Abstract
This article reviews the evolution, growth, and impact of a structured organ recovery program on transplantation in Louisiana and discusses the clinical, social, and financial factors that influence the acceptance of organ transplantation as a viable treatment option for organ failure which once led inexorably to death. The rising number of organ donations and the formulation of strategies to increase these numbers to meet the growing need are examined. Enactment and enforcement of state and federal legislation making organ donation and transplantation available and safer have led to advances in organ donation, procurement, informed consent, and organ preservation, a technology that makes the use of cadaveric organs possible and durable.
Introduction
Very few healthcare treatments can directly trace their success to public support and participation, Transplantation through organ donation is one such unique instance. After the first renal transplant by Dr. Joseph Murray in Boston on December 23, 1954, this revolutionary medical treatment moved from concept through basic laboratory research and prospective randomized clinical trials to acceptance in less than 30 years. Advances in surgical techniques, immunology, immunosuppressive agents, and governmental support account for the local and national growth of the field of transplantation. Often overlooked in this success story is the tale of the gradual acceptance by the public and medical community of the concept of using cadaver organs for the purpose of transplantation.
Legislative History
Those involved in healthcare in the early 1960s realized that for this new treatment to be accepted as a viable clinical option several obstacles had to be overcome. The most obvious were a scarcity of medically suitable organs, overcoming the problem of rejection, and the development of treatments to bridge a patient's care until an organ suitable for transplantation could be found.
Louisiana was a pioneer in the field of organ transplantation. In 1959 the first kidney transplant in the state was performed at Charity Hospital in New Orleans (1,2). This first transplant was a brother-to-brother, living-related, twin transplant. Louisiana physicians were quick to realize that for transplantation to meet the needs of patients with organ failure, a ready source of organs from sources other than living family members was required and initiatives were begun to help resolve this challenge.
In 1967 the National Uniform Anatomical Gift Act (UAGA) was enacted, Louisiana followed with its own version of the UAGA in 1968. This legislation permitted individuals or legally specified next of kin to donate organs and/or tissue at the time of death for the purpose of transplantation. Unfortunately, UAGA legislation was passed in Louisiana and other states with no funding and no plan for educating citizens about their right to donate. As beneficial as this legislation was in the development of the field of transplant surgery, it also initiated a yet-unresolved struggle in the field of organ donation.
The Louisiana UAGA had several unique features. In § R.S. 17:2354.4 the attending physician was defined as the person who determines donor suitability based on accepted medical practice and declares death when organs and/or tissue are to be used for transplant. It also determined that the timing of donor referrals is to be specified by the recovery agency. Louisiana bill § R.S. 911 outlined conditions for the declaration of death in the event of donation, determining that the declaration must be made by a Louisiana-licensed physician with a corroborating opinion by another physician who is not a member of the transplant team. To be declared dead and proceed to burial, only one physician's opinion was needed; to be an organ donor in death two physicians' opinions were required. In 1975 Louisiana added bill § R.S. 32:410 (B) to allow citizens to indicate their intent to donate organs on their driver's license. In R.S. 1299.58.1, the office of the Department of Public Safety and Corrections, through its Office of Motor Vehicles, was told to work with a depository or registry to ensure appropriate dissemination of the driver's decision to donate, again without funding or rules for implementation (1). The 1986 UAGA amendment (§ R.S. 17:2354.4) directed hospital administrators to assure that the option of organ donation was provided to the survivors of patients who died. The Louisiana Secretary of Health and Hospitals was directed to develop and track potential donor referrals, compile an authorized list of recovery agencies, and establish rules to implement donation procedures.
Following the recommendations of the National Commission on Brain Death, and the requirements of other states, Louisiana enacted its Brain Death legislation in 1985 (3). This legislation provided boundaries for donor identification and referral, though only indirectly. In 1993 the UAGA was again amended §R.S. 17:2354.1 (B) to prohibit the coroner, deputy coroner, or any legal representative or agent of the coroner, from authorizing the removal of any organs or tissues in cases in which he may have any financial or economic benefit (2, 4).
Other national legislation also influenced the growth and outcome of donation and transplantation in the state. In 1972, H.R. 1 amended the Social Security Act (Titles XVIII & XIX) and allowed insurance coverage for patients with End Stage Renal Disease (ESRD) and guaranteed payment of 100% of reasonable costs for a transplant and 80% of reasonable costs for dialysis. Anyone eligible for Social Security and/or a dependent with ESRD qualified for coverage. Congress addressed the increasing demand for transplantation and the need to organize donation efforts with the National Organ Transplant Act (NOTA) in 1984. In addition to prohibiting the purchase of organs NOTA provided for the establishment of a national organ sharing system. In § 101 of NOTA the Secretary of Health and Human Services was charged with establishing a Task Force on Organ Transplantation that was to be directed to conduct a comprehensive examination of the medical, legal, ethical, economic, and social issues presented by human organ procurement and transplantation and report its findings to the Secretary. Under § 372 (a) of NOTA the Secretary was directed to establish the Organ Procurement and Transplant Network (OPTN) as a private nonprofit entity to establish a national list of potential organ recipients and to develop a system for matching organs to individuals on the list. The OPTN was also charged with assisting organ procurement organizations in the distribution of organs that could not be placed within their own service areas and with creating and adopting national standards for the acquisition and transportation of donated organs. NOTA became the structure on which a national network was constructed for facilitating the recognition of transplantation as a treatment modality. As a result organ procurement and distribution became recognized medical services.
The 1997 Medicare Conditions of Coverage for organ procurement organizations (OPOs) (FR Vol. 61, No. 86) were published relating performance criteria to maintain provider status. These Rules also mandated adherence to Centers for Disease Control guidelines for screening and testing for donors of human tissue intended for transplantation (FR Vol. 62. No.145).
Also in 1997 the Louisiana legislature enacted Act 99 which directed the state organ recovery agency to offer organs to Louisiana patients first, unless the agency has entered into a mutually beneficial agreement with another state. This legislation was enacted to assure Louisiana patients continued access to transplantation services. This was the first time any state legislature addressed organ allocation. The April 1998 publication of the Final Rule (FR 42 CFR 121) that governs the OPTN, 11 years after the creation of the OPTN and 15 years after the original NOTA legislation, preempted the Louisiana State law and directed the OPTN to develop a new allocation policy giving priority to those whose needs are most urgent, in order to reduce the differences in waiting times for patients of like medical status. This Rule also directs the development of a standardized listing and standardized medical criteria for patients to be listed for transplantation, changes the governance of the OPTN, and directs access to outcomes data. The Department of Health and Human Resources has also published Medicare and Medicaid Programs “Conditions of Participation” (FR Vol. 63. No. 119) which direct hospital relationships with recovery agencies. Specific to this Rule are directives relating to how, when, and who shall establish donor criteria, timeliness of donor referral, and where and how to extend the option of donation to potential donor families. The implementation of this Rule assures that survivors of patients who die in a hospital will be provided the option of donation. It also assures that, as with any other elective procedure, only personnel trained in the process of informed consent for donation will be making the donation request.
Organ Donation: History and Evolution
After Louisiana surgeons performed their first renal transplant, it became apparent that the shortage of organs was a serious impediment to widespread clinical application. The primary source of donor organs, during the first years of transplantation, was family members. Between 1959 and 1970 the ratio of family to cadaver donors was 80/20. The first successful non-related donor renal transplant in Louisiana was performed at Charity Hospital in April 1963. By the time the UAGA was created and the 1972 amendment to the Social Security Act was passed, transplantation was considered a reputable clinical therapy and Louisiana had established its first transplant unit within the Charity Hospital system. In 1971, with funds from the then Department of Health, Education and Welfare, the Metropolitan New Orleans Procurement Program (MNOPP) was founded. The ratio of familial to cadaver donors rose to 50/50 during this time and the patient lists grew faster than anticipated as a result of this emerging source of donors. The factors which influenced the increase in cadaver donations were the enactment of the UAGA, acceptable brain death criteria, implementation of better donor management technologies, a defined approach during the informed consent process, and the development of new organ preservation solutions and treatments (2, 5). With a formal organ recovery program in place, patients from throughout the state were referred for transplantation. The limiting factor in this and other transplant programs was not unique, namely, the barriers of limited supply of donor organs and graft rejection. Between 1971 and 1977, 3 of Louisiana's private, hospitals (Ochsner, Southern Baptist and Hotel Dieu) started transplant programs. All of Louisiana's state hospitals now shared organ recovery services, a tissue matching laboratory, and many surgical team members. As each of the state programs grew, the transplant services became more diverse and the unique needs and varied services offered by each site required more specialized organ recovery and tissue typing, prompting the centers to develop their own organ recovery and laboratory services. Between 1977 and 1987 the 4 organ recovery agencies in the state struggled to meet the demands of growing transplant programs, Transplant leaders in the state re-thought their decision to have separate organ recovery programs and in 1987, with the assistance of the Louisiana Legislature, one of the first statewide OPOs in the country was consolidated within state boundaries (Figure 1). The Louisiana Organ Procurement Agency (LOPA) was the first OPO to have a single statewide organ recipient listing for all patients awaiting a transplant to assist in the allocation of organs. The agency opened 7 offices strategically located throughout the state staffed with coordinators capable of being on-site at a donor facility within 90 minutes of a donor referral. With consolidation, a statewide donor referral hot-line was established and the OPO and eye and tissue banks in the state worked with the State Secretary of Health and Hospitals to develop a statewide education and tracking program to assure compliance to regulations and to maintain a standard of practice.
In 1991 LOPA was able to secure a grant from the National Institutes of Health (NIH) to develop a statewide donor registry. This was the first attempt to implement the 1975 legislation requesting the provision of a functional donor registry to identify potential donors. This statewide registry had a twofold purpose: to identify citizens who had chosen to be donors at the time of death and to track the effectiveness of various education and donor enrollment programs and strategies in the state. In 1992 LOPA complied with a request by key donor hospitals for the development of a single statewide tissue donor service similar to the established organ donor service. By bundling organ and tissue recovery services, the agency's interactions with donor hospitals became more cooperative and well integrated. Within several years of consolidation, LOPA was among the most productive OPOs in the country, consistently providing transplantable organs above the national mean for its population. Anticipating the 1998 Medicare Conditions of Participation (COP) regulations, the OPO, along with the state eye banks, contracted with a medical triage donor referral service to assure donor hospitals of timely responses and prompt determination of the referred patient's donor status.
The success of LOPA and the state transplant centers was symbiotic. The transplant centers, working together, provide expert surgical staff to recover donated organs. Their availability gives recovery efforts the additional edge of local transplant expertise that helps provide a rapid response to donor family and referring hospital needs. This expertise affords a more cost-and resource-efficient recovery effort. The consolidated expertise also gives LOPA the demonstrable advantage of precisely evaluating donors and enables the use of organs refused in previous years, which has increased the number of transplantable organs available to the community by 20% during the past 5 years. Other factors that influenced LOPA's performance during its first 10 years range from skilled problem-solving personnel to the provision of additional services (Figure 2).
Nationally, OPO performance is evaluated by determining the number of organs recovered and the number of organs transplanted. Internally, LOPA's performance is measured by the total numbers of donors referred, as well as the number of medically suitable donors referred, number of consents, number of organ-specific consents, and number of organs transplanted. This evaluation process details each item or task in the donor process and weighs it against the donor potential established by death records and state death statistics per hospital in the state. This detailed measurement allows the OPO to be proactive and innovative in improving donation rates and increasing the availability of organs in the state.
Ethical issues surrounding the transplantation process abound, in particular the appropriateness of the consent process and organ recovery, utilization, and allocation. Figure 3 illustrates the current donor process.

Seven strategically located offices responding to over 29,000 donor referrals annually.
Ethical discussions in the early years of transplantation revolved around the morality of recovering organs from one human donor for the benefit of another human recipient. Is there any benefit to the donor? Continuing research has documented that, for the living donor, knowledge of how the gift has influenced another human being's life or actually preserved that life is satisfying and rewarding, justifying the possible risks and discomforts. Individuals who enroll as donors express a need to leave a “legacy of life,” knowing that their gift, even posthumously, is a meaningful extension of their own life through the gift of life to another. Those who have enrolled in donor registries, signed advanced directives, or have simply told a family member of their desire to donate are expressing the purest form of altruism. They provide selfless gifts without knowledge of outcome, without a possibility of personal advantage, without even a simple thank you. This generosity often overwhelms practitioners. When survivors donate the organs of dead or dying loved ones, it is almost always because “it helped us through our grief to know that a part of him/her lives on in someone else.” Because this action is simultaneously ennobling and comforting, these experiences reported to the community enlarge the circle of willing participants in the donor process by example.
Discussions of ethics begun in the early 1950's continue today because of the struggles within the medical community when dealing with death and dying, informed consent, and patient confidentiality. The right to be a donor, and to be informed of that right, is protected under the law so as not to impose any conflict or compromise in patient care or confidentiality when sharing patient information with organ and tissue recovery agencies.
The education and acceptance of the roles of both medical professionals and the public is an element of the process that continues to evolve. LOPA has integrated into its practice the Louisiana Donor Registry (LADR). With nearly half a million registrants, this pre-enrollment of donors is being used by the OPO and donor hospitals to ease the consent process for the bereaved family.
The linchpin in the donor process is consent. Whether the patient pre-enrolled in the LADR or the family is approached at the time of death, the decision to donate is a difficult one because it comes with the pain of devastating loss. Because of LOPA staff's high consent rate, even when compared with that of health care professionals, our coordinators appear to have an intuitive sense of how to make an approach for consent to donate organs that respects the feelings of survivors. We have begun studies to better understand this process so that we can prepare others to do the same while exercising the same kind of sensitivity, easing the process, and increasing the number of donations.
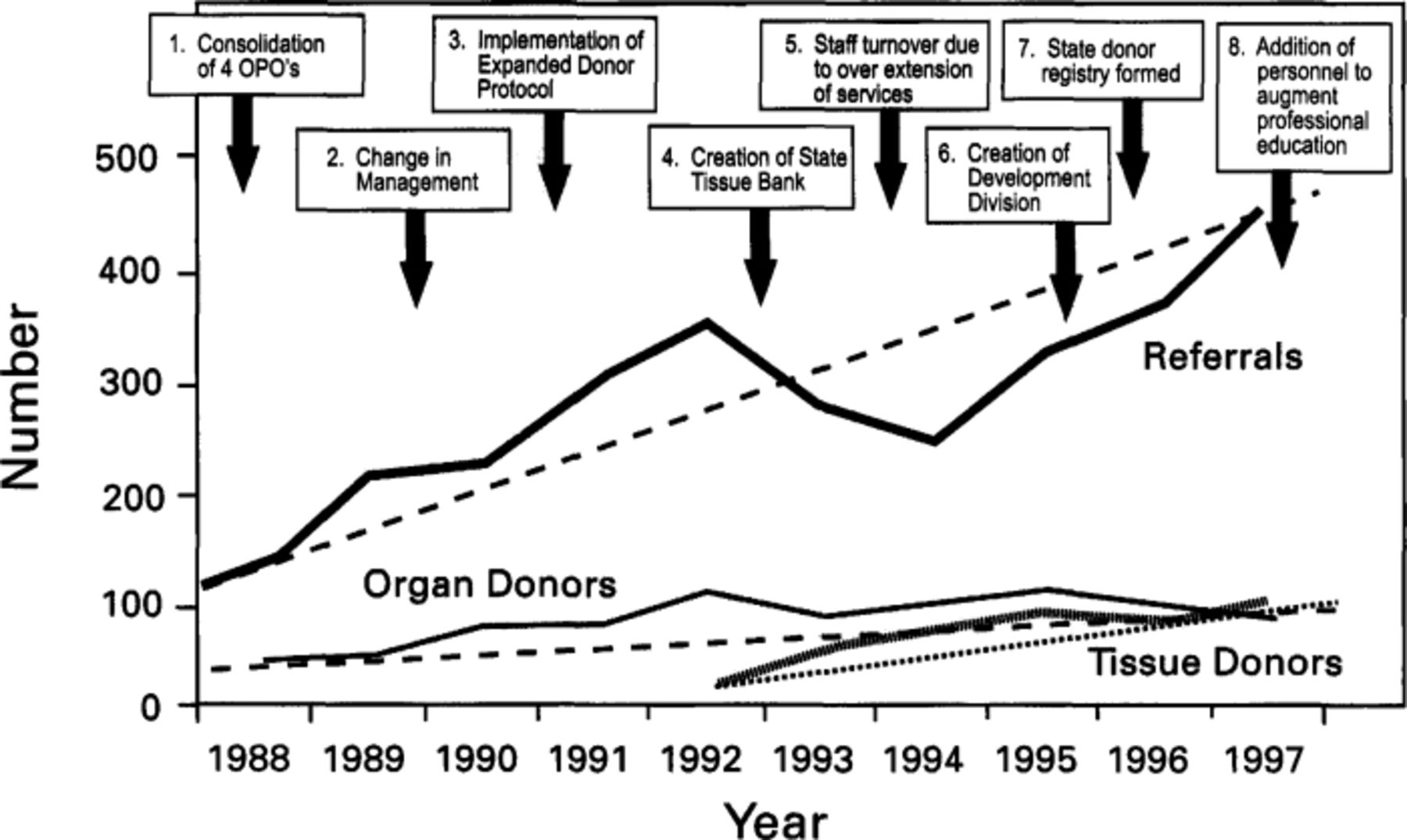
Events influencing increase in donors in Louisiana.
Once consent is obtained the donor process continues by reviewing the patient's medical and social history to identify donor risk factors. All findings in the patient history are relayed to transplant centers at the time the donated organs are offered. After screening the patient history the on-site coordinator, with the assistance of the hospital staff, begins a 5-to 12-hour medical management of the patient. Once a patient is declared dead and accepted as a donor there is a shift in the emphasis of care. With no cerebral function, the evaluation, preservation and viability of the donated organs are now of paramount importance. Physiologic changes are both rapid and subtle after brain death. The medical management goal is to optimize hemodynamic stability to maintain the optimum physiologic state of the donor. Each organ to be donated is monitored, and the donor managed to ensure good perfusion of all organs. Good hydration and stable blood pressure, adequate diuresis, oxygenation, and infection prevention, as well as maintenance of normal temperature are the keys to organ viability. Continuous monitoring of a potential donor allows for immediate management corrections to ensure organ stability.
Organ Preservation
The art of organ preservation has made possible the transplantation of almost every vital human organ (4, 6, 7). Early preservation techniques were quite simple. After the organ was flushed free of donor blood it was placed in a cold saline-like solution at 4 to 6 degrees C and was transplanted within hours of recovery. The current preservation solution, developed by the University of Wisconsin (UW), is intra-cellular, containing hydroxyethyl starch (HES) as its base, which prevents cell swelling and potassium leakage (8, 9, 10). This development in static preservation technique made extended preservation possible and enabled the transplantation of liver, pancreata, hearts, and lungs.
Each organ has an optimal range of preservation time. Cold ischemia time (CIT) is the length of time an organ spends in a cold solution until being re-vascularized in a recipient. Kidneys have a 72-hour window of opportunity and optimal CIT of less than 24 hours. Other organs present a greater challenge and must be transplanted within an 18-hour window. For most organs, particularly the thoracic organs, the optimal CIT time is 4 hours or less.
The OPTN has the responsibility of ensuring procedures that will preserve the viability and assure timely receipt of any type of organ that becomes available. Knowing and assessing the limitations of preservation techniques, the needs and status of the recipient, and the environment in which the donation has occurred, as well as getting each organ to the best-matched recipient, is the job of the OPO.

{kind=link}
{kind=link}
{kind=link}
Donor Process
Organ Allocation
After the normal function of each organ is evaluated, the donor characteristics are listed with the national donor/recipient computer list at the United Network for Organ Sharing (UNOS), the administrative arm of the OPTN which manages the computerized organ-sharing network. The system then matches the donor criteria to the list of potential recipients as stipulated by the recipient physician. The primary match is by blood group and size, and the recipient's requested criteria determine the offer to a waiting patient. Additionally, each patient is assigned a medical priority listing that is used by the OPO to rank allocations. For the past 10 years this ranking has given priority to Louisiana patients, the first offers to the sickest patients, unless LOPA has entered into an agreement that will benefit patients with a potentially better matched organ from another OPO. If no patient matches with a local donor, the organs are then offered to out of state recipients in accordance with medical ranking and national sharing standards. Depending on the degree of urgency, the risk factors and specific organ evaluation issues are weighed by transplant surgeons when considering offers on behalf of their patients. The practice of offering procured organs to local recipients first is one of the reasons LOPA has achieved such success with enrolling the community in the donor process. The community knows that transplantation is accessible to them if they require it and they in turn support the donor program. The agreements made by OPOs to share organs benefit everyone. No transplantable organ is wasted and patients benefit by having access to organs which are optimal matches for them.
With potentially 7 different recipients at 7 different transplant centers, coordinating time, distance, and medical need with matching, surgically recovering, and transporting each donated organ is essential. In Louisiana, time delays and lengthy CIT are alleviated by providing services of local transplant surgeons willing to recover organs for patients of other physicians and transplant centers. This cooperative effort provides excellent donor management, has been effective in lowering the travel and transportation costs of organs, and has lowered organ discard rates. The donor process from referral to organ recovery usually lasts 18 hours with a range of 6 – 36 hours.
Louisiana has seen an increase in demand for transplants to be performed in Louisiana (Table 1). Through its cooperative community efforts, Louisiana has made transplantation available to a population that has historically been labeled as disadvantaged (Table 2). The cooperative relationship between the medical/professional transplant community and the public has increased organ donations and provided shorter waiting times for patients listed in Louisiana (Table 3). The outcome of the proposed new Health and Human Services directive, if implemented, is predicted to decrease the number of transplants available to patients listed at Louisiana centers. This in turn will decrease the number of centers offering transplantation and lead to the subsequent loss of local transplant and organ recovery expertise, and ultimately increase the cost of transplantation. The socio-economically disadvantaged patient will be denied treatment since most do not have portable insurance and cannot afford to travel a great distance to the larger transplant centers and reside in that area prior to and for months after transplantation.
Distribution of organs and tissues by LOPA ranks with the most successful agencies in the country and has helped organ transplantation growth in Louisiana and throughout the U.S.
Comparison of minority and Medicaid patients transplanted in Louisiana
Comparisons of days waiting for patients listed in Louisiana with the national mean. The number of organs recovered in Louisiana and exported to patients at centers outside the state.
Conclusions
A full community partnership is required to offer transplantation services: legislation, timely donor referrals, public participation and support, and a transplant community providing structured access to both donors and donees. The greatest challenge continues to be a shortage of organs that has not kept pace with increasing demand. This imbalance drives the need for standards that assure the equitable rationing of organs. Making transplantation available to more patients requires better public education and a continued concentration on motivating the public to participate in the donor process. The challenges in the development of donor services include generating appropriate and timely referral of patients as donors and cultivating the willingness of the public to consider donation at the time of death.
The donation process mandates consideration of donor criteria, timely donor referral, an informed public willing to donate, consideration for the time-frames of the donor families, and availability of resources at the donor hospital. As newly recognized health care entities, organ and tissue recovery agencies provide a service to the donor by assuring the intent to donate is honored, to the donor family by providing comfort through saving the life of another, and to the medical community by supporting, with technical expertise and organizational skills, the recovery and implanting of viable disease-free organs that can save lives which would once have been characterized by severe disability and death. The organ and tissue recovery programs augment the scope and breadth of medical practice by embracing not only the patient one knows, but all patients, both donors and recipients, and thus the community.
- Academic Division of Ochsner Clinic Foundation
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.