
Abstract
BACKGROUND: Limited information is available on preoperative status and risks for complications for older patients having surgery for hip fracture. Our objective was to identify potentially modifiable clinical findings that should be considered in decisions about the timing of surgery.
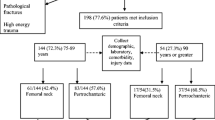
METHODS: We conducted a prospective cohort study with data obtained from medical records and through structured interviews with patients. A total of 571 adults with hip fracture who were admitted to 4 metropolitan hospitals were included.
RESULTS: Multiple logistic regression was used to identify risk factors (including 11 categories of physical and laboratory findings, classified as mild and severe abnormalities) for in-hospital complications. The presence of more than 1 (odds ratiol [OR] 9.7, 95% confidence interval [CI] 2.8 to 33.0) major abnormality before surgery or the presence of major abnormalities on admission that were not corrected prior to surgery (OR 2.8, 95% CI 1.2 to 6.4) was independently associated with the development of postoperative complications. We also found that minor abnormalities, while warranting correction, did not increase risk (OR 0.70, 95% CI 0.28 to 1.73).
CONCLUSIONS: In this study of older adults undergoing urgent surgery, potentially reversible abnormalities in laboratory and physical examination occurred frequently and significantly increased the risk of postoperative complications. Major clinical abnormalities should be corrected prior to surgery, but patients with minor abnormalities may proceed to surgery with attention to these medical problems perioperatively.
Similar content being viewed by others


References
Palda VA, Detsky AS. Perioperative assessment and management of risk from coronary artery disease. Ann Intern Med. 1997;127:313–28.
Lee TH, Marcantonio ER, Mangione CM, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation. 1999;100:1043–9.
Detsky AS, Abrams HB, McLaughlin JR, et al. Predicting cardiac complications in patients undergoing noncardiac surgery. J Gen Intern Med. 1986;1:211–9.
Eagle KA, Berger PB, Calkins H, et al. ACC/AHA guideline update for perioperative cardiovascular evaluation for noncardiac surgery. Circulation. 2002;10:1257–67.
Goldman L, Caldera DL, Nussbaum SR, et al. Multifactorial index of cardiac risk in noncardiac surgical procedures. N Engl J Med. 1977;297:845–50.
White RH, Roman PS, Zhou H, Rogrigo J, Bargar W. Incidence and time course of thromboembolic outcomes following total hip or knee arthroplasty. Arch Intern Med. 1998;158:1525–31.
Polanczyk CA, Marcantonio E, Goldman L, et al. Impact of age on perioperative complications and length of stay in patients undergoing noncardiac surgery. Ann Intern Med. 2001;134:637–43.
Zuckerman JD, Skovron ML, Koval KJ, et al. Postoperative complications and mortality associated with operative delay in older patients who have a fracture of the hip. J Bone J Surg. 1995;77-A:10.
Dolk T. Hip fractures—treatment and early complications. Upsala J Med Sci. 1989;94:195–207.
Johnstone DJ, Morgan NH, Wilkinson C, Chissell HR. Urinary tract infection and hip fracture. Injury. 1995;26:2.
Ochs M. Surgical management of the hip in the elderly patient. Clin Geriatr Med. 1990;6:571–87.
Lu-Yao GL, Baron JA, Barrett JA, Fischer ES. Treatment and survival among elderly Americans with hip fractures: a population-based study. Am J Pub Health. 1994;84:1287–91.
Magaziner J, Simonsick EM, Kashner TM, Hebel JR, Kenzora JE. Predictors of functional recovery one year following hospital discharge for hip fracture: a prospective study. J Gerontol. 1990;45:M101–7.
Hannan EL, Magaziner J, Wang JJ, et al. Mortality and locomotion 6 months after hospitalization for hip fracture: risk factors and risk adjusted hospital outcomes. JAMA. 2001;285:2736–42.
Inouye SK, van Dyck CH, Alessi CA, Balkin S, Siegal AP, Horwitz RI. Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Intern Med. 1990;113:941–8.
Kahn KL, Rogers WH, Rubenstein LV, et al. Measuring quality of care with explicit process criteria before and after implementation of the DRG-based prospective payment system. JAMA. 1990;264:1969–73.
Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13:818–29.
Dodds TA, Martin DP, Stolov WC, Deyo RA. A validation of the functional independence measure and its performance among rehabilitation inpatients. Arch Phys Med Rehabil. 1993;74:531–6.
Carson JL, Duff A, Berlin JA, et al. Perioperative blood transfusion and postoperative mortality. JAMA. 1998;279:199–205.
Myers AN, Robinson EG, Van Natta ML, Michelson JD, Collins K, Baker SP. Hip fractures among the elderly: factors associated with inhospital mortality. Am J Epidemiol. 1991;134:1128–37.
Miller K, Atzenhofer K, Gerber G, Reichel M. Risk prediction in operatively treated fractures of the hip. Clin Orthop Relat Res. 1993;293:148–52.
Arozullah AM, Khuri SF, Henderson WH, Daley J, for the Participants in the National Veterans Affairs Surgical Quality Improvement Program. Development and validation of a multifactorial risk index for predicting postoperative pneumonia after major noncardiac surgery. Ann Intern Med. 2001;135:847–57.
Magaziner J, Simonsick EM, Kashner TM, Hebel JR, Kenzora JE. Survival experience of aged hip fracture patients. Am J Public Health. 1989;79:274–8.
Ceder L, Elmqvist D, Svensson SE. Cardiovascular and neurological function in elderly patients sustaining a fracture of the neck of the femur. J Bone J Surg Br. 1981;63B:560–6.
Hoerer D, Volpin G, Stein H. Results of early and delayed surgical fixation of hip fractures in the elderly: a comparative retrospective study. Bull Hosp Jt Dis. 1993;53:29–33.
Lawrence VA, Hilsenbeck SG, Noveck H, Poses RM, Carson JL. Medical complications and outcomes after hip fracture repair. Arch Intern Med. 2002;162:2053–7.
Browner WS, Li J, Mangano DT. In hospital and long-term mortality in male veterans following noncardiac surgery. JAMA. 1992;268:228–32.
Farrow SC, Fowkes FG, Lunn JN, Robertson IB, Samuel P. Epidemiology in anaesthesia, II: factors affecting mortality in hospital. Br J Anaesth. 1982;54:811–7.
Versluysen M. How elderly patients with femoral fracture develop pressure sores in hospital. BMJ. 1986;292:1311–3.
Orosz GM, Magaziner J, Hannan EL, et al. Association of timing of surgery for hip fracture and patient outcomes. JAMA. 2004;291:1738–43.
Hirsch CH. Caring for the older surgical patient: special considerations. Primary Care Rep. 1996;2:191–200.
Reiss R, Deutsch A, Nudelman I. Surgical problems in octogenarians: epidemiological analysis of 1083 consecutive admissions. World J Surg. 1992;16:1017–20.
Gibson JR, Mendenhall MK, Axel NJ. Geriatric anesthesia: minimizing the risk. Clin Geriatr Med. 1985;1:313–21.
Author information
Authors and Affiliations
Corresponding author
Additional information
The authors have no conflicts of interest to declare for this article.
This project was supported in part by grants from the Agency for Healthcare Research and Quality (U18HS09459-0), The Mary and David Hoar Program of the New York Academy of Medicine (McLaughlin), the National Institute on Aging (Midcareer Investigator Award to Dr. Siu and Mentored Clinical Scientist Development Award to Dr. Morrison), and the American Federation for Aging Research Paul Beeson Faculty Scholar Award (Dr. Morrison).
Rights and permissions
About this article
Cite this article
McLaughlin, M.A., Orosz, G.M., Magaziner, J. et al. Preoperative status and risk of complications in patients with hip fracture. J Gen Intern Med 21, 219–225 (2006). https://doi.org/10.1111/j.1525-1497.2006.00318.x
Received:
Revised:
Accepted:
Issue Date:
DOI: https://doi.org/10.1111/j.1525-1497.2006.00318.x