Article Text

Summary
Allergic bronchopulmonary aspergillosis (ABPA) is a pulmonary disorder resulting from immune responses directed against inhaled Aspergillus fumigatus antigens. It manifests with poorly controlled asthma, fleeting pulmonary opacities and structural lung damage in the form of bronchiectasis. Initially defined in individuals suffering from bronchial asthma and cystic fibrosis, it has also been described in patients with other structural lung disorders such as chronic obstructive pulmonary disease, pulmonary tuberculosis, idiopathic bronchiectasis and others. Kartagener syndrome is a manifestation of primary ciliary dyskinesia characterised by the presence of dextrocardia, bronchiectasis and chronic sinusitis. We report a case of ABPA in an adult suffering from Kartagener syndrome. We also performed a systematic review of the literature on the association between Kartagener syndrome and ABPA.
Statistics from Altmetric.com
Background
Allergic bronchopulmonary aspergillosis (ABPA) is a pulmonary manifestation secondary to immunological reactions mounted against antigens of Aspergillus fumigatus colonising the airways.1 ,2 The disorder clinically manifests with low-grade fever, productive cough, wheezing and uncontrolled asthma.3 ABPA is a fairly common disease with a global burden of about 5 million,4 and an estimated burden of 1.38 million individuals in India alone.5 The diagnosis of ABPA is made on a combination of clinical, radiological and immunological criteria, in a predisposed individual (bronchial asthma and cystic fibrosis (CF)).6 Apart from bronchial asthma and CF, ABPA has also been observed in other lung diseases including chronic obstructive pulmonary disease (COPD), post-tubercular fibrocavitary disease, HIV syndrome, bronchiectasis and others.7–12 Kartagener syndrome is a variant of primary ciliary dyskinesia (PCD),13 and presents with the classic triad of sinusitis, bronchiectasis and situs inversus. It is a rare disease with an estimated incidence of 1 per 30 000 births. Organ laterality defects are encountered in roughly 50% of cases, thus the incidence of PCD is about 1 in 10 000 to 20 000 births.14 We describe a report of ABPA in a patient with Kartagener syndrome. We also perform a systematic review of the literature for this association.
Case presentation
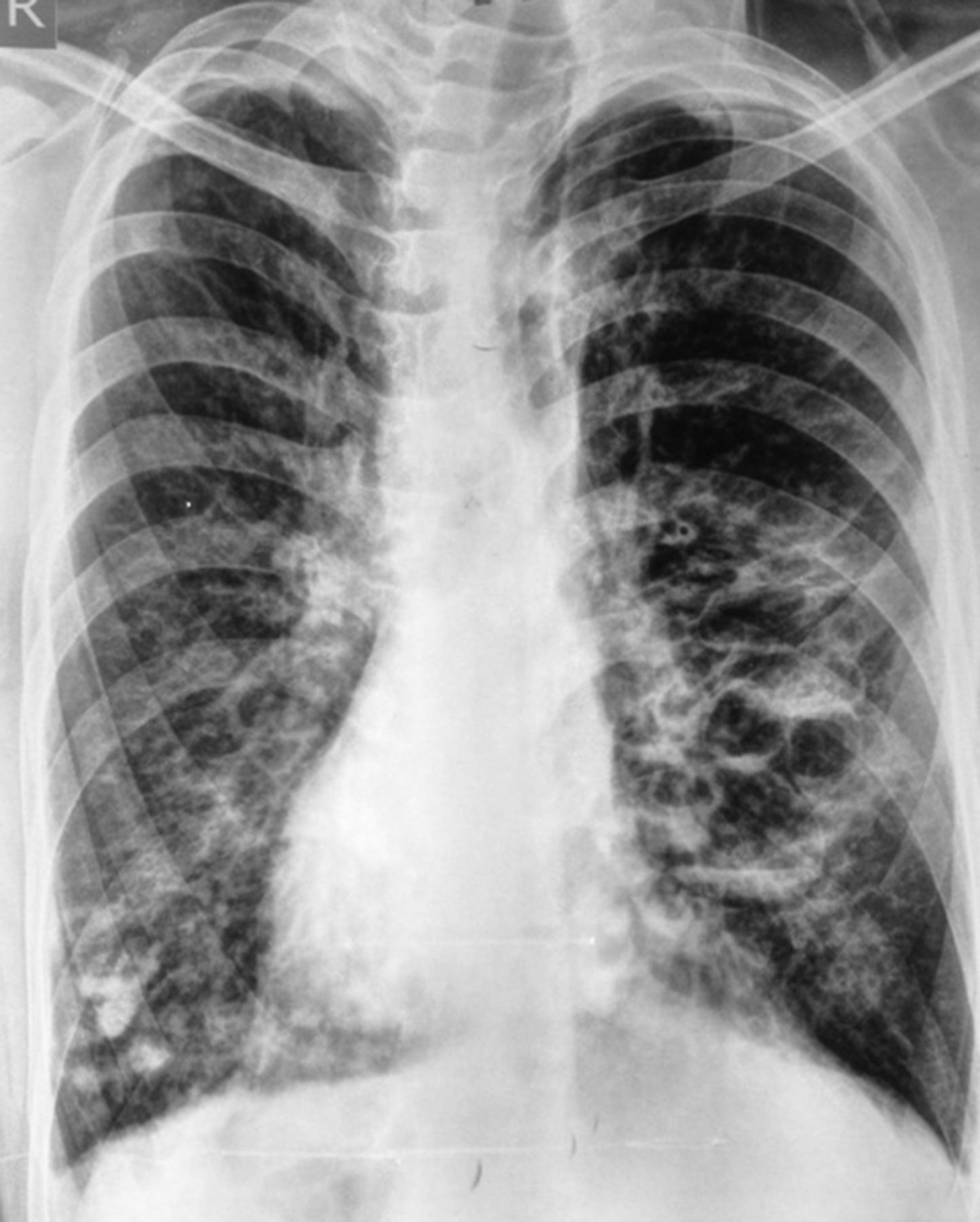
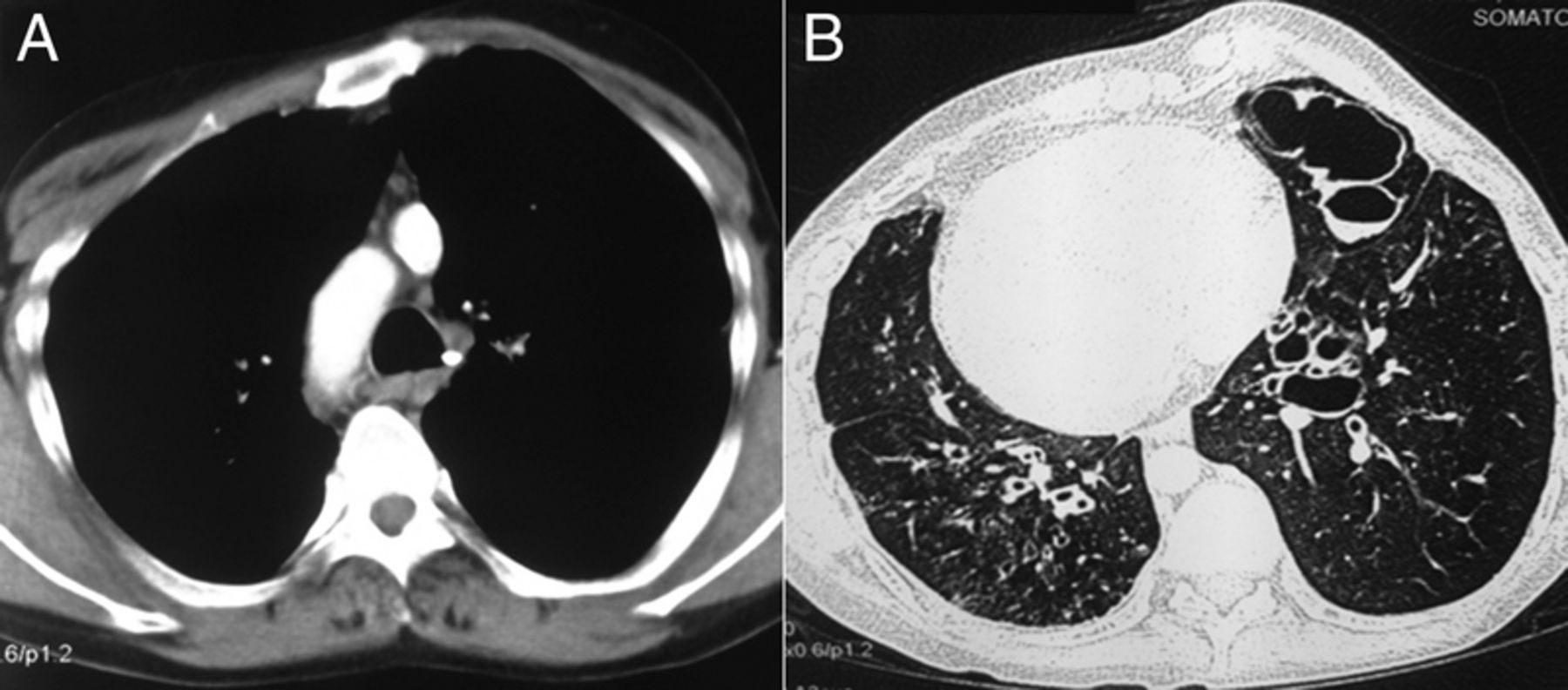
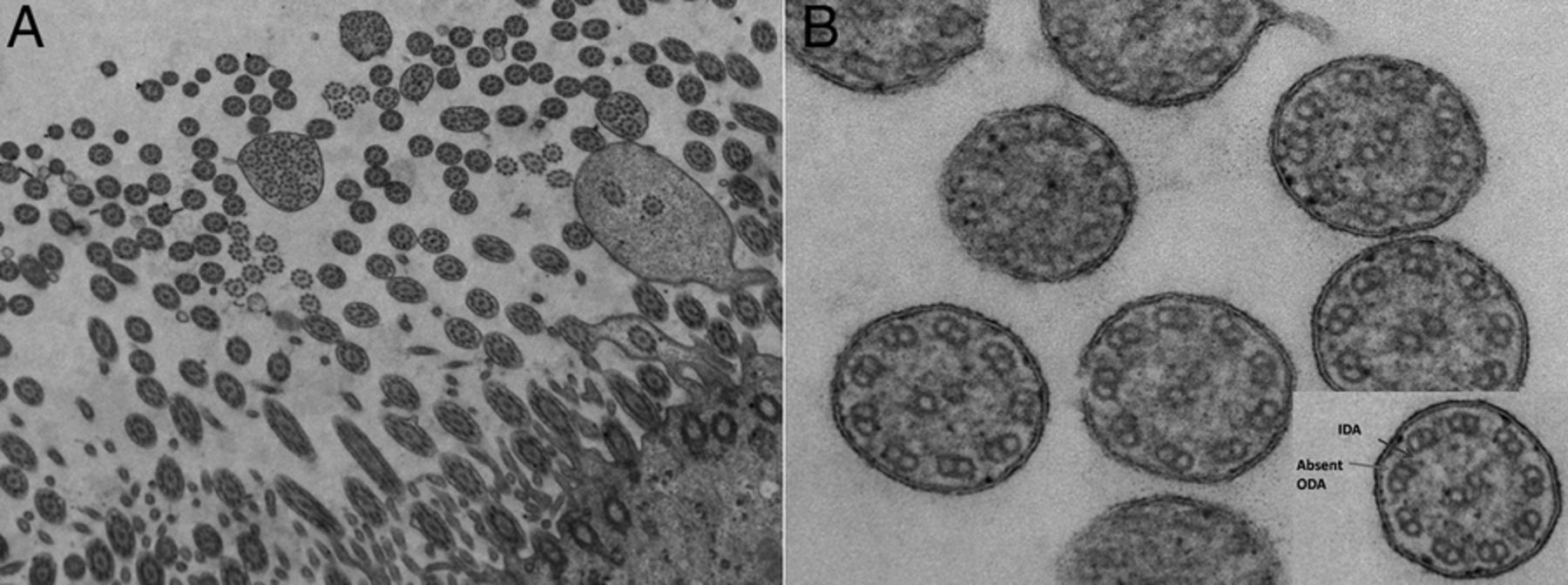
A 31-year-old man presented with a history of cough with mucoid expectoration, breathlessness and wheezing since childhood. His symptoms were punctuated by recurrent episodes of exacerbations associated with an increase in cough, purulent expectoration, haemoptysis and breathlessness. The patient also reported nasal stuffiness, nasal obstruction and epistaxis since childhood. Auscultation of the chest revealed polyphonic wheeze associated with diffusely scattered coarse crackles. Spirometry showed an obstructive pattern without bronchodilator reversibility. Chest radiography revealed dextrocardia along with bronchiectasis (figure 1). Contrast-enhanced and high-resolution CT of the thorax revealed bronchiectasis (with mucus impaction) and situs inversus (figure 2). Sweat chloride was normal. A possibility of primary ciliary dysfunction/Kartagener syndrome was considered. Semen analysis revealed azoospermia (table 1). Biopsy of tracheal mucosa was performed using flexible bronchoscopy. Electron microscopic examination of the tracheal mucosa revealed ultrastructural defect in the respiratory cilia (absent dynein in the outer ring arm of the microtubule), thereby confirming the diagnosis of Kartagener syndrome (figure 3). Evaluation was performed for ABPA, and the diagnosis was confirmed on the basis of elevated total and A. fumigatus-specific IgE, peripheral blood eosinophilia and immediate cutaneous hyper-reactivity against A. fumigatus antigen. CT of the paranasal sinuses was also conducted, which revealed only mucosal thickening with no clear suggestion of allergic fungal sinusitis.
Baseline investigations

Chest radiograph showing dextrocardia and bilateral cystic opacities consistent with bronchiectasis.
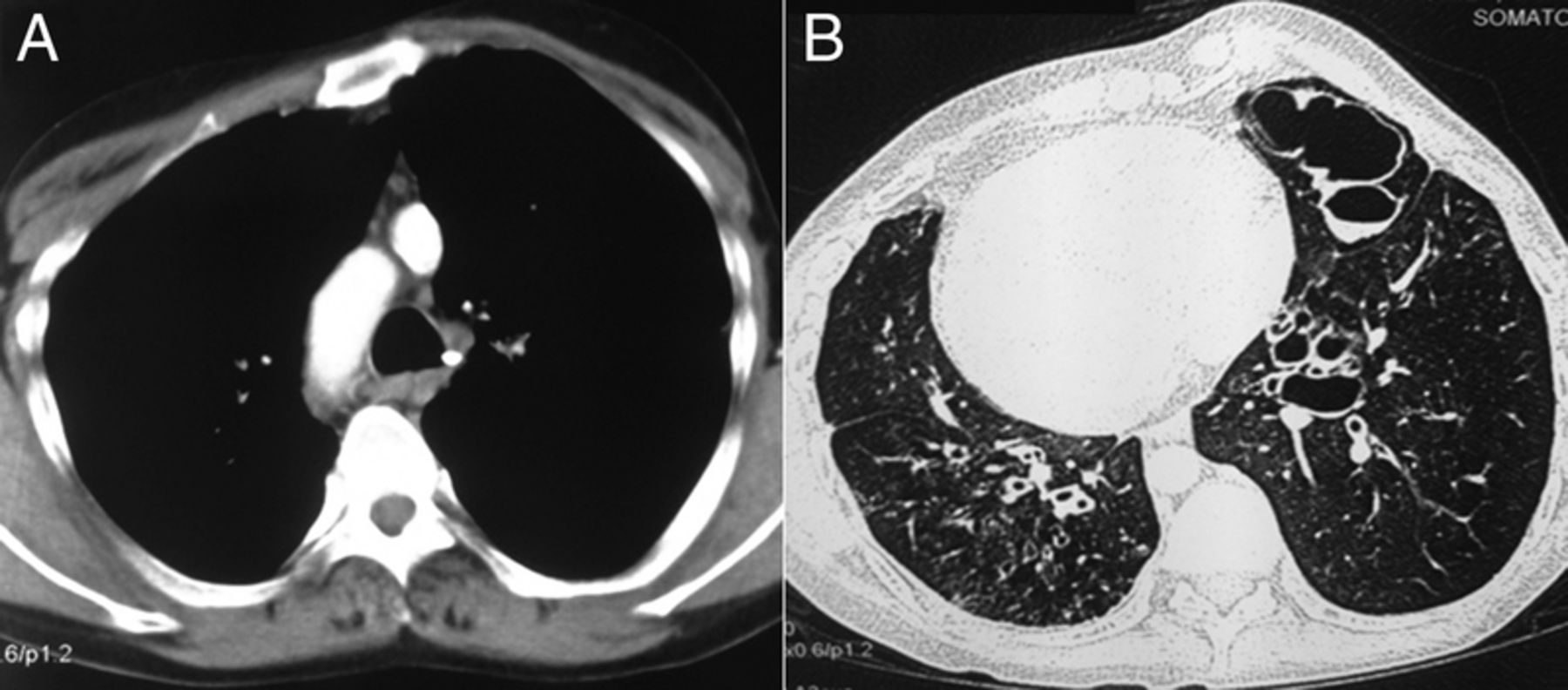
CT of the chest showing aortic arch on the right side consistent with situs inversus (A). The lung windows showing bilateral bronchiectasis and mucus impaction in a few dilated bronchi (B).

{kind=link}
{kind=link}
{kind=link}
Ultrastructural examination showing membranes of the individual cilia that have fused with one another to form large dysfunctional compound cilia (A, transmission electron microscopy (TEM), ×4000). Ultrastructural examination showing normal 9+2 microtubule structure, however, there is an absent outer dynein arm (ODA) defect (B, TEM,×40 000). (B) Inset showing a single microtubule with intact inner dynein arm (IDA) but absent ODA.
Treatment
The patient was initiated on oral prednisolone at 0.5 mg/kg body weight, which was tapered over the next 4 months and stopped. He also received a combination of inhaled fluticasone (500 μg/day) and formoterol (12 μg/day) in a pressurised metered-dose inhaler.
Outcome and follow-up
There was significant clinical and radiological improvement along with a decline in serum IgE to 948 IU/mL. A repeat spirometry showed no improvement in the forced expiratory volume in 1 s or forced vital capacity values. The patient is under close follow-up, and it is planned to initiate prednisolone and itraconazole, if there is an exacerbation of ABPA.
Discussion
This case highlights an interesting association of PCD and ABPA. The chance finding of dextrocardia prompted us to suspect Kartagener syndrome and electron microscopy confirmed the diagnosis. The diagnosis of ABPA was pursued after screening for Aspergillus sensitisation, given the high prevalence of this disorder in the community.15 The loss of normal ciliary function in Kartagener syndrome impairs clearance of airway mucus secretions, which predisposes to recurrent episodes of bacterial infections resulting in development of bronchiectasis (in roughly 80% of patients by adulthood).16 Failure to clear mucus in PCD may also cause persistence of A. fumigatus in the airways (as demonstrated by the reports of the occurrence of pulmonary aspergilloma in Kartagener syndrome, see below), which predisposes to ABPA. It is probable that because of the rarity of Kartagener syndrome, and the lack of awareness of screening for ABPA in patients with bronchiectasis, that this association might have been under-recognised. Hence, it would be prudent that patients with PCD are routinely screened for ABPA with specific IgE against A. fumigatus.17 ,18
First described in 1933, Kartagener syndrome is a variant of PCD,19 which is a heterogeneous group of disorders of motile cilia, inherited in an autosomal recessive manner. Normal cilia are hair-like projections that are present on the apical surface of the epithelial cells of the upper and lower respiratory tract (clearing of debris and respiratory mucus), female reproductive tract, spermatozoa and ependyma of brain. During embryogenesis, motile cilia have an important role in determining laterality of various organs.14 ,20 The loss of normal ciliary function leads to diseases of upper and lower respiratory tract, and defects in organ laterality.14 Respiratory symptoms are present in approximately two-third of patients and may manifest during the neonatal period (respiratory distress) or early childhood (daily nasal symptoms, productive cough).14 ,21 The diagnosis of PCD is often delayed with a median age of diagnosis ranging from 5 to 22 years due to a low index of suspicion and phenotypic heterogeneity.14 ,22 The diagnosis is made on the presence of recurrent respiratory tract infections (upper and lower), radiological evidence (dextrocardia, situs inversus, bronchiectasis, mucosal hypertrophy of paranasal sinus and others) and demonstration of ciliary defect (sperm dysmotility, identification of ultrastructural defect on electron microscopy). In our patient, chronic sinusitis, bronchiectasis and situs inversus were observed along with ultrastructural ciliary defect on electron microscopy.
ABPA is a well-described clinical entity that complicates the course of patients with asthma and CF.23 In normal individuals, the spores of A. fumigatus germinate in the airways and activate the immune response, which clears the fungi, and prevents persistence of infectious focus in the lungs. In predisposed individuals with structural lung abnormality (asthma and CF), there is colonisation of the A. fumigatus in the airway mucus. The hyphal forms of A. fumigatus release several proteins, which recruit the CD4+T-helper 2 (Th2) helper cells and further perpetuate the body's immune response in the airways. This skewed Th2 cell response causes propagation of inflammation, which in turn causes influx of neutrophils, eosinophils and IgE (total and Aspergillus specific), which are responsible for the characteristic pathology of ABPA.24
The diagnosis of ABPA is made on a constellation of elevated total and A. fumigatus-specific IgE levels, elevated eosinophil count, positive type I Aspergillus skin test, presence of precipitating (or IgG) antibodies against A. fumigatus in serum and radiographic pulmonary opacities consistent with ABPA, in patients with bronchial asthma and CF.24 However, ABPA has also been defined in patients with other structural lung disorders, including COPD, pulmonary tuberculosis, idiopathic bronchiectasis and others.7 ,8 ,10 ,12 The index case demonstrated elevated A. fumigatus-specific and total serum IgE levels, raised eosinophil values, positive skin test against A. fumigatus antigen and bronchiectasis, and thus fulfilled the diagnostic criteria for ABPA. Recently, it has also been shown that a combination of total IgE, A. fumigatus IgE and total eosinophil count levels of 2347 IU/mL, 1.91 kUA/L and 507 cells/µL, respectively, have 100% specificity in the diagnosis of ABPA.25 Our patient had values greater than the aforementioned ones, thereby confirming the presence of ABPA.
We searched the PubMed and EmBase databases using the search terms: (“Kartagener's syndrome” OR “Kartageners syndrome” OR “Kartagener syndrome” OR “primary ciliary dyskinesia” OR “primary ciliary dysfunction” OR “ciliary dysfunction”) AND (“abpa” OR “allergic bronchopulmonary aspergillosis” OR “abpm” OR “allergic bronchopulmonary mycosis” OR “aspergillosis”). Our search yielded two reports of association of Kartagener syndrome with ABPA (one meeting abstract26 and one case report27). Both the cases reported are similar to the index case (table 2). Additionally, we found two reports of pulmonary aspergilloma-complicating Kartagener syndrome.28 ,29
Previously reported association of ABPA and motile ciliary dysfunction
The diagnosis of ABPA has an important connotation in patients with Kartagener syndrome. Although bronchiectasis is an invariable consequence of Kartagener syndrome, the severity and progression of bronchiectasis can be further aggravated by the presence of ABPA. Importantly, treatment of ABPA can prevent the advancement of bronchiectasis, as ABPA is a highly treatment-responsive condition.
In conclusion, the knowledge about ABPA is growing with recognition of newer conditions that predispose to its development. Physicians involved in caring for patients with ciliopathies should be aware of the association between Kartagener syndrome and ABPA, and should maintain a high index of suspicion for ABPA in cases of PCD responding poorly to usual management. Conversely, in patients with ABPA without underlying asthma or CF, one should consider PCD, given the fact that 50% of PCD cases will lack situs inversus. Early recognition and treatment of ABPA may help in preventing the progression of lung disease in patients with PCD.
Learning points
Kartagener syndrome is an uncommon cause of bronchiectasis in adults.
Allergic bronchopulmonary aspergillosis (ABPA) can complicate the course of patients with Kartagener syndrome.
Early recognition of ABPA and adequate treatment can prevent further lung damage in Kartagener syndrome.
Patients with primary ciliary dyskinesia should be routinely screened for Aspergillus sensitisation with an Aspergillus fumigatus-specific IgE.
Patients with ABPA, especially those without asthma and cystic fibrosis, should be investigated for primary ciliary dyskinesia.
References
Footnotes
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.