Article Text

Abstract
Objective To compare the effects of metoclopramide and domperidone on the breast milk output of mothers with infants in neonatal intensive care.
Design Double-blind randomised controlled trial.
Setting Tertiary level neonatal intensive care unit (NICU).
Sample Eighty mothers expressing breast milk for their infants (mean gestational age 28 weeks) based in NICU and the amounts expressed fell short of the prescribed target.
Intervention Mothers were randomised to receive domperidone or metoclopramide for 10 days (10 mg three times a day).
Outcome measures Total milk volume daily for up to 10 days before the medication, 10 days during the trial and up to 10 days after medication. Adverse side effects were also recorded.
Results Mothers produced more milk in the domperidone group and achieved a mean of 96.3% increase in milk volume (mean increase/pretrial volume) compared with a 93.7% increase for metoclopramide. After adjusting for the amount of milk produced prior to medication, the mean amount of milk produced while taking medication for those on domperidone was 31.0 ml/24 h (95% CI −5.67 to 67.6) greater than the mean for those on metoclopramide. Seven mothers taking metoclopramide reported side effects and three taking domperidone; a further eight women (of 29) who had a follow-on prescription for metoclopramide also reported side effects.
Conclusions Oral domperidone and metoclopramide increased the volume of milk produced by mothers who are expressing to feed their babies in NICU. There were small differences in milk output between the two medications and in the incidence of side effects, but the differences were non-significant.
Statistics from Altmetric.com
Introduction
Breast milk is the optimum food for preterm and term infants, reduces the risk of infection (including necrotising enterocolitis) and improves neurodevelopmental outcomes.1,–,4 Consequently, the mothers of infants in neonatal care are encouraged to provide expressed breast milk although they may often find it difficult to produce adequate quantities to meet their infant's needs over the longer term before their baby can feed at the breast. This can be further exacerbated by the range of experiences and emotions that mothers experience in the neonatal intensive care unit (NICU), including exhaustion, anxiety and unresolved grief.5 ,6
What is already known
Metoclopramide and domperidone (10 mg orally three times a day) both increase breast milk production by their effect on prolactin secretion.
What this study adds
▶ This is the first trial to compare the enhancing effects of domperidone with metoclopramide on breast milk output and to record any maternal side effects systematically.
▶ There were small differences in the milk output between the two medications and in the incidence of side effects, but the differences were non-significant.
Frequent and efficient milk removal is essential for continued production of breast milk. Non-pharmacological interventions such as holding their baby in close skin-to-skin contact, expressing milk as soon after delivery as possible, frequent pumping up to 12 times in 24 h, lactation counselling and relaxation techniques may all be beneficial.7,–,9 However, some mothers are recommended pharmacological methods to increase their milk supply when their lactation starts to fail. Most galactogogues exert their pharmacological effects through interactions with dopamine receptors, resulting in increased prolactin levels, and thereby augmenting milk supply.10 Metoclopramide is most commonly used, due to its documented efficacy and safety in women and infants.11,–,13 It crosses the blood–brain barrier and very rare side effects in mothers may include tremor, bradykinesia (slow movements) and other dystonic reactions. Domperidone does not readily cross the blood–brain barrier and is less likely to cross into breast milk than metoclopramide, thus decreasing any risks of toxicity to mother and infant; and rare transient side effects include abdominal cramps and headache.14,–,16 Currently, in the UK both medications are given for at least 10 days to enhance milk production, but their use as galactogogues is not licensed (http://www.nelm.nhs.uk/en/NeLM-Area/Evidence/Medicines-Q--A/Drug-treatment-of-inadequate-lactation).
Small amounts of both medications have been detected in breast milk samples, with no adverse effects to babies reported. Studies have examined the effects of the medications compared with placebo,11 ,15 on the composition of breast milk,17 on serum prolactin levels13 ,15 ,18 ,19 and the transfer of medication into the newborn.16 ,20 A comparative study between the two drugs focused on prolactin responses in non-pregnant women rather than milk production in breastfeeding mothers.21 This is the first trial to compare the milk enhancing effects of domperidone with metoclopramide and to record any maternal side effects systematically.
Methods
A prospective randomised blinded controlled trial study was carried out. Mothers of infants in one tertiary NICU, who were expressing their breast milk, were invited to document milk production at each expression in a systematic fashion, using a standard data collection sheet. The 24 h totals gave the baseline values for milk production and enabled the staff to provide advice on the efficient milk expression techniques.
Mothers not producing 160 ml/kg/day for their baby after several days of expressing were encouraged to express more frequently (at least eight times in 24 h) and increase skin-to-skin (kangaroo) contact with their baby. Those still not reaching the target volume were invited to enter the trial and given the information sheet; 160 ml/kg/day is the average milk volume prescribed for preterm babies once they reach full feeds in order to optimise nutrition. The final volume of milk recommended varies with gestational age and postnatal age. Mothers who consented were randomised to take either metoclopramide or domperidone for 10 days (both drugs prescribed at 10 mg three times a day), after consultation with an obstetrician. A letter was faxed to the mother's general practitioner (GP), if they were no longer an in-patient, to inform them about the trial.
Permission was obtained to use the milk expression data collected prospectively for 10 days before the medication started, for 10 days when they were taking the medication and for 10 days after the medication had finished. Mothers were also asked to record any side effects that they experienced as free text on the data sheet.
Randomisation and packing of the drugs was carried out by the University Hospitals Bristol pharmacy; sequentially numbered identical bottles containing identical capsules were produced. Each bottle was labelled with the name of the trial (identifying both medication names) and a number. The medication was encased in a gelatine capsule to ensure that mothers and staff were blind to which drug they were taking. Randomisation was blocked, allocation based on random number tables, and the randomisation code was kept by the pharmacy and by the principal investigator. The bottles were dispensed and recorded by the lactation specialist.
All mothers under 16 years of age were excluded from the study and also any mother who had had an adverse reaction to either drug in the past or who was taking other medication that might be contraindicated.
Original sample size calculations showed that to detect 0.5 SD difference (medium-sized effect) in the increase in the volume of milk produced (from days 1 to 10) between the two groups with 80% power (0.05 level of significance), 64 women with complete data would be needed in each group.
The primary outcome measure was breast milk volume per 24 h when the medication was being taken. Secondary outcomes were the volume of milk produced after the course of medication had finished and the frequency of adverse maternal side effects in each medication group.
The demographic characteristics were tabulated by the treatment group, and as the premedication milk volume differed between the two groups, regression analysis was used to compare the milk volumes for the medication phase.
A graph of milk output was created using the last observation carried forward to ensure that all subjects had data for the 10 medication days and the last 4 days before randomisation, as not all had data for 10 days before medication. Consequently, using a mean value for premedication milk output produced a biased predictor of milk output when on medication. To avoid this bias, a multilevel model was used in which all milk volumes recorded were used for each woman, and a factor fitted for individual women and the number of days before randomisation. Multiple observations for each woman were controlled for in estimating the standard errors using the robust method in STATA v 9.
Research ethics approval was obtained from the Central and South Bristol Research Ethics Committee and research governance approval from the North Bristol NHS Trust Research and Development Department.
Results
The flow of participants through the trial is shown in figure 1. Mothers were recruited to the trial from April 2007 to March 2010. Eighty mothers agreed to take part and were randomised to take one of the medications, 15 were excluded as they stopped expressing or taking the drugs soon after being randomised and 65 mothers completed the trial. Fifty mothers continued to collect data for several days after completing the medication phase and provided follow-up data for milk output without medication. Demographic information for all 80 mothers in the trial is shown in table 1. Two mothers had term babies (40 weeks gestation; one in each medication group) and the remaining babies had a mean gestational age of 28 weeks (range 23–35 weeks). The 15 excluded women came equally from both groups (7 of 38, 18.4% domperidone; 8 of 42, 19% metoclopramide).

Flow diagram of mothers in the breast milk trial.
Demographics of all 80 mothers recruited to the breast milk trial
Milk output
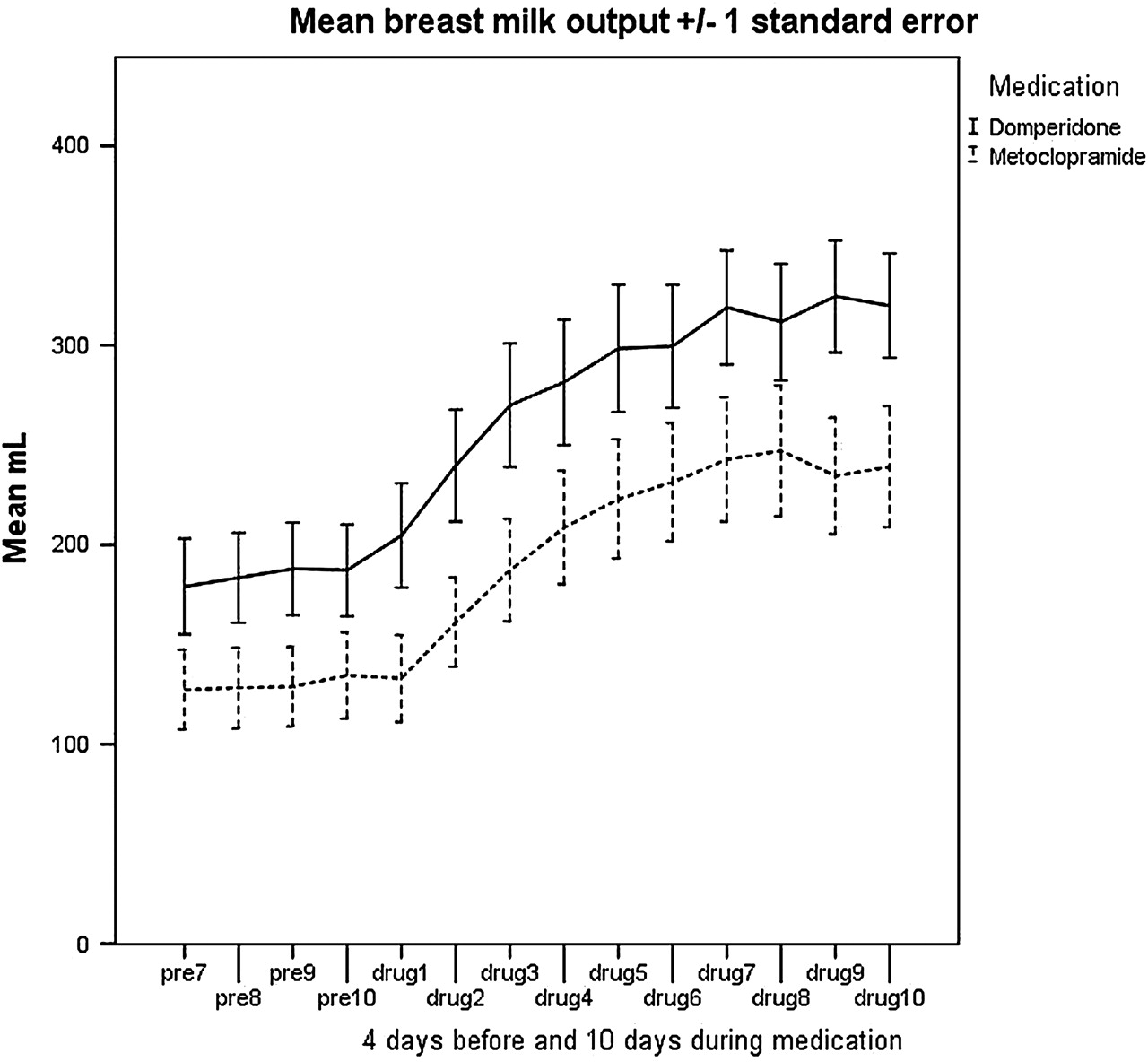
Milk output from 4 days before medication and during the medication phase is shown in figure 2. Table 2 shows the milk output per day for the 65 mothers with complete data for the medication phase of the trial. Initial comparisons indicated that those in the domperidone group produced more milk (42.9 ml/day) than those in the metoclopramide group. The domperidone group achieved a mean of 96.3% increase in milk volume (mean increase/premedication volume) compared with a 93.7% increase in the metoclopramide group.

{kind=link}
{kind=link}
Average milk output (ml per 24 h) over the medication phase of the study for mothers taking domperidone or metoclopramide (drug days 1–10) and for 4 days before (pre-7 to pre-10).
Mean unadjusted milk volumes (ml per 24 h) for 65 mothers in the medication phase of the trial and mean differences with 95% CIs
Regression analysis was carried out for all 65 mothers and table 3 shows the results for the differences in milk volume between the groups during the medication phase. After adjusting for the amount of milk produced individually prior to being on the medication and time on medication, the estimated difference in the amount of milk produced while taking medication for those on domperidone was 31.0 ml per 24 h (95% CI: −5.7 to 67.6) greater than the mean for those on metoclopramide (not statistically significant). The results were very similar for the 50 mothers with data for all three time periods. Milk volumes were consistently greater in the domperidone group compared with the metoclopramide group. Milk production after the end of the medication was adjusted for premedication milk output and for milk volumes when taking the medication, which reduced the difference to 15.3 ml (95% CI −40.1 to 70.6).
Regression results comparing the differences in the milk output between domperidone and metoclopramide before and after adjusting for baseline milk outputs
Side effects
Ten women (15.4%) reported 12 side effects when taking the medication as shown in table 4. Over 20% (7) of the mothers taking metoclopramide reported side effects and 9.7% (3) of those taking domperidone. Only one woman stopped taking the trial medication (metoclopramide) after 5 days due to bad headaches and dry mouth; all the others tolerated any side effects as they were keen to keep their increased milk production going.
Types of side effects experienced by 10 women taking the galactogogues during the trial (two women experienced two side effects each) and eight women when taking post-trial (open-label) metoclopramide (no side effects reported for open-label domperidone)
Thirty-one mothers obtained a prescription for metoclopramide (29) or domperidone (2) from their GP after the trial medication and post-trial medication data collection period had finished. Milk output data from this subsequent phase (when some were on open-label prescription drugs) were not analysed, but the side effects recorded were included. Of the 29 women who had a follow-on prescription for metoclopramide, eight (27.6%) reported side effects, 6 (75%) of whom had taken domperidone as their trial medication. These side effects included those reported during the trial (diarrhoea, mood swings) but also depression (2), itchy skin, tiredness, restless legs and less effective milk stimulation. One woman also reported switching to domperidone (prescribed by her GP) when she could not cope with the tiredness while she was taking metoclopramide. Those taking domperidone as their second course of medication reported that their milk supply was even better than the first course. None of the differences were statistically significant due to the small numbers involved.
Discussion
This trial has shown that oral domperidone and metoclopramide increased the volume of milk produced by mothers who are expressing to feed their babies in NICU. There were small differences in the milk output between the two drugs and in the incidence of side effects, but the differences were non-significant. While the 31-ml difference in the daily milk expression did not reach statistical significance, for a 1-kg baby this volume is quite clinically significant and could make a difference for the baby in terms of being exclusively fed on breast milk, or being fed a mix of formula and breast milk. None of the side effects reported caused the trial to be stopped and only one mother stopped taking the medication due to side effects.
Taking part in the trial and documenting the milk volume expressed enabled the NICU lactation consultants to monitor and encourage the women's progress and also helped mothers understand why they needed to express more frequently.
Limitations of the study were the slow recruitment rates that meant that only 80 women were recruited to the trial during the funded time period of the trial rather than the 128 planned. We involved two other hospitals, but they were unable to recruit any women to the trial, due to the reluctance of women to take medication to enhance their milk supply in one unit and the second unit having a population of babies from across a region whose mothers did not stay in the central unit for long enough to be involved in the trial. A strength of this study compared with others15 ,17 is that we adjusted for baseline milk supply, which showed the true differences in the increase in milk output between the groups. We have not found any other comparable trials to combine with our results for meta-analysis, which would help to strengthen the conclusions.
Until recently, metoclopramide has been the galactogogue of choice in the UK for mothers who need to increase their breast milk supply for their infants in neonatal care, due to its safety in women and infants.11,–,13 However, domperidone, which does not cross the blood–brain barrier as readily as metoclopramide, may be a safer alternative. Domperidone has been shown to be effective in increasing breast milk volumes in small trials, with only low levels of the medication being detected in breast milk, thus minimising any risk to breastfed infants.15 ,16 Future research could explore these effects in larger trials to add to the evidence to inform those prescribing galactogogues for women.
Acknowledgments
The authors thank Rachel Hillan, Marion Copeland and Kate Battersby for assisting with recruiting mothers to the trial, and are grateful to all the mothers who took part and documented their milk output so carefully.
References
Footnotes
-
Funding Funding was provided by the Special Trustees of University Hospitals Bristol NHS Foundation Trust.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.