
Abstract
Omega-3 fatty acid therapy shows great promise in both primary and secondary prevention of cardiovascular (CV) diseases, especially coronary heart disease (CHD). In this review, we discuss the evidence available from prospective and retrospective observational epidemiologic studies and controlled clinical trials demonstrating the effects of omega-3 fatty acids (fish oil) in primary and especially secondary prevention of major CV events, including CV mortality, fatal and nonfatal myocardial infarction (MI), and sudden cardiac death (SCD). Significant reductions in total mortality and SCD to the extent of 20% to 50% have been found in studies using doses ranging from 0.85 to 4.0 g/d. We review the compelling evidence that indicates all clinicians should strongly consider therapy with fish oil, specifically eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), for patients with known CV disease and for patients at increased risk for CV disease, particularly patients at increased risk for SCD. The target DHA + EPA consumption levels are about 800 to 1000 mg/d for individuals with known CHD and at least 500 mg/d for individuals without disease.
- Coronary heart disease prevention
- DHA
- docosahexaenoic acid
- eicosapentaenoic acid
- EPA
- fish oil
- omega-3 fatty acids
Introduction
Substantial data indicate that elevated levels of low-density lipoprotein cholesterol (LDL-C), elevated levels of triglyceride-rich lipoproteins, and low levels of high-density lipoprotein cholesterol (HDL-C) are strongly associated with coronary heart disease (CHD).1–3 Platelets also play an important role in the pathogenesis of atherosclerosis and its complications.4–6 Numerous other risk factors for atherosclerosis, including elevated blood pressure, should be kept under control in the prevention of CHD.7 Omega-3 fatty acids are increasingly being utilized to provide substantial protection against cardiovascular (CV) disease.8–12 Table 111 summarizes the major classes of fatty acids; α-linolenic acid (ALA) is the prototype of the omega-3 fatty acids, which include eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). Numerous prospective and retrospective observational epidemiologic studies and randomized controlled trials from several countries, including Japan, India, and the United States, have shown that moderate fish oil consumption decreases the risk of major CV events, including myocardial infarction (MI) and sudden cardiac death (SCD).13–22 The purpose of the present review is to briefly summarize the effects of omega-3 fatty acids in primary and secondary prevention of CHD and SCD, including their effects on high-grade ventricular dysrhythmias and atrial fibrillation (AF). Finally, we conclude with a brief review of fish oil indications, their safety profile, and treatment guidelines.
Fish Oil and Primary Prevention
As early as 1944, Sinclair described the rarity of CHD in Greenland Eskimos despite their consumption of diet high in fat and cholesterol.23 Sinclair observed that the Eskimos had a tendency to bruise and to bleed easily, and subsequently Bang and Dyerberg demonstrated that the Eskimos had reduced platelet counts (50 000–80 000/mm3 lower) and decreased platelet aggregation, resulting in prolonged bleeding times. Bang and Dyerberg24,25 and Dyerberg et al,26 in their study comparing Greenland Eskimos and Danish controls, found, as expected, that the Eskimos, who eat about 500 g of fish per person per day (compared with 10–20 g/d in Westernized societies), had considerably higher levels of omega-3 fatty acids and lower levels of arachidonic acid in plasma, platelets, and red blood cell (RBC) membranes. Interestingly, in addition to reduced rates of CHD, the Greenland Eskimos also had a more favorable lipid profile and low levels of blood pressure. Coronary heart disease is also less prevalent in Japan, despite higher prevalences of hypertension (HTN) and smoking, which may be partly due to the Japanese population's traditionally high consumption of fish compared to populations in the Western world. Even within Japan, the Japanese islanders, who eat 3 times more fish compared to the mainland population, have lower rates of HTN, CHD, and all-cause mortality.8,11
In Westernized society, there is also evidence that increased consumption of fish is associated with decreased CHD. In the Zutphen study13 from the Netherlands, the 20-year mortality rate was 50% lower among those who ate 30 g of fish per day compared to those who did not eat fish. Data from the Multiple Risk Factor Intervention Trial (MR-FIT) in 6250 participants demonstrated reduction in 10-year mortality rates with increased consumption of polyunsaturated fatty acids.14 The US Physicians Health Study of 20 551 male physicians, of ages ranging from 40 to 84 years, demonstrated that consumption of fish at least once per week resulted in a 52% reduction in SCD during 11 years of follow-up.15 Patients in this study did not have any CV or cerebrovascular diseases prior to their enrollment in the study. The Nurses Health Study16 recently examined the dietary habits and the incidence of all kinds of strokes in 79 839 female nurses (ages 30 to 55 y at the time of enrollment). At the end of 14 years of follow-up, significant reductions in both thrombotic and lacunar strokes were noticed among women who consumed fish 2 or more times per week. This benefit was more apparent in women with higher baseline risk for stroke and those not taking aspirin. Similar positive effects of fish consumption on CV outcomes were noticed in the Honolulu Heart Program,27 where heavy smokers with high fish consumption were at lower risk for CHD mortality than those who smoked heavily and had low fish consumption. Table 2 outlines the potential beneficial effects of fish oils.8
On the contrary, there are a few epidemiologic studies that failed to show beneficial effects of high fish oil consumption on CV events. The Health Professionals Follow-up Study28 found that increasing fish intake from 1 to 2 servings per week to 5 or 6 servings was not associated with any reduction in the risk of CHD among men who were initially free of CV disease. A case-control evaluation of 14 916 participants from the Physicians Health Study group29 demonstrated similar baseline levels of EPA and DHA in those who had an MI versus those who did not have an MI during 5 years of follow-up. The Health Professionals Follow-up Study28 and the Physicians Health Study29 included cohorts with potentially higher baseline intake of omega-3 polyunsaturated fatty acids (PUFAs) than those in other cohort studies. These studies also involved cohorts at low risk of CHD and included few participants with low fish consumption (less than once per week). A threshold effect in which fish intake is cardioprotective in small amounts may partially explain these discordant results.30,31
The Japan EPA lipid intervention study (JELIS),17 a primary and secondary prevention trial, tested the hypothesis that long-term addition of 1800 mg/d of highly purified EPA to statin (ie, simvastatin and pravastatin) therapy can reduce the incidence of major CV events in Japanese patients with hypercholesterolemia. JELIS randomized 14 981 patients for primary prevention and 3664 patients for secondary prevention in a prospective open-label, blinded endpoint study with a 4.6-year follow-up. In addition to the large sample size, this study had the advantages that all patients were given low-dose statin therapy and continued to consume a diet rich in omega-3 fatty acids. At the end of 54 months, the primary endpoint of the trial, major adverse CHD events (composite end point of nonfatal MI, CHD death, unstable angina, and revascularization procedures) was reduced by 19% (P = .015). There was no significant reduction in SCD among patients receiving therapy for primary prevention or even among patients treated for secondary prevention. This finding seems to be at odds with the GISSI-Prevenzione trial,18 which reported a 45% decrease in the risk of SCD in post-MI patients. The authors of the JELIS trial reconcile this difference by stating that Japanese populations already consume more fish compared to Western populations and that their baseline population CV death rates are lower than those in the Western world. Therefore, there might be a dose beyond which additional antiarrhythmic effects may not be seen.30 However, these findings suggest that the benefits of omega-3 fatty acids may also be found in populations consuming large amounts of fish, ie, with higher doses of omega-3 fatty acids, cardioprotective effects other than arrhythmia reduction may be observed. Reductions in the incidence of unstable angina and nonfatal CHD events suggest that other, plaque-stabilizing properties may also be involved with omega-3 fatty acid therapy.30,32
Fish Oil and Secondary Cv Prevention
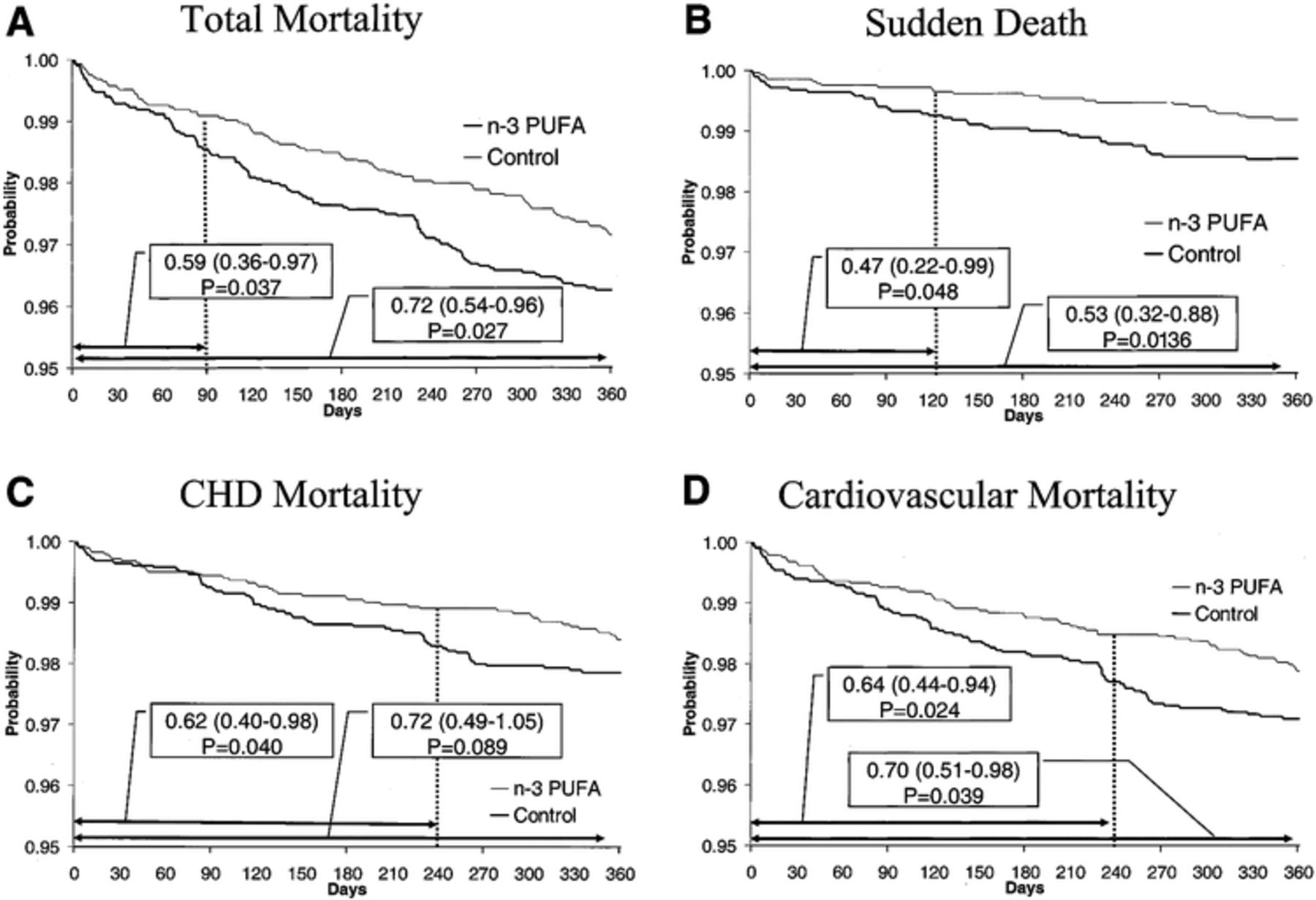
There is now mounting evidence suggesting that fish oil has substantial beneficial effects in the secondary prevention of CV events. In the GISSI-Prevenzione trial,18 11 323 patients who had suffered an MI within the previous 3 months were randomized to receive a fish oil supplement (1 g daily containing 850 mg of concentrated EPA and DHA) versus no supplement, 300 mg of a vitamin E supplement versus no supplement, and both supplements versus no supplements. The primary combined efficacy endpoint was death, nonfatal MI, and stroke. Patients taking fish oil supplements had a 15% risk reduction in the primary endpoint, including 21% and 30% reductions in total and CV mortality, respectively. Further analysis revealed that this endpoint reduction was driven by a highly significant 44% reduction in SCD18,33,34 (Figure 1). Moreover, SCD reduction reached statistical significance after only 4 months of randomization. However, vitamin E showed no efficacy alone or in combination with fish oil.33,34 The authors concluded that in order to save 1 patient in a population at relatively low risk (annual mortality 2.6%), 164 patients would need to be treated for 1 year with omega-3 fatty acids.33

(Reproduced with permission from Marchioli R, Barzi F, Bomba E, et al. Circulation 2002;105:1897–1903.33)
Thus, the antiarrhythmic effect observed in the GISSI trial is due to the low background dietary intake of omega-3 fatty acids, high baseline risk of SCD, and entry requirement of a recent MI. In contrast, the other existing literature, including the JELIS trial, suggests that the reduction of nonfatal CHD events may require higher doses (2–3 g/d of DHA + EPA) and/or a longer duration of treatment (3 to 5 y).17,30 In a subgroup analysis of findings from the GISSI trial, Macchia and colleagues35 found that the magnitude of reduction in mortality due to SCD increased with progressively worsening left ventricular (LV) systolic function (Figure 2). The effect of n-3 PUFA treatment on SCD was related to the degree of systolic dysfunction (test for trend P = 0.02), with the benefit on SCD reduction in patients with ejection fraction (EF) less than or equal to 40% being 4-fold higher than in those with EF greater than 50%.

(Reproduced with permission from Macchia A, Levantesi G, Franzosi MG, et al. Eur J Heart Fail 2005;7:904–909.35)
The Diet and Reinfarction Trial (DART)19 examined the effects of dietary intervention in the secondary prevention of MI in 2033 men who recovered from a recent MI, and these patients were allocated to 3 different dietary advice groups: (1) fat advice group, in which participants were advised to reduce dietary fat intake to 30% of total energy and to increase the polyunsaturated/saturated (P/S) ratio to 1; (2) fiber advice group, in which participants were advised to increase their intake of cereal fiber to 18 g daily; and (3) fish advice group, in which participants were instructed to either eat at least 2 weekly portions (200–400 g) of fatty fish (mackerel, herring, kipper, pilchard, sardine, salmon, or trout) or to take a daily fish oil supplement. After 2 years of follow-up, the fish/fish oil group showed a 29% reduction in all-cause mortality compared to the remaining 2 groups (P < 0.05), with the difference entirely attributable to a reduction in CHD deaths. The reduction in CV events was particularly impressive in the subgroup that took the fish oil supplement as opposed to simply increasing dietary fish consumption.
The Indian Study on Infarct Survival20 also demonstrated a significant effect of omega-3 fatty acid therapy on mortality in patients who had an MI. In this study, 360 Indian patients were randomized within 24 hours following an MI to receive fish oil providing 1.08 g/d of EPA plus 0.72 g/d of DHA; 20 g/d of mustard seed oil (the fatty acid composition of which is predominantly oleic acid, linoleic acid, and erucic acid); or a placebo of 100 mg/d of aluminum hydroxide. The combined primary endpoint of total CV events consisted of SCD, total CHD deaths, and nonfatal reinfarction. At 1-year follow-up, there were significant reductions in total CHD events and nonfatal MI and a 50% reduction in SCD in the fish oil and mustard oil groups when compared with the placebo group. The fish oil and mustard oil groups also showed significant reductions in total cardiac arrhythmias, LV enlargement, and angina pectoris compared with the placebo group. The study population was significantly different from those in other published studies in that they were enrolled within 24 hours of symptoms of MI and were predominantly vegetarian, consistent with the demographics of the part of India where the trial was conducted, although no baseline data were provided for documentation. In addition, they did not receive the aggressive treatment typical of modern post-MI therapies. In fact, only 30% of patients were treated with beta-blockers and 20% with angiotensin-converting enzyme inhibitors, and the use of lipid-lowering drugs was not reported.
Increased intake of fish oil in several studies demonstrated an effect in retarding or even reversing the progression of atherosclerotic heart disease. Von Schacky and associates,36 in the randomized, double-blind Study on Prevention of Coronary Atherosclerosis by Intervention with Marine Omega-3 fatty acids (SCIMO), evaluated the effects of omega-3 fatty acid therapy on angiographic endpoints in 223 patients using 6 g/d of fish oil (EPA + DHA, 3.3 g/d) for 3 months and then 3 g/d for 21 months versus placebo. Patients in the placebo group were treated with capsules containing a blend of oils comparable to that of the typical European diet, but the blend was free of EPA and DHA as well as the precursor omega-3 fatty acid ALA. All participants had a greater than 20% stenosis in at least 1 coronary artery on angiography and had revascularization (percutaneous coronary angiography or carotid artery bypass graft) planned or performed in the previous 6 months in no more than 1 vessel. Comparison of baseline versus posttreatment angiograms showed that coronary segments in the fish oil group showed less progression and more regression than segments in the placebo group. A very small study by Sacks and colleagues37 in 59 patients was designed to examine differences in angiographic endpoints, and the authors also reported CV events. Thirty-one patients on fish oil (6 g/d) were compared with 28 patients receiving an olive oil placebo. Fish oil therapy did not result in significant reductions either in the incidence of CV death and MI or in revascularization rates in this very underpowered study.
Fish Oil and High-Risk Ventricular Arrhythmias
Recently reviewed cumulative data by Anand et al32 demonstrate benefits of DHA + EPA against AF as well as trends toward benefits in malignant ventricular arrhythmias. Although omega-3 fatty acids appear to be effective for reducing SCD in the setting of CHD with reduced LV systolic function, 3 trials using omega-3 fatty acids in patients with implantable cardioverter defibrillators (ICDs) have shown mixed results. Raitt et al38 examined whether omega-3 PUFAs have any beneficial antiarrhythmic effects in patients with electrocardiographically documented ventricular tachycardia and fibrillation (VT/VF). The study randomized 200 patients with ICDs to treatment for 2 years with either 1.8 g/d of an omega-3 fatty acid supplement containing 42% EPA and 30% DHA ethyl esters or an olive oil placebo. The primary endpoint was time to first episode of ICD treatment for VT or VF. Although the treatment groups did not differ significantly in the number of episodes of VT and VF observed during follow-up, an overall trend toward an increased incidence of VT and VF was observed in the group receiving omega-3 fatty acid supplementation. In the subset of 133 patients whose entry arrhythmia was VT, 79% of the patients in the fish oil group experienced VT/VF at 24 months compared to 65% of patients in the control group (P = .007). The omega-3 fatty acid group had significantly higher rates of recurrent episodes of VT or VF compared to the placebo group (P < .001), suggesting that these supplements may even be proarrhythmic in certain patients.
Another recently completed trial called the Fatty Acid Antiarrhythmia Trial (FAAT),39 conducted by Leaf et al in 402 patients with an ICD, randomized patients to 2.6 g/d of omega-3 fatty acids versus 4 g/d of an olive oil placebo. The primary endpoint was time to first ICD event for VT or VF or death from any cause. The noncompliance rate was high but similar between the 2 groups. Despite this shortcoming, at 1 year follow-up, the omega-3 fatty acid group showed a positive trend toward a longer time to first ICD event (VT or VF) or death from any cause, with a risk reduction of 28% (P = .057). However, when the authors included probable episodes of VT/VF, the risk reduction became statistically significant at 31% (P = .033). Moreover, after adjusting for subjects who were compliant for 11 months or longer, the risk reduction approached 38% (P = .034). In subgroup analysis, the effect was greatest in patients with CHD and in those with left ventricular ejection fraction less than 30%.
The antiarrhythmic effects of omega-3 fatty acids have also been investigated in another recently completed multicenter, randomized, double-blind parallel trial, the Study on Omega-3 Fatty Acids and Ventricular Arrhythmia (SOFA).40 The trial included 546 patients with an ICD in place who had at least 1 episode of VT or VF during the previous year. Patients were randomized to 2 g of fish oil (464 mg EPA and 335 mg DHA) or high–oleic acid sunflower oil placebo for 12 months. The primary outcome was incidence of recurrent spontaneous VT or VF and all-cause mortality. At 1 year, no observable event-free survival difference was observed between treatment groups (70% vs 67% for fish oil vs placebo). However, in subgroup analysis, in patients with prior MI (n = 342), there was a nonsignificant trend toward longer event-free survival in the fish oil group compared with the placebo group (71% vs 63%, P = .09).
The authors speculate that the positive effects observed in FAAT,39 in contrast to the negative results reported in SOFA40 and in the trial by Raitt and associates,38 may be attributed to the possible inclusion of 2 very different ICD populations. FAAT included patients with recent MI, whereas Raitt et al did not have any patients with recent MI, suggesting that fish oil therapy may be more beneficial in preventing ventricular arrhythmia in CHD patients, especially those with recent MI, as there is a lower amount of scar tissue in these patients.
Overall, 2 of the 3 ICD trials support at least a modest benefit of omega-3 PUFAs for the prevention of high-risk ventricular arrhythmias.32,41 Omega-3 PUFAs also appear to be effective in reducing SCD in patients with ischemic LV systolic dysfunction.35 Results of the ongoing large randomized GISSI-Heart Failure Study (GISSI-HF or GISSI V) involving 7000 heart failure (HF) patients are anticipated in 2008 and should shed more light on the effects of DHA + EPA on outcomes in patients with reduced LV systolic function.42
Fish Oil and Af
Recent research has suggested a greater role for omega-3 fatty acids not only with respect to ventricular arrhythmias and autonomic tone but also in the management of AF. Mozaffarian et al43 demonstrated a 30% lower risk of incident AF over a 12-year follow-up period in patients who consumed tuna or other broiled/baked fish. The relationship between increased fish consumption and lower incidence of AF persisted even after correcting for variables such as age, gender, education, smoking, CHD history, diabetes, HF, and MI. However this does not prove causality. Another study, from Calò and colleagues,44 investigated the effect of preoperative and postoperative treatment with omega-3 PUFAs in preventing the occurrence of AF after bypass surgery in a total of 160 patients with no prior history of AF. Patients were randomized to an omega-3 PUFA group, who received an average dose of 850 to 882 mg/d of EPA and DHA from a variety of commercially available preparations, vs a placebo control group. Omega-3 supplementation was initiated 5 days prior to surgery and was continued until the seventh postoperative day on average. New-onset postoperative AF was noticed in 33.3% of the control cohort and in 15.2% of the PUFA cohort (P = .013). After bypass, the PUFA patients were also hospitalized for significantly fewer days than controls (7.3 ± 2.1 vs 8.2 ± 2.6 d, P = .017). Crystal et al45 described efficacy of omega-3 PUFAs comparable to amiodarone, beta-blockers, and sotalol in prophylaxis against AF postbypass. In view of this evidence, omega-3 PUFAs could be used to prevent AF postbypass particularly in patients with contraindications to sotalol or beta-blockers (ie, chronic obstructive lung disease or bradycardia), and it is thought that the antiarrhythmic and anti-inflammatory properties of PUFAs could have played an essential role in preventing AF after cardiothoracic surgery.32
Omega-3 Mechanisms
Omega-3 fatty acids appear to confer CV health benefits largely through DHA and EPA enrichment of membrane phospholipids.46–48 Large doses (3–5 g/d) of fish oil have been shown to produce a 30% to 50% reduction in triglycerides, whereas in most studies low-dose therapy (eg, 1 g/d) has not been associated with any lipid improvements, although the GISSI trial using 850 mg/d did show a very small (3.4%) but statistically significant reduction in triglycerides.18 Therefore, other mechanisms must play a major role in the clinical effects of fish oil, particularly in the antiarrhythmic effects and in the reduction of SCD.30,32 Table 3 shows the relationship between baseline blood levels of long-chain omega-3 fatty acids and risk of SCD. The level of long-chain n-3 fatty acids was significantly and inversely related to the risk of SCD.49
A relatively low daily dose of 810 mg of DHA + EPA has been shown to decrease resting heart rate, increase postexercise heart rate recovery, and increase beat-to-beat heart rate variability, all of which represent improved autonomic tone, or the balance between vagal/sympathetic activity.50,51 Moreover, high doses of fish oil have also been shown to lower blood pressure.52,53 More than a decade ago, we demonstrated that fish oil therapy resulted in a significant 25% reduction in mean arterial pressure and systemic vascular resistance, a modest reduction in LVH, and modest improvements in LV diastolic filling in cardiac transplant patients with cyclosporine-induced hypertension.52 These changes appear to be manifestations of augmented vagal tone, suggesting that omega-3 fatty acids may confer cardioprotection in part by improving autonomic sympathovagal balance.54 Fish oils, similar to long-term exercise, have many properties in the blood leading not only to increased fibrinolytic activity but also to reduced whole-blood viscosity and increased red blood cell deformability, all of which improve tissue perfusion at a cellular level.55 Other studies in heart transplant patients, however, suggest that the omega-3 fatty acid–induced improvements in autonomic tone may not be entirely vagally mediated.56 Additionally, we recently demonstrated that very high doses of omega-3 fatty acids (ie, 8 g/d) provide anti-inflammatory effects and improve body composition in HF patients.57
By reducing transcription of inflammatory cytokines and by other mechanisms, fish oil has been shown to have significant anti-inflammatory effects.58 These effects may extend its use to patients with chronic inflammatory conditions such as rheumatoid arthritis and ulcerative colitis.59,60 These anti-inflammatory properties may also play an important role in stabilization of unstable plaque in patients with acute coronary syndrome (ACS).30–32 Eicosapentaenoic acid competes with arachidonic acid for the cyclo-oxygenase, leading to decreased synthesis of thromboxane A2, which is a strong platelet agonist, and increases the synthesis of thromboxane A3, which is relatively inactive, so the net effect of high doses of omega-3 fatty acids is platelet inhibition.11,30–32 Table 4 summarizes the clinical uses and recommendations of omega-3 fatty acids.
Side Effects of Omega-3 Fatty Acids
The most commonly observed side effects of omega-3 fatty acid supplementation are nausea, gastrointestinal upset, and a “fishy burp.” The US Food and Drug Administration (FDA) performed a comprehensive review of the safety of fish oil in 1997 and concluded that “consumers not exceed a total of 3 grams per day of EPA and DHA omega-3 fatty acids,” the equivalent of 10 1-g capsules of saturated fish oil (which is 30% DHA + EPA).30–32 Although prolonged bleeding times (present invariably within the normal range) have been noted with very high doses of omega-3 PUFAs (20 g/d), raising a concern for hemorrhagic complications, a recent update by Harris concluded that virtually no increased risk for clinically significant bleeding has been seen in patients with doses of omega-3 fatty acids up to 7 g/d of DHA + EPA, even when combined with aspirin or coumadin.61,62
Omega-3 fatty acid supplementation may increase the level of LDL-C (usually <5%), but this is counterbalanced by its triglyceride-lowering property to the extent of 30% to 50%.2,8–11,63 Another potential danger from high fish intake is the consumption of toxic contaminants, such as methyl mercury. The FDA has recommended that children and pregnant or nursing women avoid mackerel, shark, swordfish, and tilefish, as they are known to often have high mercury levels.64 Fortunately, as mercury is water soluble and protein-bound, it is predominantly localized to muscle tissues and therefore not found in fish oil extractions.65 Fortunately, only negligible amounts of mercury are found in routinely consumed omega-3–rich fish and seafood including shrimp, trout, sardines, salmon, oysters, and herring.66
Treatment Guidelines
We firmly believe that the current evidence strongly supports treatment with omega-3 fatty acids for secondary prevention in patients with CHD and as primary prevention in those with known risk factors for SCD, such as LV dysfunction, LV hypertrophy (LVH), prior MI, or high-grade ventricular arrhythmias. Although there are numerous over-the-counter fish oil supplements with varying amounts of DHA and EPA available on the market, a concentrated prescription omega-3 supplement similar to that used in the GISSI-Prevenzione study has been made available since 2005 (Lovaza, Reliant Pharmaceuticals, Liberty Corner, NJ). At present in the United States, prescription omega-3 fatty acids are approved by the FDA only for the treatment of very high triglyceride levels, and the recommended dose is 3.4 g of DHA + EPA per day, which can reduce triglyceride levels by 30% to 50%.67,68 Lovaza has been shown to reduce severely elevated (>500 mg/dL) triglycerides by 45% and is the only agent to carry this indication at a dose of 4 capsules per day.68,69
The current American Heart Association (AHA) dietary guidelines (Table 5) recommend combined use of EPA and DHA in a dose of approximately 1000 mg per day in patients with CHD.70,71 This dose is derived based on the results from GISSI-Prevenzione study,18 in which a dose of 850 mg was used. For those individuals with no known CHD or hypertriglyceridemia, the AHA recommends the consumption of about 2 oily fish meals per week, which is equivalent to nearly 500 mg of EPA + DHA per day.30,32 Table 6 describes the EPA + DHA content of different kinds of commonly consumed seafood. The most highly consumed fish and shellfish include tuna (representing 22% of total consumption), shrimp (16%), salmon (9%), mixed fish (8%), and crab (7%). Table 7 lists species of fish that are rich in EPA and DHA.72 We have combined data from multiple studies in order to get an assessment of the amount of EPA (or the dose of fish, fish oil, capsules, or cod liver oil) required to inhibit platelets or have positive effects on the blood lipid profile (Table 8).8,11,73
The following are recommendations from major organizations on fish consumption:
The AHA: consume fish, especially oily fish, at least twice a week.70,71
National Cholesterol Education Program (NCEP)—recommends fish as a food item for people to choose more often.74
World Health Organization (WHO)—regular fish consumption, 1 to 2 servings per week; each serving should provide the equivalent of 200 to 500 mg of EPA and DHA.75
European Society of Cardiology—oily fish and omega-3 fatty acids have particular protective properties for primary CV disease prevention.76–78
United Kingdom Scientific Advisory Committee on Nutrition—consume 2 or more portions of fish per week, of which 1 should be oily and provide 450 mg/day of EPA and DHA.79
American Diabetes Association—2 to 3 servings of fish per week provide adequate dietary omega-3 PUFAs.80
Conclusions
Convincingly strong evidence from extensive research over the last 3 decades on the beneficial effects of fish oil therapy mandates that clinicians consider fish oil supplements for primary and secondary CV disease prevention, particularly in patients with high risk for SCD. To reinforce, current recommendations suggest that patients with known CHD should consume about 800–1000 mg/d of combined EPA/DHA, and individuals with no known disease should consume at least 500 mg/d. These doses of EPA/DHA can be obtained by consuming fatty fish or by taking fish oil supplements. Patients with high triglyceride levels will benefit from large doses (3–4 g/d) of EPA/DHA, a dose that almost certainly would require fish oil supplements.
- Academic Division of Ochsner Clinic Foundation








{kind=link}
{kind=link}