
Abstract
Trastuzumab is a monoclonal antibody that targets the human epidermal growth factor receptor tyrosine kinase HER2/ErbB2. This agent has shown a highly significant antitumour effect for patients with HER2-positive breast cancer, and is now considered part of the standard regimens for the treatment of this disease in both the metastatic and adjuvant setting.
Cardiotoxicity has been associated with trastuzumab, and this issue has now been studied and documented in a number of adjuvant trials for which data have now been released. Cardiotoxicity has been shown to be potentiated when the agent is used concurrently or sequentially with an anthracycline, and this has limited the use of trastuzumab in some patients. Determining the overall impact of trastuzumab is further complicated by the administration of other cardiotoxic agents such as the taxanes and cyclophosphamide as well as by pre-existing cardiac disease.
The incidence of severe congestive heart failure (New York Heart Association class III or IV) was 0–3.9% in the trastuzumab arms versus 0–1.3% in the control arms in the five major randomized adjuvant trials. Only one cardiac death was related to trastuzumab whereas two cardiac deaths occurred in the control arms. Ejection fraction decline of ≥10% or 15% was reported in 3–34% of trastuzumab recipients in these trials.
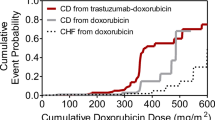
Patients affected by trastuzumab-related cardiotoxicity do not exhibit the cellular death and distinctive ultrastructural myocardial changes seen on electron microscopy with anthracycline-induced cardiotoxicity. The cardiotoxicity of trastuzumab also differs from traditional chemotherapy-induced cardiotoxicity in that it appears to be at least partially reversible, not related to the cumulative dose, and re-challenge is generally tolerated.
There remain a number of uncertainties regarding the diagnosis and management of trastuzumab-related cardiotoxicity. While no formal guidelines or consensus statements exist at present regarding cardiac monitoring during use of trastuzumab, proposed recommendations include a careful assessment of ejection fraction prior to initiating trastuzumab, avoidance of concurrent administration of trastuzumab with anthracyclines, and regular monitoring of symptoms and cardiac function during and for several years after therapy. Increased vigilance is appropriate for higher risk patients.




Similar content being viewed by others

Notes
1This terminology was originally suggested by Dr Lynne W. Stevenson, Boston, MA, USA (personal communication)
References
Nahta R, Esteva F. HER2 therapy: molecular mechanisms of trastuzumab resistance. Breast Cancer Res 2006; 8: 215
Romond EH, Perez EA, Bryant J, et al. Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N Engl J Med 2005; 353: 1673–84
Slamon DJ, Eiermann W, Robert N, et al. Phase III randomized trial comparing doxorubicin and cyclophosphamide followed by docetaxel (ACT) with doxorubicin and cyclophosphamide followed by docetaxel and trastuzumab (ACTH) with docetaxel, carboplatin and trastuzumab (TCH) in HER2-positive early breast cancer patients: BCIRG 006 study [abstract]. Breast Cancer Res Treat 2005; 94: S5
Joensuu H, Kellokumpu-Lehtinen P, Bono P, et al. Adjuvant docetaxel or vinorelbine with or without trastuzumab for breast cancer. N Engl J Med 2006; 354: 809–20
Piccart-Gebhart MJ, Proctor M, Leyland-Jones B, et al. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med 2005; 353: 1659–72
Slamon D, Leyland-Jones B, Shak S, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med 2001; 344(11): 783–92
Seidman A, Hudis C, Pierri MK, et al. Cardiac dysfunction in the trastuzumab clinical trials experience. J Clin Oncol 2002; 20: 1215–21
Tan-Chiu E, Yothers G, Romond E, et al. Assessment of cardiac dysfunction in a randomized trial comparing doxorubicin and cyclophosphamide followed by paclitaxel, with or without trastuzumab as adjuvant therapy in node-positive, human epidermal growth factor receptor 2-overexpressing breast cancer: NSABP B31. J Clin Oncol 2005; 23: 7811–9
Rastogi P, Jeong J, Geyer CE, et al. Five-year update of cardiac dysfunction on NSABP B-31, a randomized trial of sequential doxorubicin/cyclophosphamide →> paclitaxel compared to AC → T with trastuzumab: LBA 513 [abstract]. In: ASCO 43rd Annual Meeting; 2007 Jun 1–5; Chigaco (IL). J Clin Oncol 2007; 25 (18S Part I): 6s
Suter TM, Proctor M, van Veldhuisen DJ, et al. Trastuzumab-associated cardiac adverse effects in the Herceptin Adjuvant trial. J Clin Oncol 2007; 25: 3859–65
Slamon D, Eierman W, Robert N, et al. BCIRG 006: 2nd interim analysis phase III randomized trial comparing doxorubicin and cyclophophamide followed by docetaxel (ACT) with docetaxel, carboplatin and trastuzumab (TCH) in HER2neu positive early breast cancer patients [abstract]. 29th Annual San Antonio Breast Cancer Symposium; 2006 Dec 14–17; San Antonio (TX)
Billingham M. Role of endomyocardial biopsy in diagnosis and treatment of heart disease. In: Silver M, editor. Cardiovascular pathology. New York: Churchill Livingstone, 1991: 1465–8
Ewer MS, Vooletich MT, Durand JB, et al. Reversibility of trastuzumab-related cardiotoxicity: new insights based on clinical course and response to medical treatment. J Clin Oncol 2005; 23: 7820–7
Perez EA, Suman VJ, Davidson NE, et al. Cardiac safety analysis of doxorubicin and cyclophosphamide followed by paclitaxel with or without trastuzumab in the North Central Cancer Treatment Group N9831 adjuvant breast cancer trial. J Clin Oncol 2008; 26: 1231–8
Ewer MS, Lenihan DJ. Left ventricular ejection fraction and cardiotoxicity: is our ear really to the ground? J Clin Oncol 2008; 26: 1201–3
Ewer M, Lippman S. Type II chemotherapy-related cardiac dysfunction: time to recognize a new entity. J Clin Oncol 2005; 23(13): 2900–2
Telli ML, Hunt MA, Carlson RW, et al. Trastuzumab-related cardiotoxicity: calling into question the concept of reversibility. J Clin Oncol 2007; 25: 3525–33
Ewer MS, Tan-Chiu E. Reversibility of trastuzumab cardiotoxicity: is the concept alive and well [letter]? J Clin Oncol 2007; 25: 5532–3
Gille L, Nohl H. Analysis of the molecular mechanism of adriamycin-induced cardiotoxicity. Free Radic Biol Med 1997; 23: 775–82
Herman EH, Zhang J, Hasinoff BB, et al. Comparison of the protective effects against chronic doxorubicin cardiotoxicity and the rates of iron (III) displacement reactions of ICRF-187 and other bisdiketopiperazines. Cancer Chemother Pharmacol 1997; 40: 400–8
Zhao YY, Baliga RR, Opel DJ, et al. Neuregulins promote survival and growth of cardiac myocytes: persistence of ErbB2 and ErbB4 expression in neonatal and adult ventricular myocytes. J Biol Chem 1998; 273: 10261–9
Clerk A, Michael A, Sugden P. Stimulation of the p38 mitogen-activated protein kinase pathway in neonatal rat ventricular myocytes by the G protein-coupled receptor agonists, endothe-lin-1 and phenylephrine: a role in cardiac myocyte hypertrophy? J Cell Biol 1998; 142(2): 523–35
Suter T, Cook-Bruns N, Barton C. Cardiotoxicity associated with trastuzumab (Herceptin) therapy in the treatment of metastatic breast cancer. Breast 2004 Jun; 13(3): 173–83
Crone S, Zhao YY, Fan L, et al. ErbB2 is essential in the prevention of dilated cardiomyopathy. Nature Med 2002; 8: 459–65
de Korte MA, de Vries EG, Lub-de Hooge MN, et al. 111 Indium-trastuzumab visualises myocardial human epidermal growth factor receptor 2 expression shortly after anthracycline treatment but not during heart failure: a clue to uncover the mechanisms of trastuzumab-related cardiotoxicity. Eur J Cancer 2007; 20: 46–51
Bryant J, Picot J, Baxter L, et al. Use of cardiac markers to assess the toxic effects of anthracyclines given to children with cancer: a systematic review. Eur J Cancer 2007; 43: 1959–66
Aggarwal S, Pettersen MD, Bhambhani K, et al. B-Type natri-uretic peptide as a marker for cardiac dysfunction in anthra-cycline-treated children. Ped Blood Cancer 2007; 49: 812–6
Ewer MS, Perez EA, Baselga J, et al. Cardiac safety guidelines for the adjuvant use of trastuzumab (Herceptin) in HER2-positive early breast cancer [poster no. 176]. St Gallen Primary Therapy of Early Breast Cancer 10th International Conference; 2007 Mar 14–17; St Gallen, Switzerland
Ewer M, Yeh ET. Cancer and the heart. Hamilton, Ontario: Decker, 2006
Acknowledgements
No sources of funding were used to assist in the preparation of this review. Dr Steven Ewer has no conflicts of interest that are relevant to the content of this review. Dr Michael Ewer has been a speaker and has received honoraria from F. Hoffman La Roche, sanofi-aventis and Novartis; he has no equity interest in any pharmaceutical entity.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ewer, S.M., Ewer, M.S. Cardiotoxicity Profile of Trastuzumab. Drug-Safety 31, 459–467 (2008). https://doi.org/10.2165/00002018-200831060-00002
Published:
Issue Date:
DOI: https://doi.org/10.2165/00002018-200831060-00002