Article Text

Abstract
Background: Voriconazole has an important role to play in the prophylaxis and management of fungal endophthalmitis and keratitis. New-generation triazoles, including voriconazole, posaconazole and ravuconazole, have been shown in laboratory studies and clinical experience to have very good safety profiles with few side effects. Fungal eye infections, while not common in temperate climates, have been notoriously difficult to diagnose and treat, and generally result in protracted therapy with poor final outcomes. Current treatment options are far from optimal.
Aims: This paper will review studies and clinical case reports published in the ophthalmic literature that address the safety of these drugs in the eye, penetration and concentration in ocular tissues and media, and efficacy in treating common pathogens implicated in fungal keratitis and endophthalmitis.
Conclusions: Over 40 clinical case reports of treatment with voriconazole suggest that it may be used safely and effectively against a broad range of fungal pathogens.
Statistics from Altmetric.com
Fungal eye infections have potentially devastating consequences. Fungal keratitis may be caused by ocular trauma with involvement of organic matter, or may be related to contact lens wear or refractive surgery. If not successfully treated, it can progress into the eye, causing endophthalmitis. Fungal endophthalmitis may also be the result of trauma, endogenous disease or a complication of intraocular surgery.
Fungal infections are relatively rare in the United States and other temperate climates. However, the US Centers for Disease Control (CDC) recently reported an outbreak of at least 130 confirmed cases of Fusarium keratitis among contact lens wearers in 26 states.1 The CDC’s case-control investigation found an association between the infections and use of a particular contact lens solution (ReNu with MoistureLoc, Bausch & Lomb, Rochester, NY), which was subsequently withdrawn from the US and global markets.
In South Asia, Africa and other warmer climates, fungal infections occur more frequently than in cooler climates. Relative incidence reports from India indicate that more than 20% of postcataract endophthalmitis cases2 and as much as 44% of all central corneal ulcers3 are caused by fungi.
Candida yeast species and filamentous fungi, especially Fusarium species, are the most frequent culprits in the United States, according to a recently published analysis of fungal isolates associated with keratitis or endophthalmitis cases treated at the Bascom Palmer Eye Institute over the past two decades.4 Of the 421 corneal isolates identified, Fusarium species were the most frequent fungal pathogen (49.4%), followed by Curvularia (8.1%), Aspergillus (7.1%) and Paecilomyces species (5%). Earlier accounts also point to Fusarium species as the source of many fungal keratitis infections.5 The most common corneal yeast isolates at Bascom Palmer were Candida albicans (9.5%) and C. parapsilosis (6.7%). Of the 122 intraocular pathogens isolated, almost half were yeasts, specifically Candida species; Aspergillus was found to be the most common intraocular mould.
Current treatment
Current treatment protocols for mycotic infections are far from optimal, due to a combination of the growth characteristics of fungi, late diagnosis, scarcity of effective antifungal agents and poor tissue penetration of the currently available therapeutic agents.
The most common antifungal treatments for fungal endophthalmitis are intravenous and/or intravitreal amphotericin B. At times, treatment is combined with a vitrectomy due to limited intraocular drug penetration. Amphotericin B may also be injected directly into the vitreous to achieve higher concentrations; however, toxicity to the retina has been reported, especially if accidentally injected into an air-filled eye. Limitations of intravenous amphotericin B include required hospitalisation, severe ocular inflammation and numerous systemic adverse effects such as nephrotoxicity, fever, rigors and hypotension. Moreover, the effectiveness of amphotericin B against the most commonly implicated fungal isolates is limited. For example, O’Day and colleagues demonstrated that intravitreal concentrations of amphotericin B barely reach the minimum inhibitory concentration at which 90% of isolates are inhibited (MIC90) for Candida parapsilosis6 after systemic administration.
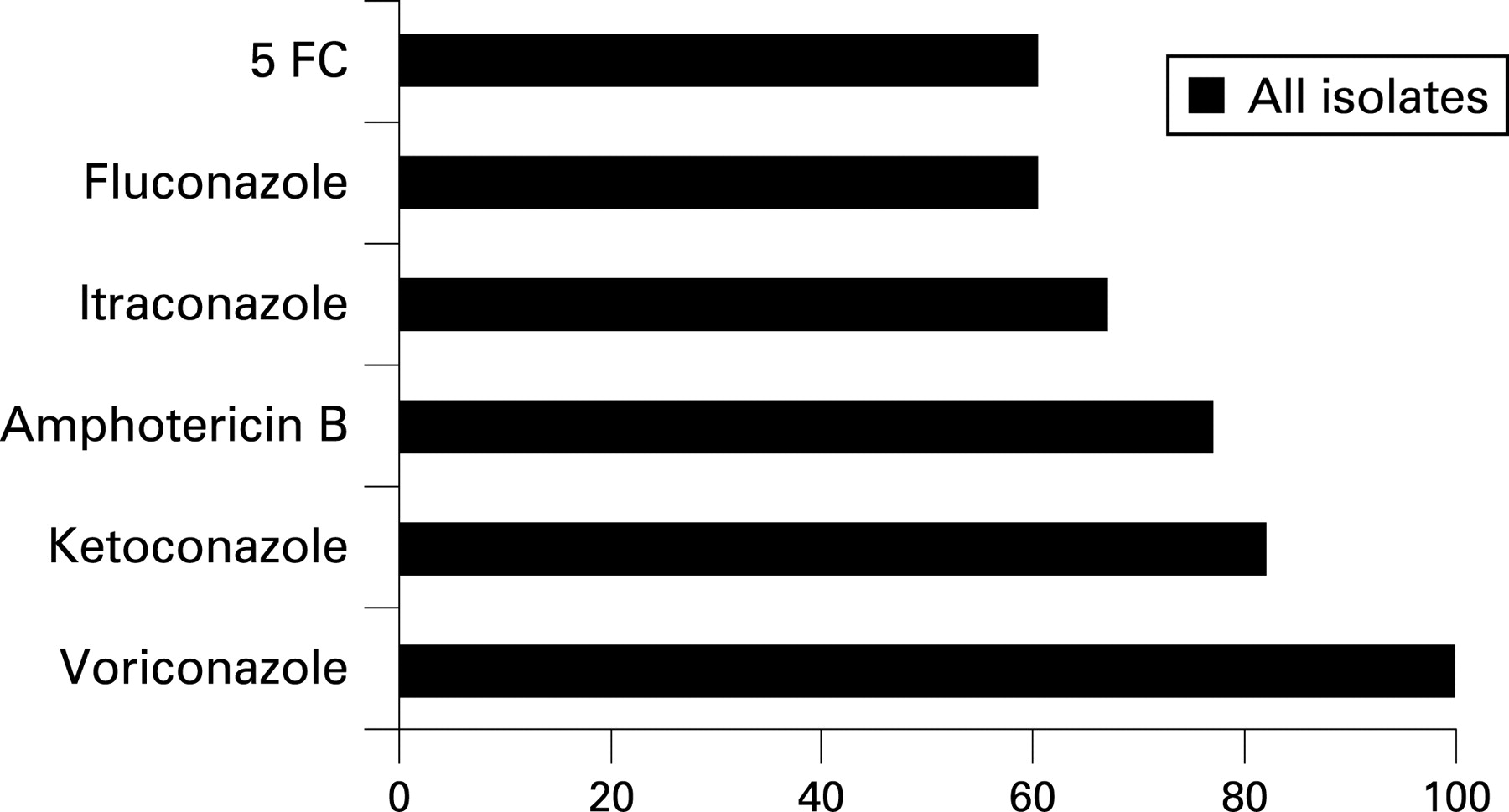
Fluconazole, an older-generation triazole, has been used systemically as a supplement or alternative to amphotericin B, but it lacks the broad spectrum of coverage necessary for the most commonly encountered fungal species in eye disease. Furthermore, intraocular penetration is marginal. Itraconazole is rarely used in the treatment of ocular fungal eye infections, as it lacks a broad spectrum of coverage, specifically against Fusarium species4 (fig 1).

Topical natamycin, a polyene, is the only Food and Drug Administration (FDA)-approved and commercially available topical antifungal. It has good efficacy against filamentous fungi but does not penetrate well into the cornea. Additionally, it forms precipitates upon instillation and degrades easily, requiring storage in a dark container. Topical amphotericin B is commonly used in the management of fungal keratitis, but it requires preparation by a compounding pharmacy.
New-generation triazoles
There are promising reports in the literature suggesting that newer-generation triazole agents may overcome the significant shortcomings of existing therapies. Triazoles inhibit the biosynthesis of ergosterol, an essential component of the fungal cell wall. The newest triazole agents, including ravuconazole, posaconazole and voriconazole, are synthetic derivatives of fluconazole but have a significantly broader spectrum of activity. At present, only voriconazole (Vfend, Pfizer, New York) is commercially available. It has been approved by the FDA for the treatment of invasive aspergillosis, espophageal candidiasis and other systemic indications, and is available in oral and intravenous formulations.
Ravuconazole (Bristol-Myers Squibb, Wallingford, CT) has been shown to have in vitro activity against non-ocular isolates of yeasts, Aspergillus species and other filamentous fungi, black moulds, and some Mucorales.7 8 Some Fusarium species were resistant.
Posaconazole (Noxafil) oral suspension (Schering-Plough, Kenilworth, NJ) was recently FDA approved in the fall of 2006. In vitro and in vivo studies have shown it to have broad-spectrum activity against non-ocular isolates of most Candida species, Cryptococcus neoformans, Aspergillus species, Fusarium species, zygomycetes and endemic fungi.9 One study showed it to be active against a majority of isolates resistant to fluconazole and itraconazole, and the most active of any antifungal agent tested against Aspergillus.10 Adverse events, most commonly gastrointestinal complaints, are generally mild.11
Voriconazole has been shown to have a broad spectrum of activity against non-ocular isolates of Aspergillus species, Candida species, Paecilomyces lilacinus, Cryptococcus neoformans, Scedosporium species, Curvularia species and others.12–15 It has excellent in vitro activity with low MIC values against Candida and Aspergillus species known to be resistant to amphotericin B, fluconazole and itraconazole.16 17 Activity against Fusarium species has been variable.
It has been reported to be fungicidal against most Aspergillus species and some dematiaceous fungi.11 18 Voriconazole has also become the new standard of care in the treatment of invasive aspergillosis which may occur in immunocompromised patients, including allogeneic BMT, other haematological cancers and solid organ transplants. This is based on the results of a large, randomised study in which it proved superior to amphotericin B with 53% complete or partial response, compared with 32% for amphotericin B.19 In another large, randomised study comparing voriconazole to amphotericin B for empiric therapy in patients with neutropenia and persistent fever, the success rate for treatment with voriconazole was slightly lower than amphotericin B at 26.0% to 30.6%, respectively, but there were much fewer side effects in the voriconazole group compared with the amphotericin group.20
Adverse effects, including visual disturbances and skin rashes, have been mild and transient. Visual disturbances, including abnormal vision, colour vision change and/or photophobia, typically resolve within 1 month, even with continued therapy. Elevations in hepatic enzyme levels can occur.
This paper is intended primarily to review studies and clinical case reports published in the ophthalmic literature that address the safety of these drugs in the eye, penetration and concentration in ocular tissues and media, and efficacy in treating common pathogens implicated in fungal keratitis and endophthalmitis.
OCULAR SAFETY
Gao and colleagues were the first to show the safety of voriconazole in the eye.21 They examined retinal toxicity in a rodent animal model and found that intravitreal voriconazole in high concentrations of up to 25 μg/ml caused no electroretinographic or histological abnormality in the rat retina.
In human clinical use, none of the case reports we reviewed (multiple reports of voriconazole treatment;8 22–34 36 38 39 41–50 two reports of posaconazole treatment) identified any adverse effects other than mild, transient visual disturbances and elevation of liver enzymes. The safety profile of these triazole agents represents a remarkable improvement when contrasted with the extremely negative side effects of amphotericin B.
OCULAR PENETRATION AND CONCENTRATION
In 2004, Hariprasad and colleagues demonstrated that orally administered voriconazole showed good tolerability and bioavailability, achieving therapeutic concentrations in the non-inflamed eye.35 Fourteen patients scheduled for elective pars plana vitrectomy were given two 400 mg doses of voriconazole 12 h apart prior to surgery. Aqueous, vitreous and plasma samples were obtained during surgery, within 3 h of the second dose of voriconazole.
After two doses, the mean plasma concentration of voriconazole was 2.13 μg/ml, which resulted in voriconazole concentrations of 0.81 μg/ml (38.1% of plasma levels) in the vitreous and 1.13 μg/ml (53.0% of plasma levels) in the aqueous. The concentrations achieved in the vitreous in this study far exceed the MIC90 for a wide spectrum of yeasts and moulds, although not for Fusarium species (table 1).
Separately, they also reported aqueous and vitreous levels from a patient with active fungal inflammation who died 1 week after initiating treatment with intravenous voriconazole 200 mg twice daily.36 Postmortem analysis showed concentrations of the drug in the vitreous of 1.12 μg/ml and in the aqueous of 1.52 μg/ml, again far exceeding MIC90 levels for a wide spectrum of pathogens. Due to the breakdown in the blood–aqueous barrier, it is not surprising that a systemically administered drug would achieve higher concentrations in an infected eye than it did in non-inflamed eyes.
Hariprasad and colleagues also analysed topically administered voriconazole in non-inflamed human eyes.37 In this study, a voriconazole 1% topical solution was used every 2 h for 1 day prior to planned vitrectomy surgery. The mean concentration of voriconazole was 6 μg/ml in the aqueous and 0.15 μg/ml in the vitreous, demonstrating that the drug penetrates well beyond the cornea when applied topically. Given that aqueous and vitreous levels exceed or meet the MIC90 for most pathogens, one could assume that concentrations on the ocular surface would be more than sufficient to treat fungal keratitis.
In a case report of an eye with Scedosporium apiospermum keratitis that went on to corneal transplant, Nulens and colleagues found that aqueous voriconazole levels following 12 days of oral treatment were about 50% of plasma levels.38 In a later case report, this team also found that applying voriconazole topically (1% voriconazole solution at hourly intervals) resulted in significantly increased drug levels in the anterior chamber.39 The voriconazole level in the aqueous humour was 3.2 μg/ml, which was 160% of the level in plasma (2.0 μg/ml).
In a rabbit model, Sponsel and colleagues also demonstrated that topical voriconazole penetrates beyond the corneal tissue.40 Rabbit eyes infected with Paecilomyces lilacinus were treated twice daily with a topical voriconazole solution. When corneal, vitreous and chorioretinal tissues were analysed, tissue concentrations at both doses tested (5 and 10 μg/ml) exceeded the MIC90 for P. lilacinus. Tissue concentrations were highest in the cornea; the chorioretinal concentration was roughly twice as high as the vitreous concentration.
In the one case report involving posaconazole, the drug was given orally four times daily (200 mg each) and topically, with an hourly application of the same 10 mg/0.1 ml oral suspension. A diagnostic vitrectomy indicated that the concentration of posaconazole in the vitreous was 0.25 μg/ml, compared with 1.2 μg/ml in the plasma.41
OCULAR EFFICACY: LABORATORY MODELS
In 2004, Marangon and colleagues published an investigation of antifungal susceptibility, in which voriconazole was the only agent of six tested with 100% activity against a wide variety of Aspergillus, Fusarium and Candida isolates4 (figs 1, 2).

{kind=link}
{kind=link}
They evaluated the in vitro susceptibility of 36 keratitis or endophthalmitis isolates (21 Candida species, 10 Fusarium species, four Aspergillus species and one Paecilomyces species) to various antifungals.
All yeast isolates were sensitive in vitro to most antifungal agents including voriconazole. All moulds were resistant to fluconazole. In vitro susceptibility profiles are shown in fig 2. Voriconazole had a very low MIC90 for the Candida and Aspergillus isolates in this study.
In the experimental rabbit study mentioned earlier,40 topical voriconazole halted or reversed the progression of corneal infection by P. lilacinus beyond a single-axis 2 mm diameter in nine of 10 infected eyes, including three eyes with complete resolution of the fungal keratitis.
For this study, voriconazole powder was suspended to concentrations of 5 and 10 μg/ml. Although much higher doses of the drug have been tested intravitreally, the authors concluded that less concentrated topical applications may be adequate to prevent or treat extension of corneal infection to the deeper eye tissues.
OCULAR EFFICACY: CLINICAL CASE REPORTS
New-generation triazoles have been used in the treatment of fungal infections, generally with considerable success. Many of the patients described in the literature failed treatment with conventional antifungal agents, and success was achieved only after initiating a new-generation triazole. Case reports are summarised in table 2.
We identified four case reports involving the use of posaconazole.41 42 A 42-year-old with invasive Fusarium solani keratitis and endophthalmitis was successfully treated with posaconazole after high doses of amphotericin B (both topical and intravenous), natamycin and ketoconazole failed to stop the infection from spreading. At 16 months, the prognosis for eventual lens replacement and visual rehabilitation of the eye appeared very good.
Tu et al recently reported three cases of Fusarium ocular infections.42 The first case developed Fusarium keratitis and endophthalmitis and was treated with a combination of topical, intracameral, intravitreal and systemic amphotericin B and voriconazole. Because of the unresponsive nature to the infection, the patient was switched to posaconazle with resolution of the infection. The two other cases reported developed Fusarium keratitis and one developing endophthalmitis. Both were initially treated with topical and systemic voriconazole before developing systemic complications from treatment (elevated liver enzymes) and were switched to posaconazole with a rapid resolution of the infectious process.
There have been at least 36 cases reported involving treatment with voriconazole. The first such case report was published by Reis and colleagues in 2000. They treated a 16-year-old whose keratitis had been deteriorating for months and was later shown to be Fusarium species.43 The recurrent infection was treated with topical amphotericin B and systemic fluconazole and itraconazole, to no avail. Intravenous voriconazole produced a significant improvement, and the infection was finally resolved after adding topical voriconazole.
Many of the subsequently published cases were also essentially rescue attempts, in which voriconazole therapy was attempted as a last resort after a long clinical course with prior failure of other agents. Scott and colleagues treated a patient with bleb-associated fungal endophthalmitis.44 Prior to culture results, the patient was treated with antibiotics and corticosteroids. Once the fungal nature of the infection was clear, the patient received three intravitreal injections of amphotericin B, lensectomy with two vitrectomies, oral and topical ketoconazole, oral fluconazole, and intraocular (one injection of 50 μg) and oral (200 mg twice daily) voriconazole. The patient was finally treated successfully with high-dose intravitreal voriconazole. A single injection of 200 μg/0.1 ml (four times the recommended intravitreal dose) was given.
The degree to which resolution of the infection was achieved and the speed of recovery after months of failed treatment in some cases are remarkable.45 46 Two small series have been reported with notably good visual outcomes.
Durand and colleagues reported on the successful use of voriconazole in two cases of postcataract surgery fungal endophthalmitis.47 The first case was a man with postcataract extraction Fusarium endophthalmitis. The infection persisted despite removal of the intraocular lens, three vitrectomies and five intravitreal injections of amphotericin B. Treatment with oral voriconazole (300 mg, twice daily) for 6 months resolved the inflammation and improved vision in the eye from 20/80 to 20/40.
The second case was a man with postcataract surgery intraocular inflammation later diagnosed to be Aspergillus fumigatus endophthalmitis. Intravitreal amphotericin B and systemic voriconazole (6 mg/kg intravenously q12h ×2 doses, then 200 mg orally twice daily) were given, but there were signs of recurrence after 1 week. Intravenous caspofungin was added, and the eye improved. Vision improved from counting fingers to 20/80 at 6 months and 20/25 at 23 months. Previous research had shown that caspofungin may act synergistically with voriconazole against Aspergillus in systemic infections,48 and Durand’s case is the first to support this combination approach in an ocular setting.
Researchers at the Barnes Retina Institute and the Cullen Eye Institute reported on a series of seven eyes of five patients with confirmed Candida endophthalmitis infections.36 A variety of routes of administration and dosing regimens were employed in the series, including intravenous and oral voriconazole, with or without caspofungin, and intravitreal injection of voriconazole.
Five of the eyes in this series had excellent final visual acuities of 20/30 or better. Interestingly, three patients in the series developed fungal endophthalmitis or experienced progressive worsening of the disease while being treated with fluconazole. This is evidence that fluconazole was ineffective against the pathogens involved or did not achieve therapeutic concentrations in the vitreous.
As noted above, there is some debate about whether voriconazole achieves the MIC90 to be effective against Fusarium species, the most common aetiology in fungal keratitis. Two Fusarium cases (one oral, one topical), described below, have been reported in which voriconazole therapy was not effective.
Verma and colleagues treated postlaser in situ keratomileusis keratitis in a 45-year-old woman with oral voriconazole (400 mg daily) without success.49 Despite intensive treatment with a variety of agents, including voriconazole, the patient went on to require three penetrating corneal grafts, with a poor visual result in the end. Fusarium solani was subsequently grown from the initial corneal button.
Marangon and colleagues noted that, even though voriconazole did very well in their in vitro susceptibility analysis, it was not effective in clinical use in two of their patients with keratitis, one Fusarium species and the other Colletotrichum.4 In both of these cases, topical treatment with a 1% solution failed to control the infection.
On the other hand, in the Durand and Reis cases and at least two others,48 50–52 voriconazole was effective in treating Fusarium infections. In some cases, oral voriconazole may not produce sufficient concentrations of drug in corneal tissues. The Klont and Reis cases suggest a beneficial effect of adding topical voriconazole to systemic treatment in Fusarium keratitis.
There have now been at least 12 reported cases in the use of intravitreal voriconazole in the treatment of fungal endophthalmitis. Organisms treated with this route of administration include Candida,36 Aspergillus,29 Scedosporium,23 28 31 34 Fusarium31 and Verticillium.30 Dosages used ranged from 100 μg/0.1 ml to 200 μg/0.1 ml. In those eyes with endogenous Scedosporium, outcomes were typically poor, with two of seven eyes leading to enucleation. Three patients eventually died from systemic sepsis. Given the immunosuppressed nature of these patients, and the 90% mortality of disseminated Scedosporium, the abysmal outcomes in these patients are not surprising. In those eyes with postoperative fungal endophthalmitis, a combination of oral, intravenous and intravitreal voriconazole successfully controlled the infection. In those eyes that were successfully treated, there were no signs of retinal toxicity.
DISCUSSION AND CONCLUSIONS
The activity spectrum of new generation triazoles encompasses many yeast and mould species, including the mycotic species most frequently implicated in fungal keratitis and endophthalmitis. In addition to excellent susceptibility profiles, these drugs also appear to be quite safe and well tolerated by patients (in contrast to the very poor side effect profile of amphotericin B). Finally, several studies and case reports have now shown therapeutic intraocular concentrations through various routes of administration in the human eye. Together, this evidence suggests that voriconazole and other new triazole agents are powerful tools in the management of fungal keratitis and endophthalmitis. This is a most welcome advance, given the abysmal success rate in treating fungal eye infections up to this point.
In keratitis or endophthalmitis cases where the aetiology may be unclear for weeks or months, the potential to be able to treat the eye with a relatively safe, broad-spectrum antifungal in addition to a broad-spectrum antibiotic agent in an outpatient setting may allow for improved visual outcomes. Current antifungal agents are too toxic to be used prophylactically in this fashion. Additionally, prophylactic treatment with oral voriconazole in cases of ocular injury with vegetable matter may be useful in preventing the development of fungal keratitis or endophthalmitis in this high-risk population.
The availability of multiple routes of voriconazole administration, including topical and intravitreal solutions that can be prepared by a compounding pharmacy, provides the clinician with flexibility and creativity in managing these difficult eye infections. Effective oral or topical medications that can be self-administered are important, as ophthalmology is primarily practised in the outpatient setting. Additionally, the cost savings by avoiding hospitalisation for administration of older-generation intravenous antifungals are important.
Voriconazole is rapidly metabolised, so one should consider following a single intravitreal injection with oral or topical administration in order to maintain therapeutic intraocular concentrations and increase efficacy.
The new-generation triazoles provide ophthalmologists with much-needed new weapons in the arsenal of treatments against fungal eye disease. We believe there is sufficient evidence in the literature to support treatment with voriconazole prophylactically in patients at high risk for developing fungal keratitis or endophthalmitis. When a fungal aetiology is known or strongly suspected, oral voriconazole may be considered as first-line therapy or used as an adjunct to other antifungal treatment. Intravitreal injections of voriconazole have been reported in case reports with some success and no reports of toxicity, but more data should be obtained before any conclusions can be drawn from this route of administration. Obviously, given the variability of fungal eye infections, the clinician should use judgement regarding the route of voriconazole administration.
Acknowledgments
The authors wish to thank Pfizer pharmaceuticals for providing funding to support the research and editorial services of Jan Beiting and Hospicom. The authors would also like to acknowledge the Research to Prevent Blindness Organization, New York.
REFERENCES
Footnotes
Funding: Funding was received from Pfizer for technical research assistance in preparing this manuscript. SMH’s research was supported by an unrestricted grant from the Research to Prevent Blindness Organization, New York, NY.
Competing interests: SMH, WFM and TKL have no competing interests. WES has received grants from Pfizer and other competing organisations such as Fujisawa. JRG has received grants from Merck, Pfizer and Schering. He is also on the Merck and Schering advisory board.