
Abstract
The recent and continuing developments in radiotherapy, gene therapy, and the technologies of imaging, materials, and devices, as well as the techniques for their implementation, have expanded the options available for the treatment of peripheral vascular disease. Though long-term data are still lacking, percutaneous transluminal angioplasty (PTA) has developed into a treatment modality in its own right and continues to be an adjuvant treatment to traditional surgical revascularization. Numerous stents and grafts are currently available for the treatment of arterial lesions and aneurysms, while the testing of many more continues. In addition to these new devices, developments in gene therapy and brachytherapy have brought several new minimally invasive options to the treatment of peripheral vascular disease.
The explosive advancement of medical technology in the 1990s continues into the millennium at near exponential pace, mirroring the improvements seen in computer technology. Imaging techniques made possible by specialized computer software such as spiral computerized tomography scans with three dimensional reconstruction, digital subtraction angiography, and intravascular ultrasound have helped to provide the precision needed for “minimally invasive,” or endovascular treatment of peripheral vascular disease (1–3). Although the anatomic location of treatment (renal, iliac, femoral, or popliteal arteries) remains the center of much controversy, there is little disagreement between interventionalists and vascular surgeons that endovascular techniques are evolving and remain a part of the decision tree for peripheral vascular disease.
As the field of endovascular surgery has expanded, so too have the available techniques, devices, and materials, from the currently available angioplasty balloons, stents, covered stents, and abdominal aortic aneurysm stent-grafts to the newer alternative or adjuvant concepts of gene therapy and brachytherapy. “Minimally invasive” techniques refer to the method of introduction of the devices, whether by percutaneous methods or limited cutdown techniques; however, they remain significantly invasive to the vessel targeted for treatment—and this demands a thorough understanding of the patterns of vascular disease based upon anatomic location.
Percutaneous Transluminal Angioplasty (PTA)
The concept of percutaneous transluminal angioplasty (PTA) was introduced in 1964 when Dotter and Jenkins first demonstrated successful dilatation of stenotic lesions by passing a series of progressively larger, though rigid, coaxial dilating catheters across stenotic vascular lesions (4). The technique became popular only with the 1978 introduction of the flexible, twin-lumen balloon by Andreas Gruntzig.
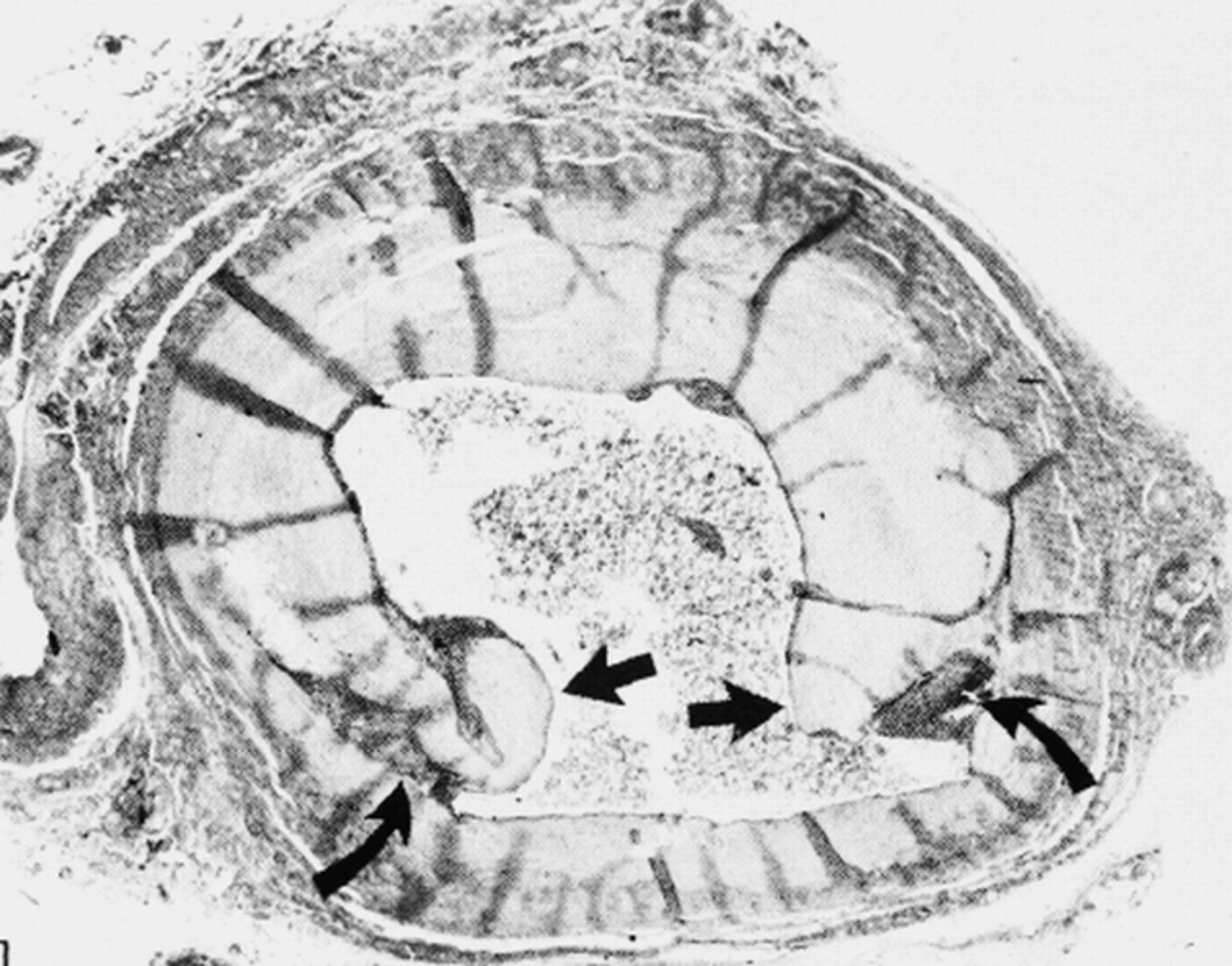
The technical details of lesion traversal, including the selection of the correct catheters and wires, vary with each particular lesion; however, the basic procedure of any angioplasty involves creating a controlled injury. Atheromatous plaque is incompressible and cannot be “squeezed” as Dotter originally postulated (4). Therefore, the primary mechanism of balloon dilatation entails the disruption of the plaque and its detachment from the arterial wall (Figure 1), which creates intimal fractures and minimal dissection of the media adjacent to the plaque (Figure 2). There is also some stretching of the uninvolved arterial wall leading to an enlargement of the lumen and an overall increase in the arterial diameter after remodeling (5).

Percutaneous transluminal angioplasty (PTA). A. Atherosclerotic plaque on longitudinal and cross-sectional view. B. Deflated angioplasty balloon inserted inside plaque. C. Inflated angioplasty balloon inside plaque with subsequent plaque rupture. D. End result of lesion post-angioplasty showing an increase in intraluminal diameter of the vessel

Histologic cross-section of an atherosclerotic lesion postangioplasty. Arrows point to regions of plaque fracture and disruption
Indications for PTA
In the past, the indications for peripheral vascular angioplasty had been conservative, emphasizing the avoidance of complications that would necessitate urgent surgical intervention. The past 5 years has seen a trend toward liberalizing indications (Table 1) as the technology, along with the skills and experience of practitioners, has continued to evolve. The resulting decrease in complication rates has helped angioplasty develop into an independent therapeutic procedure with its own indications and contraindications instead of being used simply as an alternative to surgery. In general, however, because it is less invasive, angioplasty may be performed as an initial procedure, the failure of which does not preclude the originally planned surgery. It can also be useful as an interim measure and an aid to healing, and can subsequently decrease the risk of surgery (6). Performed either preoperatively or intraoperatively, angioplasty can be of value by simplifying, shortening, and in some cases even improving surgical revascularization. It can also be a reasonable “last chance” limb salvage procedure when the only other alternative is amputation. Even though the long-term results are not great, the possibility of extending the patient's amputation-free survival, even if temporary, can tip the balance of the risk-benefit ratio towards intervention.
The principal clinical indications for angioplasty
The most controversial of all possible indications is the discovery of an asymptomatic lesion during the course of a diagnostic study. There is always the risk of progression of disease, but the important factor is symptomatology. A lesion should not be treated unless the interventionalist can prove it to be symptomatic. One only needs to remember that there is never such a thing as a “little procedure”; even a procedure considered low-risk can lead to catastrophic complications.
Lesions that are focal and shorter in length do well with angioplasty. There is a group of lesions, including long segments of disease or occlusions, for which angioplasty, although feasible, should not be the first line of therapy (7). Some of the contraindications to angioplasty are shown in Table 2.
Some contraindicaions to peripheral vascular angioplasty
Results: PTA vs. Surgical Revascularization
The patency data, especially in comparing this minimally invasive technique with surgical revascularization, are easy to find but difficult to analyze due to the classic “apples vs. oranges” problem of small samples and the equality of patient groups. Most questions remain unanswered; however, certain trends do emerge from the confusion of data. First, PTA patency rates tend to be lower than but parallel to those for surgery (8, 9). Second, patency rates for both techniques fall off as the periphery of the vascular tree is approached (10). Third, the same factors that affect PTA results (impaired runoff, rest pain, distal gangrene, continued smoking, diabetes, female gender) also affect the outcome of surgery. The immediate success and long-term benefits of PTA are significantly diminished by the problems of acute closure and postangioplasty stenosis (most of the former and some of the latter are related to extensive, flow-limiting dissections). The most important cause of restenosis is intimal hyperplasia and elastic recoil—though the process of restenosis and its relationship to the recurrence of symptoms are more complex and beyond the scope of this article.
Devices
The choice of the type (manufacturer) of balloon to use for angioplasty is usually dictated by physician preference, familiarity with the product, and contract negotiations with the respective company. In general, an appropriately sized balloon (diameter) should be used for the selected vessel in order to minimize the risk of complications. PTA usage has been reported in many series from the carotid arteries to the tibial arteries with varying results and follow-up patency rates (10–14).
The ultimate goal of PTA is an open vessel with a normal caliber. The idea of a vascular scaffold that would oppose elastic recoil, provide internal support, and preserve luminal patency and dimensions was pioneered many years ago. The myriad of early prototypes has led to two types of stents characterized by their expansion mechanism: balloon expandable and self-expandable, including those made of nitinol, a nickel and tantalum alloy with thermal memory expansion. Significant advances have been made in the last few years, and several prototypes have reached clinical trials and FDA approval (11). No ideal stent is yet available.
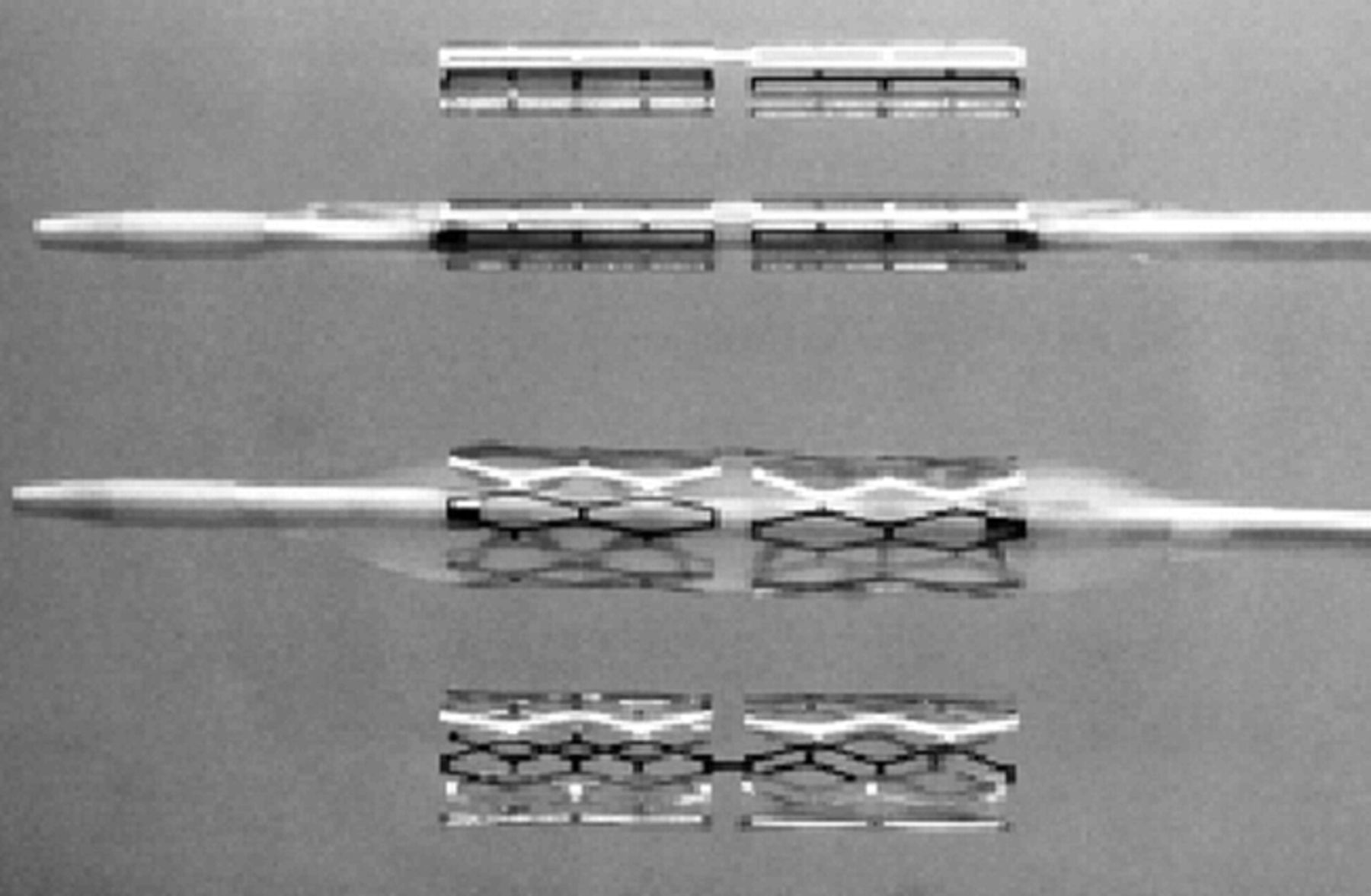
In assessing the various devices, the principles of deliverability, versatility, and biocompatibility are important considerations. Stents, available in a variety of lengths and diameters, are placed in vessels following angioplasty to help maintain vascular patency in an area of stenosis (Figure 3). In certain situations, a stent may be placed to aid in stabilization of an intimal dissection following angioplasty (Figure 4)⇓. Increased neointimal formation, localized inflammation, and even erosion through the vascular wall can occur following placement, making future surgical treatment extremely challenging and potentially increasing its morbidity (15).

Iliac stenosis amenable to angioplasty and possible stent placement

Figure 4a. External iliac dissection postangioplasty

Figure 4b. Stent in place to stabilize the dissection
The balloon-expandable stents are some of the earlier designs and are typically preloaded on a balloon. The Palmaz stent (Figure 5; Johnson & Johnson Interventional Systems, Warren, NJ) is made from stainless steel. Its hoop strength and high expansion ratio make it a durable stent; however, the lack of longitudinal flexibility makes it susceptible to permanent deformation in a tortuous vessel and difficult to deliver over the aortic bifurcation for a contralateral lesion. Another balloon-expandable, the Strecker stent (Boston Scientific/Vascular, Natick, MA) is a moderately flexible tube knit from a single tantalum filament. Its knitted design provides high radiopacity, good flexibility, and minimal shortening. Additionally, the tantalum fiber does not interfere with magnetic resonance angiography techniques (11, 15, 16).

Palmaz balloon-expandable stent
Self-expanding stents do not require a balloon and expand by resuming a preset configuration triggered by thermal memory at body temperature, or by a spring mechanism triggered when the device is unloaded from a constraining delivery catheter. The Wallstent (Figure 6; Schneider Stent, Plymouth, MN) is made of 16–20 stainless steel monofilaments mounted on a delivery catheter with an outer covering sheath; the stent automatically deploys and expands into position once the sheath is withdrawn. It has good strength and flexibility but can shorten once deployed making precise positioning difficult. The IntraCoil stent (Figure 7; IntraTherapeutics Inc., St. Paul, MN) uses the thermal shape memory of nitinol to reform its shape once it reaches body temperature. This stent, restrained on a delivery catheter, reportedly offers good flexibility and is easy to use. Another nitinol stent, the Memotherm Bard stent (Bard, Covington, GA) has a special diamond shape construction, but moderate hoop strength and little to no foreshortening upon deployment. It also has the disadvantage of minimal flexibility, making it inapplicable to angulations greater than 30°. The Symphony stent (Figure 8; Boston Scientific/Vascular, Natick, MA) is one of the newer self-expanding stents. Made of a single strand of nitinol configured to form a tubular implant of hexagonal cell patterns, this stent exhibits very little foreshortening upon deployment (17).

Self-expanding stainless steel Wallstent

Self-expanding nitinol IntraCoil stent

Self-expanding nitinol Symphony stent
Applications
Stents have been developed to deal with the major limitations of PTA, including the treatment of lesions that are unsuitable for angioplasty, acute failures with elastic recoil and/or dissection, and late failures due to restenosis. In some anatomical areas such as the aorto-iliac segment, stents have had their greatest impact on improving the immediate hemodynamic results of PTA and effectively managing recoil and dissection while also providing higher patency rates than PTA alone. In addition, lesions that were untreatable by PTA alone, such as iliac occlusions, can now be treated in combination with stenting. The benefit of primary stenting in the leg (below the iliac arteries) has not been proven. Lesions that are troublesome for percutaneous intervention, such as eccentric plaques, long-segment occlusions, long-segment stenosis, obstructive intimal flaps after PTA, and stenosis at graft anastomosis, occur more frequently in the femoropopliteal distribution, and, not surprisingly, stents have been applied as a potential solution. Although the immediate and early results have generally been good, and many angioplasty failures have been converted to successes with stents, long-term studies have shown less than promising results due to intimal hyperplasia and occlusion (15, 18). Therefore, at present it is wise to limit the application of these expensive devices to large or medium size arteries obstructed by post-PTA dissections or to elastic or eccentric lesions producing unsatisfactory results.
Stent-Grafts
As public enthusiasm continues to increase with regards to minimally invasive vascular techniques, interest in percutaneously delivered stents with synthetic graft coverings has also increased. Stent-grafts are being investigated for the treatment of both aneurysmal and peripheral occlusive arterial disease. The idea behind stent-graft placement was to create an endovascular bypass that could more closely approximate patency after surgical bypass and at the same time would be superior to PTA for long lesions. Technical success has been better with larger vessels (aortic, iliac) than with smaller more distal vessels (femoral, superficial femoral arteries) (19, 20).
The stent-grafts can be divided into three types based on their construction: (1) covered stents made by applying a covering of graft material such as polytetrafluoroethylene (PTFE) to a balloon or self-expanding stent, (2) stents used only as anchoring mechanisms for the graft material, and (3) the integration of weaving technology and stents.
Available Devices
Numerous types of aortic endograft systems are already under investigation for the treatment of infrarenal abdominal aortic aneurysms. Two stent-grafts are currently approved by the FDA, each representative of a particular design philosophy. The EVT Endograft (Figure 9; Endovascular Technologies, Menlo Park, CA) is a single-piece bifurcated graft. The prosthesis consists of self-expanding Z-stents covered with a tube graft of Dacron, a thin, woven polyester fabric. It is introduced into the aorta by unilateral femoral cutdown, with one limb (the contralateral) manipulated into position by guide wires using conventional interventional techniques. The AneuRx Endograft (Figure 10; Medtronic, Sunnyvale, CA) is a modular system made up of a nitinol exoskeleton and a Dacron endoskeleton. Delivery of the components requires two small groin incisions to expose the femoral arteries (21).

Bifurcated EVT Endograft for treatment of abdominal aortic aneurysms

Modular component AneuRx endograft for treatment of abdominal aortic aneurysms

Dr. Lepore is a Fellow in Ochsner's Section on Vascular Surgery
We have used both of these devices at Ochsner. Some of the limitations are dictated by the infrarenal aortic neck (from the renal arteries to the beginning of the aneurysm), which factors into landing the proximal portion of the graft. Other factors to consider when evaluating a potential candidate involve the complexity/angulation of the aneurysm and the diameter of the iliac arteries (to accommodate the size of the device). Overall, the modular endograft systems seem to provide more options to tailor the graft to each patient's anatomy and appear to be easier to use.
Experience with covered stents for the treatment of peripheral vascular disease or peripheral aneurysms is limited. For occlusive disease, it is postulated that an endoluminal stent-graft may limit the ingrowth of intimal hyperplasia along the length of the treated segment, thereby improving patency compared with other conventional treatments. For aneurysmal disease, the stent-graft may be used to bridge the aneurysmal segment and therefore occlude the aneurysm from the native circulation.
Other stent-grafts have been reported in the iliac and femoral systems with varied success (19, 22). The most commonly used devices are the Passager Stent-Graft (Minimally Invasive Technologies, La Ciotab, France) and the Prograft Hemobahn graft (W.L. Gore & Associates, Flagstaff, AZ). The Passager Stent-Graft is a self-expanding nitinol device covered with Dacron that comes compressed on a loading cartridge. The Hemobahn graft has a self-expanding nitinol exoskeleton supporting an ultrathin-walled PTFE endoskeleton with good flexibility, kink resistance, and radial stiffness. These devices are still early in their development and remain controversial compared with surgical techniques due to lack of long-term follow-up.
Gene Therapy
Along with the advancement in medical technology has come improvement in gene therapy techniques applicable to all fields of medicine. The two major areas of research in gene therapy that will likely have the greatest impact on peripheral vascular disease are gene therapy affecting vascular restenosis and neointimal proliferation, and gene therapy impacting angiogenesis and neovascularization. Research is being centered around affecting receptor expression such as the integrins ICAM-1 and VCAM-1 as well as growth factors, particularly platelet defined growth factor (PDGF) and fibroblast growth factor 2 (FGF-2) to augment restenosis and intimal thickening (23, 24). Other researchers have been working on the amplification of the angiogenic response by affecting vascular endothelial growth factor (VEGF) and its receptors. Trials using plasmid-mediated delivery of VEGF are ongoing and may offer some hope for the future of patients with end stage (inoperable) peripheral vascular disease (25). Ochsner Clinic and Alton Ochsner Medical Foundation are currently participating in a multicenter study on VEGF treatment for vascular occlusive disease.
Brachytherapy
Endovascular techniques are being combined experimentally with brachytherapy. Some clinical studies have suggested a substantial reduction in the restenosis rate with intraluminal irradiation of coronary and peripheral arteries applied in conjunction with angioplasty and stent placement (26, 27). After angioplasty and stent placement are completed, iridium (loaded on a wire) is placed over the region for a short period of time. Some clinicians feel this acts as prophylaxis against future restenosis for patients who are at high risk (28).
Conclusion
The technologic advances over the past decade have had a major impact on the treatment of vascular disease and created a new and exciting work environment for vascular surgeons. There are now many options to consider when treating the patient suffering from peripheral vascular disease, and the devices that are available to perform endovascular techniques continue to improve—though significant controversy exists and will continue as to the efficacy and validity of various treatment modalities. As the average age of the population continues to increase, so will the incidence of peripheral vascular disease. Although minimally invasive techniques have become an integral part of the treatment of these patients, it remains incumbent upon the treating physician to offer the best treatment to the patient. This will not necessarily be the least invasive.
- Ochsner Clinic and Alton Ochsner Medical Foundation
References
In this issue








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.