%, with clinical success defined as the ability to use the graft for at least one hemodialysis treatment. Three months after percutaneous thrombectomy, primary patency should be at least 40%.1
In our patient, successful angioplasty of the native venous outflow tract in the cephalic vein was not possible. However, fluoroscopy revealed adequate collateral flow, enough to continue with hemodialysis using this arteriovenous graft. An arteriovenous graft can have one or more outflow veins that mature and become suitable conduits because of increased blood flow and pressure brought on by the arteriovenous graft itself. These outflow veins can be used to convert an arteriovenous graft to an arteriovenous fistula.5,6 To our knowledge, ours is the first case report showing a collateral vein as a conduit adequate for preserving the arteriovenous graft.
Our patient had had a venous stent placed that likely contributed to stenosis and thrombosis of the cephalic vein. However, the placement of his arteriovenous graft near the confluence of the median cubital and cephalic veins aided in the accessory flow to the basilic vein and in maintaining access.
CONCLUSION
Our case of successful percutaneous thrombectomy illustrates the value of preserving the median cubital vein whenever possible in the placement of forearm arteriovenous grafts.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care and Medical Knowledge.
ACKNOWLEDGMENTS
The authors have no financial or proprietary interest in the subject matter of this article.
- © Academic Division of Ochsner Clinic Foundation
In this issue








{kind=link}
{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.