- Lung hernia
- surgical repair
Lung herniation is a rare entity and is usually associated with chest trauma, congenital chest wall defect, or history of thoracotomy. Spontaneous herniation is an even less common event. We report a case of acute respiratory failure caused by spontaneous herniation of the lung that required surgical intervention.
CASE REPORT
A 63-year-old man presented to his primary care physician with a productive cough and dyspnea that had been ongoing for 2 weeks. His past medical history was significant for hypertension, chronic obstructive pulmonary disease (COPD), coronary artery disease, and coronary artery bypass surgery in 1992 and 1998. He also had a 40 pack-year history of tobacco smoking. He was administered antibiotics and oral steroids for a presumed COPD exacerbation. A few days later he presented to a local emergency department with worsening shortness of breath and left-sided chest pain after a vigorous coughing spell. He was intubated for acute respiratory failure associated with hypercapnia and mild hypoxia. A chest radiograph showed a left pleural effusion. He was anemic but hemodynamically stable. He received 2 units of packed red blood cells and was later transferred to our institution for further management.
On examination the patient was intubated and sedated. He had a sternotomy scar with associated left parasternal and lateral chest ecchymosis. Paradoxic motion of the left anterolateral chest wall was seen at the fourth and fifth intercostal spaces. This area was soft to palpation. No crepitus was noted. Breath sounds were audible bilaterally. Imaging studies were obtained (Figures 1–⇓3). Both chest radiograph and computed tomography (CT) scan showed a herniation of the lung in the anterolateral aspect of the left chest.

Chest radiograph showing left lung herniation.

Transverse computed tomography scan image showing lung herniation.
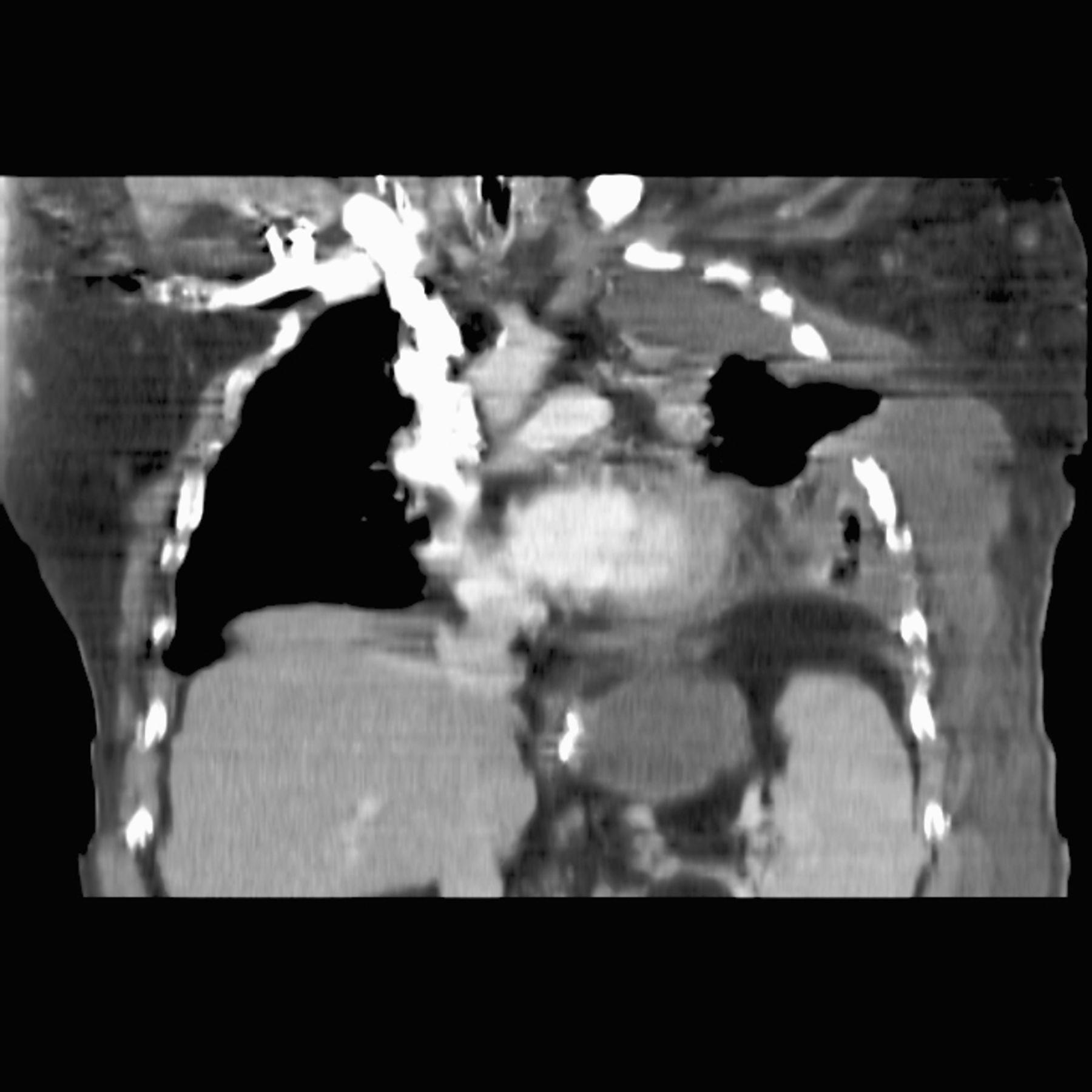
Coronal computed tomography scan image showing lung herniation.
Attempts at weaning the patient off mechanical ventilation with tachypnea and hypoventilation were unsuccessful. He underwent a left lateral thoracotomy. A pleural “hernia sac” was identified in the fourth intercostal space and was continuous with the left pleural space. The main content was the lingula and anterior segment of the left upper lobe. This was mobilized carefully from the chest wall and reduced into the thoracic cavity (Figure 4). A large serosanguinous pleural effusion was drained. The fifth sternochondral junction was found to be dislocated, most likely resulting from the splaying of the ribs. The space between the fourth and fifth ribs was reapproximated using pericostal sternal wires in an interrupted fashion.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Intraoperative photograph showing reduced lung and pleural “hernia sac.” Note use of Weitlaner retractors only between ribs.
Postoperatively, the patient was gradually weaned off mechanical ventilation; he was extubated on postoperative day 2. The chest tube was discontinued appropriately. He was transferred to the surgical floor, and since discharge on day 17 he has done well, with no evidence of recurrence.
DISCUSSION
Extrathoracic lung herniation is protrusion of pleura-covered lung through a defect in the chest wall. Lung herniation was first classified by Morel-Lavallee in 1847.1 These lung herniations have been classified both on the basis of location of the defect (anatomical) or on etiology (Table). The first case of extrathoracic herniation of the lung was reported by Roland in 1499.1 Later observations were made by Hildanus in 1606, Loyseau in 1617, and Plater in 1641. The case described by Felix Plater was reported as probably being the first true lung hernia, with the others being traumatic evicerations.1
Classification of Lung Hernias
Since the Felix Plater case, numerous cases have been reported, mostly related to trauma or dehiscence of a previous thoracotomy. For example, May and associates2 reported anterior traumatic lung herniation due to seatbelt injury.
Spontaneous herniation of the lung is less common and quite rare. Brock and Heitmiller3 have reported 16 cases of spontaneous lung herniation due to vigorous coughing, sneezing, or abnormal motion, without a history of trauma. They noted it was more common in males. Also, one third of the patients were obese, and one half were smokers. Secondary hernias are either congenital or acquired. Congenital herniation occurs because of attenuation of the endothoracic fascia at the thoracic inlet and intercostal spaces. These can also occur with agenesis of ribs, sternum, or costal cartilages. Acquired herniation is usually secondary to trauma or disruption of a prior thoracotomy. It has even been described as occurring with thoracoscopy incisions: These incisions tend to be smaller and inadequately approximated, predisposing them to improper healing and herniation. Pathologic hernias are seen in conjunction with chest wall abscesses, empyema necessitans, malignant tumors, and tuberculous osteomyelitis.4
Spontaneous herniation is most commonly seen in patients with COPD or those with long-term use of steroids. It is most common between the eighth and ninth ribs, where there is reduced muscular support.5
Presentation is usually as a soft swelling with an expansile impulse on coughing. This may be associated with a crepitus.5 The patient may have a history of prior trauma or thoracic surgery. Respiratory failure may occur secondary to paradoxic respiratory movement and is usually associated with very large hernias, as noted in our case. Herniation of the lung apices into the supraclavicular fossa has been described and may cause compression of the subclavian vein and T1 nerve root, causing symptoms.6
Diagnosis is based on clinical presentation and imaging, mainly chest radiograph and CT scan. A chest radiograph may demonstrate larger than normal intercostal spaces and/or extrathoracic lung parenchyma. A CT scan with Valsalva maneuver is helpful in establishing the diagnosis.4
Management
Asymptomatic hernias, especially supraclavicular ones, do not need an intervention. Indications for surgical intervention are enlarging size, difficulty breathing, inability to reduce the hernia, pain, or hemoptysis. Small defects need to be repaired earlier than large defects, as the risk of incarceration is high.
Surgical management of lung herniation, like hernia repair elsewhere, requires reduction of the hernia, excision of the hernia sac, and closure of the defect. Closure of the defect can be performed in several ways, depending on the quality of the regional tissues. Reapproximation of the splayed ribs in a small defect may be performed with pericostal sutures. In larger defects, biologic or prosthetic mesh coverage should be used as it serves to avoid tension on the repair and provide structural integrity. Both underlay and overlay techniques have been described.7,8 Ross and Burnett7 used an underlay polytetrafluoroethylene and overlay polypropylene technique for repair. In a series of 16 patients with spontaneous lung herniation,2 7 cases were repaired primarily and 9 required use of a prosthetic patch.
Meshes such as high-density polyethylene, polytetrafluoroethylene, Vicryl (Ethicon, a Johnson & Johnson company, Sommerville, NJ), and polypropylene may be used. Soft tissue coverage with rotational muscle flaps and omentum may be used when there is inadequate muscle coverage of the defect. Reardon and colleagues9 described a minimally invasive technique using thoracoscopy to reduce the lung hernia. Resection of the herniating lung has also been described for a chronically atelectatic and indurated lung.10 A newly described fixation technique using laminar hooks connected to titanium bars has been described by Wiens et al.11
CONCLUSION
Lung herniation is a rare disease, usually associated with prior trauma or surgery. Spontaneous herniation may occur in patents with COPD with forceful cough or sneeze. When symptomatic, it should be repaired with reduction of the hernia, resection of the sac, and closure of the defect. This may be done either with primary reapproximation of the ribs or use of prosthetic material to cover the defect. Management should be individualized to the patient.
- Academic Division of Ochsner Clinic Foundation