
Abstract
Background
Many ICUs have implemented protocols for tight glucose control, but there are few data on hypoglycemia and neurologic outcomes in patients with subarachnoid hemorrhage (SAH).
Methods
We prospectively ascertained 172 patients with SAH, who were treated according to a standard protocol for target glucose 80–110 mg/dl. Outcomes were assessed with the modified Rankin scale (mRS) at 14 days, 28 days, and 3 months.
Results
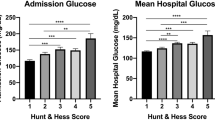
Worse neurologic injury at admission (P < 0.001) and a history of diabetes (P = 0.002) were associated with increased glucose variance. There was lower nadir glucose in patients with radiographic cerebral infarction (81 ± 15 vs. 87 ± 16 mg/dl, P = 0.02), symptomatic vasospasm (78 ± 12 vs. 84 ± 16 mg/dl, P = 0.04) and angiographic vasospasm (79 ± 14 vs. 86 ± 16 mg/dl, P = 0.01), but maximum and mean glucose values were not different. Glucose < 80 mg/dl was earlier and more frequent in patients with worse functional outcome at 3 months (P < 0.001). Progressive reductions in nadir glucose were associated with increasing functional disability at 3 months (P = 0.001) after accounting for neurologic grade and mean glucose. Severe hypoglycemia (<40 mg/dl) occurred in one patient.
Conclusions
In patients with SAH, nadir glucose < 80 mg/dl is associated with cerebral infarction, vasospasm, and worse functional outcomes in multivariate models. Protocols for target glucose 80–110 mg/dl effectively control hyperglycemia, but may place patients with SAH at risk for vasospasm, cerebral infarction, and poor outcome even when severe hypoglycemia does not occur.



Similar content being viewed by others

References
Badjatia N, Topcuoglu MA, Buonanno FS, Smith EE, Nogueira RG, Rordorf GA, et al. Relationship between hyperglycemia and symptomatic vasospasm after subarachnoid hemorrhage. Crit Care Med. 2005;33:1603–9.
Frontera JA, Fernandez A, Claassen J, Schmidt M, Schumacher HC, Wartenberg K, et al. Hyperglycemia after SAH: predictors, associated complications and impact on outcome. Stroke. 2006;37:199–203.
Kruyt ND, Biessels GJ, de Haan RJ, Vermeulen M, Rinkel GJ, Coert B, Roos YB. Hyperglycemia and clinical outcome in aneurysmal subarachnoid hemorrhage. A meta-analysis. Stroke 2009; Epub ahead of print.
Schlenk F, Graetz D, Nagel A, Schmidt M, Sarrafzadeh A. Insulin-related decrease in cerebral glucose despite normoglycemia in aneurysmal subarachnoid hemorrhage. Crit Care. 2008;12:R9.
Bell DA, Strong AJ. Glucose/insulin infusions in the treatment of subarachnoid haemorrhage: a feasibility study. Br J Neurosurg. 2005;19:21–4.
Bilotta F, Spinelli A, Giovannini F, Doronzio A, Delfini R, Rosa G. The effect of intensive insulin therapy on infection rate, vasospasm, neurologic outcome, and mortality in neurointensive care unit after intracranial aneurysm clipping in patients with acute subarachnoid hemorrhage: a randomized prospective pilot trial. J Neurosurg Anesthesiol. 2007;19:156–60.
Latorre JG, Chou SH, Nogueira RG, Singhal AB, Carter BS, Ogilvy CS, et al. Effective glycemic control with aggressive hyperglycemia management is associated with improved outcome in aneurysmal subarachnoid hemorrhage. Stroke. 2009;40:1644–52.
Wiener RS, Wiener DC, Larson RJ. Benefits and risks of tight glucose control in critically ill adults: A meta-analysis. JAMA. 2008;300:933–44.
Thiele RH, Pouratian N, Zuo Z, Scalzo DC, Dobba HA, Dumont AS, et al. Strict glucose control does not affect mortality after aneurysmal subarachnoid hemorrhage. Anesthesiology. 2009;110:603–10.
The Nice-Sugar Study Investigators. Intensive versus conventional glucose control in critically patients. New Engl J Med 2009;360:1283–97.
Ali NA, O’Brien JMJ, Dungan K, Phillips G, Marsh CB, Lemeshow S, et al. Glucose variability and mortality in patients with sepsis. Crit Care Med. 2008;36:2316–21.
Egi M, Bellomo R, Stachowski E, French C, Hart G. Variability of blood glucose concentration and short-term mortality in critically ill patients. Anesthesiology. 2006;105:244–52.
Schlenk F, Vajkoczy P, Sarrafzadeh A. Inpatient hyperglycemia following aneurysmal subarachnoid hemorrhage: Relation to cerebral metabolism and outcome. Neurocrit Care 2009; Epub ahead of print.
Schlenk F, Nagel A, Graetz D, Sarrafzadeh A. Hyperglycemia and cerebral glucose in aneurysmal subarachnoid hemorrhage. Intensive Care Med. 2008;34:1200–7.
Vespa P, Boonyaputthikul R, McArthur DL, Miller C, Etchepare M, Bergsneider M, et al. Intensive insulin therapy reduces microdialysis glucose values without altering glucose utilization or improving the lactate/pyruvate ratio after traumatic brain injury. Crit Care Med. 2006;34:850–6.
Classen J, Vu A, Kreiter KT, Kowalski RG, Du EY, Ostapkovich N, et al. Effect of acute physiologic derangements on outcome after subarachnoid hemorrhage. Crit Care Med. 2004;32:832–8.
Tseng M-Y, Czosnyka M, Richards H, Pickard JD, Kirkpatrick PJ. Effects of acute treatment with pravastatin on cerebral vasospasm, autoregulation, and delayed ischemic deficits after aneurysmal subarachnoid hemorrhage: a phase 2 randomized placebo-controlled trial. Stroke. 2005;36:1627–32.
Sen J, Belli A, Albon H, Morgan L, Petzold A, Kitchen N. Triple-h therapy in the management of aneurysmal subarachnoid haemorrhage. Lancet Neurol. 2003;2:614–21.
Naidech A, Jovanovic B, Wartenberg K, Parra A, Ostapkovich N, Connolly E, et al. Higher hemoglobin is associated with improved outcome after subarachnoid hemorrhage. Crit Care Med. 2008;35:2383–9.
Rabinstein AA, Weigand S, Atkinson JLD, Wijdicks EFM. Patterns of cerebral infarction in aneurysmal subarachnoid hemorrhage. Stroke. 2005;36:992–7.
Banks J, Marotta C. Outcomes validity and reliability of the modified Rankin scale: implications for stroke clinical trials: a literature review and synthesis. Stroke. 2007;38:1091–6.
Wilson JTL, Hareendran A, Grant M, Baird T, Schulz UGR, Muir KW, et al. Improving the assess of outcomes in stroke. Use of a structured interview to assign grade on the modified Rankin scale. Stroke. 2002;33:2243–6.
Krinsley JS, Grover A. Severe hypoglycemia in critically ill patients: risk factors and outcomes. Crit Care Med. 2007;35:2262–7.
Krinsley JS. Glycemic variability: a strong independent predictor of mortality in critically ill patients. Crit Care Med. 2008;36:3008–13.
Egi M, Bellomo R, Stachowski E, French C, Hart G, Hegarty C, et al. Blood glucose concentration and outcome of critical illness: the impact of diabetes. Crit Care Med. 2008;36:2249–55.
Inzucchi SE, Siegel MD. Glucose control in the icu—how tight is tight enough? New Engl J Med. 2009;360:1346–8.
Acknowledgments
This work was departmentally funded. The authors acknowledge the team at the Enterprise Data Warehouse who built the portal for electronic retrieval of laboratory and medication data. The Enterprise Data Warehouse is a joint project of Northwestern Memorial Hospital, Northwestern University, and the Northwestern Memorial Faculty Foundation. More information is available at www.edw.northwestern.edu.
Conflict of Interest Statement
AMN has received past grant support from the Neurocritical Care Society, NovoNordisk, and the Northwestern Memorial Foundation, and current grant support from Gaymar Inc and Astellas Pharma US for unrelated work. AMN has received past speaker fees from EKR Therapeutics (ended 2008). It is unclear how these might relate to this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Naidech, A.M., Levasseur, K., Liebling, S. et al. Moderate Hypoglycemia is Associated With Vasospasm, Cerebral Infarction, and 3-Month Disability After Subarachnoid Hemorrhage. Neurocrit Care 12, 181–187 (2010). https://doi.org/10.1007/s12028-009-9311-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-009-9311-z