Article Text

Abstract
Objective: The purpose of the study was to evaluate the efficacy and safety of botulinum A toxin in the treatment of detrusor sphincter dyssynergia in multiple sclerosis patients.
Methods: This was a multicentre, placebo controlled, randomised, double blind study. Patients with chronic urinary retention were included if they had post-voiding residual urine volume between 100 and 500 ml. They received a single transperineal injection of either botulinum A toxin (100 U Allergan) or placebo in the sphincter and also 5 mg slow release alfuzosin bid over 4 months. Main endpoint was post-voiding residual urine volume assessed 1 month after injection. Follow up duration was 4 months. Statistical analysis was performed using a sequential method, the triangular test.
Results: The study was stopped after the fourth analysis (86 patients had been included: placebo: 41, botulinum A toxin: 45). At inclusion, there was no significant difference between groups whichever variable was considered. Mean (standard deviation) post-voiding residual urine volume was 217 (96) and 220 (99) ml in placebo and botulinum A toxin groups, respectively. One month later, post-voiding residual urine volume was 206 (145) and 186 (158) ml (p = 0.45) in placebo and botulinum A toxin groups, respectively. However, compared to placebo, botulinum A toxin significantly increased voiding volume (+54%, p = 0.02) and reduced pre-micturition (−29%, p = 0.02) and maximal (−21%, p = 0.02) detrusor pressures. Other secondary urodynamic endpoints and tolerance were similar in the two groups.
Conclusions: In multiple sclerosis patients with detrusor sphincter dyssynergia, a single injection of botulinum A toxin (100 U Allergan) does not decrease post-voiding residual urine volume.
- EDSS, Expanded Disability Status Scale
- IPSS, International Prostatism Symptom Score
- SD, standard deviation
- botulinum toxin
- detrusor sphincter dyssynergia
- multiple sclerosis
- urodynamics
Statistics from Altmetric.com
- EDSS, Expanded Disability Status Scale
- IPSS, International Prostatism Symptom Score
- SD, standard deviation
Detrusor sphincter dyssynergia1 is frequently encountered in multiple sclerosis2,3 and is the main urodynamic dysfunction in this disease.3–5 Different therapeutic strategies, including the use of drugs (spasmolytic agents, alpha blockers) and surgery (endourethral prosthesis, sphincterotomy), have been proposed,5 but they usually do not restore normal synergia and may cause several side effects such as sexual impotence. Botulinum A toxin, which has been used for several years in the treatment of movement disorders, blepharospasm, hemi facial spasm, spasmodic dysphonia, and spasticity, could provide an alternative approach.6 In clinical trials performed in patients with detrusor sphincter dyssynergia, botulinum A toxin generally decreased detrusor and urethral pressures and reduced post-voiding residual urine volume.7,8,9,10,11,12,13 However, these trials were performed in male patients with spinal cord injury and it seems hazardous to extrapolate their results to a different type of patient. Thus we designed this study to prospectively evaluate the efficacy and safety of botulinum A toxin in the treatment of detrusor sphincter dyssynergia in multiple sclerosis patients.
METHODS
This was a multicentre, placebo controlled, randomised, double blind study performed on two parallel groups. It was conducted in outpatient settings in university hospitals (five centres: Angers, Bordeaux, Brest, Paris, and Rennes) or in a rehabilitation clinic (one centre: Rennes Notre Dame de Lourdes). The protocol (no. 98/23–185) was approved by the “Comité Consultatif de Protection des Personnes dans la Recherche Biomédicale” of Rennes (France) on June 10, 1998. All patients gave written informed consent to participate.
Patients
Patients over 18 years of age and suffering from multiple sclerosis with detrusor sphincter dyssynergia were screened for enrolment. The diagnosis of multiple sclerosis had to have been made according to Poser criteria14 at least 6 months before inclusion. Detrusor sphincter dyssynergia was defined as involuntary contractions of the external urethral sphincter during detrusor contraction and micturition. Patients were included if urodynamic investigation showed a post-voiding residual urine volume between 100 and 500 ml. Patients were excluded if they had urine or prostate febrile infection, perineal skin disorders, or myasthenia, or if they took any treatment which could have altered neuromuscular transmission. Pregnant women or non-menopausal women who did not take effective contraception were also excluded.
Pre-inclusion evaluation
A complete medical check up of each patient with multiple sclerosis was performed including determination of the Expanded Disability Status Scale (EDSS),15 and the duration and type of urinary disorders. Data were collected on the following variables: obstructive symptoms, pollakiuria, urgencies and incontinence (voiding variables assessed using 10 cm visual analogue scales with 0 = worst and 10 = best), the International Prostatism Symptom Score (IPSS),16 and voiding volume and post-voiding residual urine volume (the latter being measured using a catheter).
An urodynamic investigation was performed to measure urethral, detrusor, and rectal pressures. This was associated with an electromyographic examination of the external striated sphincter performed with a co-axial needle. During this investigation, the bladder was filled at 50 ml/min. Data were collected on the following variables: maximal and cloture urethral pressures, basal detrusor pressure, pre-micturition and maximal detrusor pressures, detrusor compliance at functional bladder capacity, maximal bladder capacity, and maximal urinary flow. The type of dyssynergia was determined according to the Blaivas classification.2
Randomisation and treatment preparation
Randomisation was stratified on each participating centre and computer generated lists equilibrated every four patients were kept in the centre pharmacies. To randomise a patient, the investigator had to phone the pharmacist of his/her centre. In turn, the pharmacist attributed to the patient the first number which was available on the randomisation list of his/her centre. The pharmacist then prepared a syringe containing either the botulinum A toxin (100 U Allergan; Allergan Pharmaceuticals, Westport, County Mayo, Ireland) diluted in 4 ml of preservative free 0.9% saline or the placebo (4 ml of preservative free 0.9% saline, making the placebo preparation indistinguishable from the botulinum A toxin preparation), according to the randomisation list. The syringe was then brought to the investigator by a pharmacist’s assistant unaware of its contents. The day of randomisation, which was also the day of treatment injection, was day 0 (D0) of the study.
Treatment injection
The treatment was administered as a single transperineal injection using striated sphincter electromyography: the co-axial needle was inserted on the median line 2 cm above the anal margin for men or in the upper external or internal quarter above the urethral meatus for women, allowing the striated sphincter to be localised. The injection was performed after having verified that the needle was not inserted in a vessel.
In addition, each patient was prescribed an alpha blocker (5 mg tablet of slow release alfuzosin bid) over 4 months.
Outcomes
The primary efficacy endpoint was the post-voiding residual urine volume at D30. Secondary efficacy endpoints included voiding and urodynamic variables (see the lists of these variables in the first and second paragraphs, respectively, of the “Pre-inclusion evaluation” subsection above) at D30, and the evolution with time of voiding variables at D30, D60, D90, and D120.
Statistical hypotheses and sample size estimates
A retrospective study on 43 patients with detrusor sphincter dyssynergia managed in the rehabilitation centre of Rennes University Hospital showed that mean (standard deviation, SD) post-voiding residual urine volume was 220 (120) ml. Analysis of the literature led us to hypothesise that the alpha blocker could reduce the mean post-voiding residual urine volume to 170 ml at D30.
In order to stop the study as soon as sufficient information had been collected, we chose a sequential method, the single triangular test (see appendix).17,18 The test was designed to allow the detection of a difference between groups on the main endpoint of 70 ml (that is, a reduction of post-voiding residual urine volume from 170 to 100 ml at D30) with 90% power, the type I error (one sided) being set at 5%.19 Under these conditions, we determined, using PEST 3.0 statistical software (The Pest Project, Reading, UK), that the average sample size was 58 (90th percentile = 88) under the null hypothesis, 64 (90th percentile = 97) under the alternative hypothesis, 76 (90th percentile = 112) midway between the null and alternative hypotheses, and the maximum sample size (corresponding to the apex of the triangle) was 170. Moreover, the equivalent fixed sample design would have required 100 patients.
Statistical analyses
Statistical analyses were performed on an intention to treat basis.
Sequential analysis
The monitoring and sequential analyses were performed on the main endpoint for efficacy every 20 patients with PEST. Once the trial was stopped, the final analysis on the main endpoint was also performed with PEST, allowing an unbiased estimate of each treatment effect and a significance level taking into account the sequential nature of the analyses to be obtained.
Final analysis
A standard statistical analysis was performed on secondary endpoints with SAS statistical software (SAS Institute, Cary, NC). Student’s t test was used for comparison of continuous variables and χ2 test (or Fisher’s exact test when appropriate) was used for comparison of categorical variables. An analysis of covariance with repeated measures adjusted on baseline values was used for comparison of the continuous variables repeatedly assessed at D30, D60, D90, and D120.
Reported values are expressed either as means (SD) (continuous variables) or as frequencies of observed values and corresponding percentages (categorical variables).
RESULTS
Study population
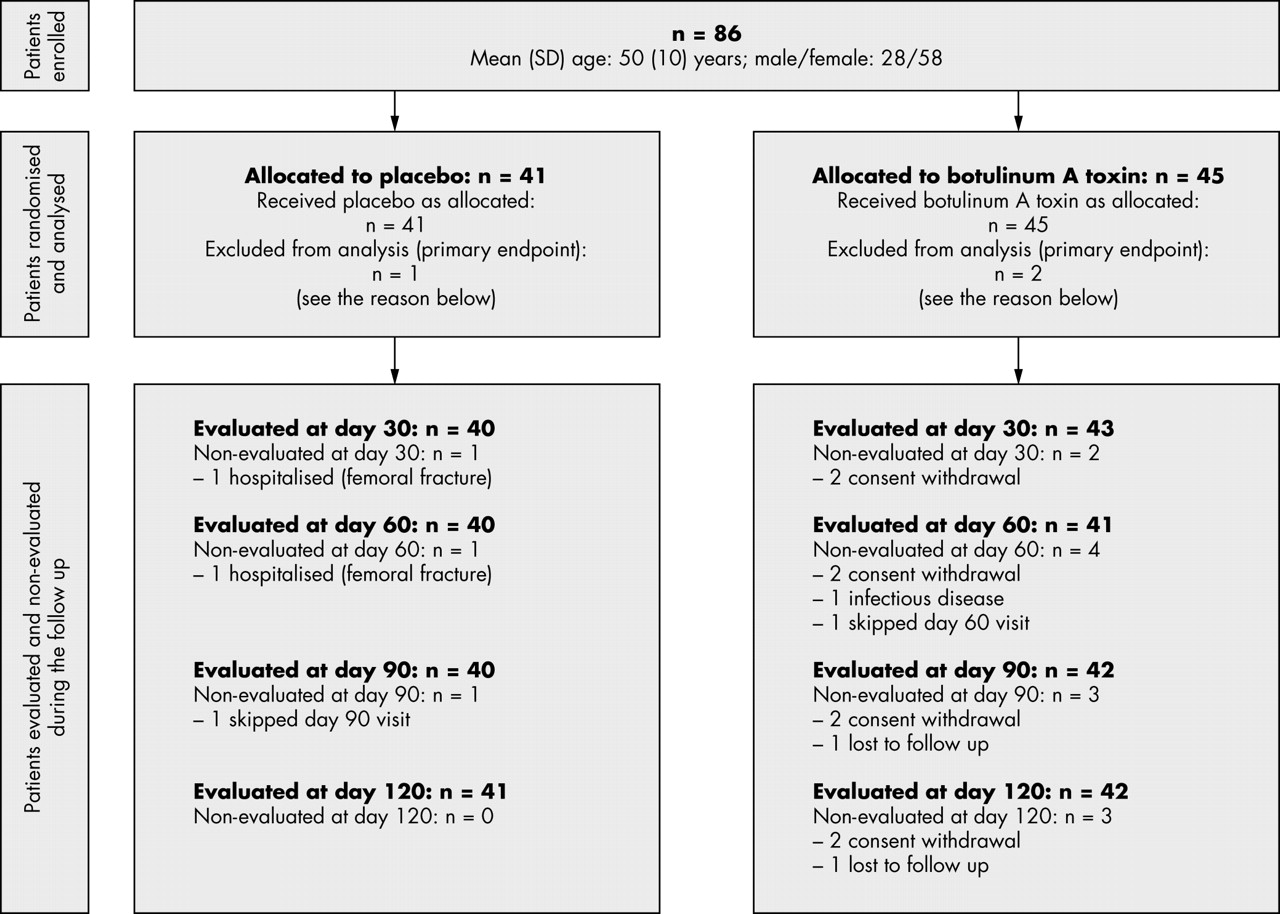
Eighty six patients (placebo: 41, botulinum A toxin: 45) were recruited in the six centres between November 27, 1998 and November 12, 2001. There was no difference between groups at inclusion as regards age, sex ratio, time from onset of multiple sclerosis, EDSS, time from onset and type of urinary disorders, proportion of patients previously taking an alpha blocker (table 1), and voiding and urodynamic variables (table 2). Mean (SD) post-voiding residual urine volume was 217 (96) and 220 (99) ml in the placebo and botulinum A toxin groups, respectively. According to Blaivas classification, detrusor sphincter dyssynergia could be classified as type 2 in 14 and 18 patients and as type 3 in 18 and 20 patients in the placebo and botulinum A toxin groups, respectively. Fifteen patients (eight and seven patients in the placebo and botulinum A toxin groups, respectively) could not be classified and one patient (placebo group) was not assessed.
General characteristics of study patients at inclusion
Voiding and urodynamic variables at inclusion
Figure 1 is a flow chart of the study. During the study, two patients withdrew consent before D30 and one patient was lost to follow up after D60. These three patients were in the botulinum A toxin group. One patient in the placebo group was not evaluated on D30 because of hospitalisation in another centre for the treatment of a femoral fracture. Thus, 83 patients (placebo: 40, botulinum A toxin: 43) were evaluated on the main endpoint (D30) and 83 patients (placebo: 41, botulinum A toxin: 42) completed the study (D120).
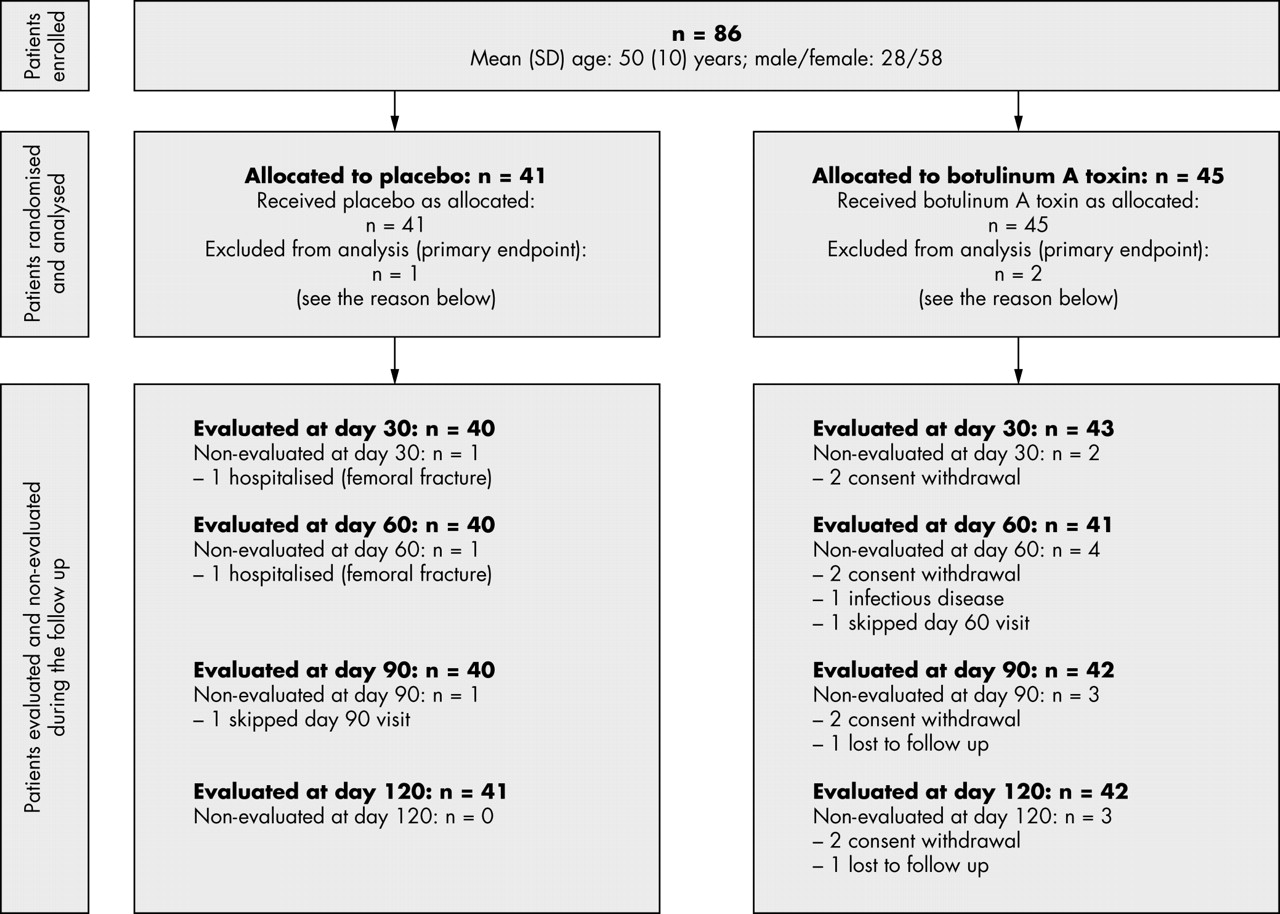
Flow chart of the study.
Treatment efficacy
Main endpoint (sequential analysis)
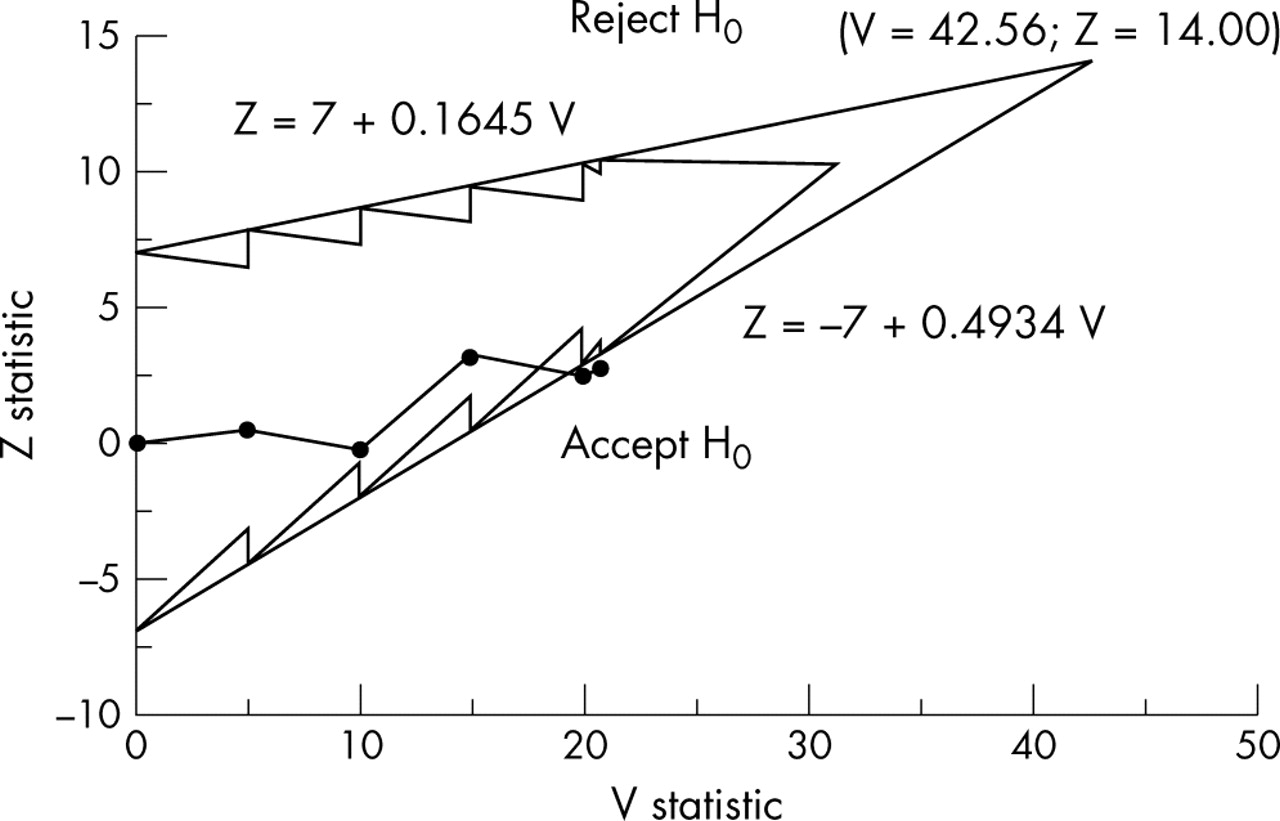
Figure 2 shows the triangular test and the corresponding sample path. The trial was stopped after the fourth analysis (the analysis was performed on 80 patients, placebo: 39, botulinum A toxin: 41) without rejection of the null hypothesis. By the time the result of this analysis was available, three more patients had been enrolled in the study. These patients were included in the final sequential analysis with use of the overrunning procedure. Mean (SD) post-voiding residual urine volume was 206 (145) and 186 (158) ml (p = 0.45) in the placebo and botulinum A toxin groups, respectively (table 3). Unbiased median estimates of post-voiding residual urine volume at D30 were 208 and 182 ml in the placebo and botulinum A toxin groups, respectively (unbiased estimates taking into account the sequential nature of the analysis).
Voiding and urodynamic variables at D30

Triangular test and sample path.
Secondary endpoints at D30
Compared to placebo, botulinum A toxin significantly increased voiding volume (+54%, p = 0.02) and decreased pre-micturition (−29%, p = 0.02) and maximal (−21%, p = 0.02) detrusor pressures (fig 3), and tended to reduce maximal (−15%, p = 0.11) and cloture (−21%, p = 0.07) urethral pressures but did not significantly affect the other urodynamic variables (table 3). There was no significant difference between groups on the quality of voiding as assessed using 10 cm visual analogue scales and the IPSS (table 3).
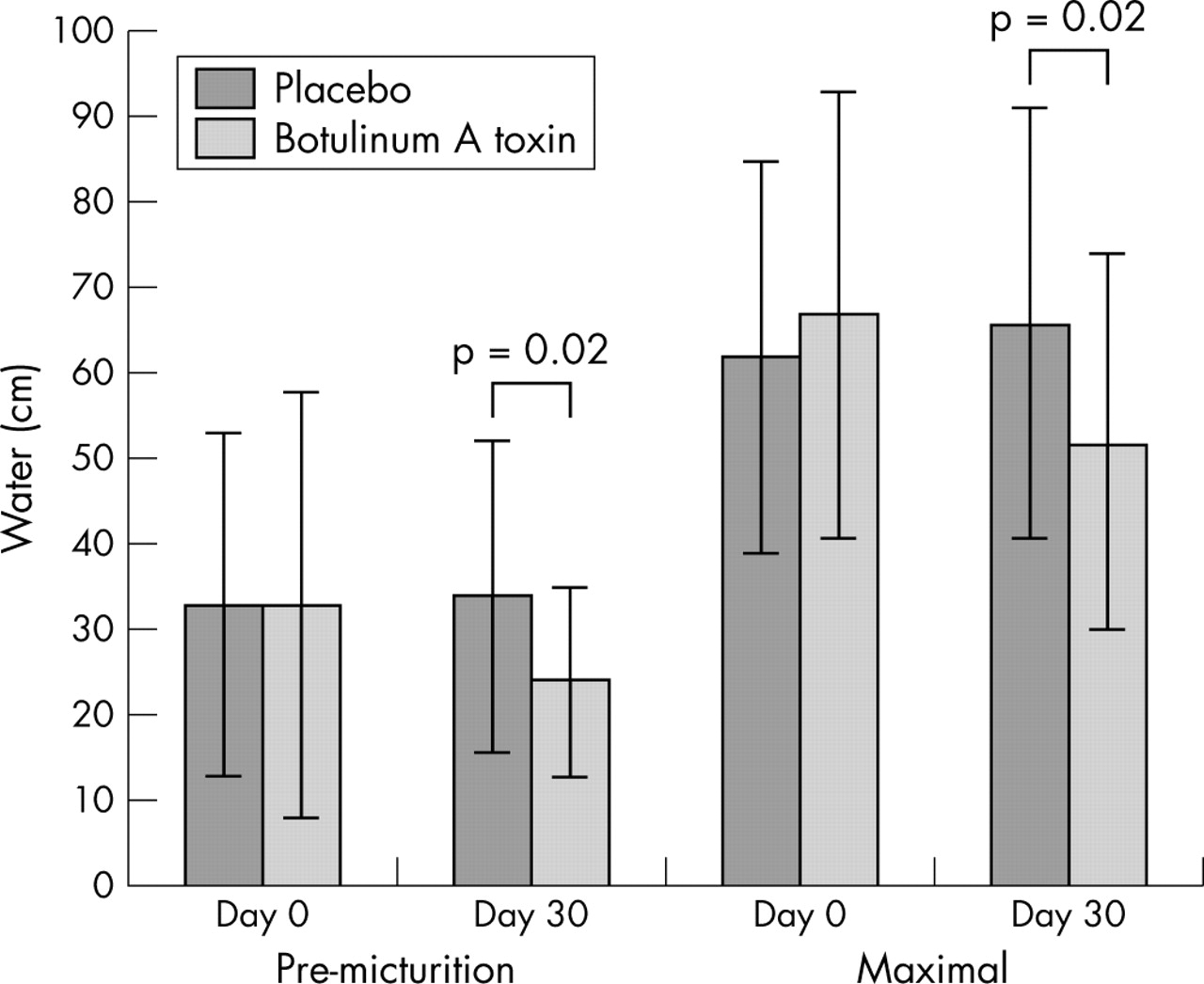
Pre-micturition and maximal detrusor pressures.
Secondary endpoints repeatedly assessed until D120
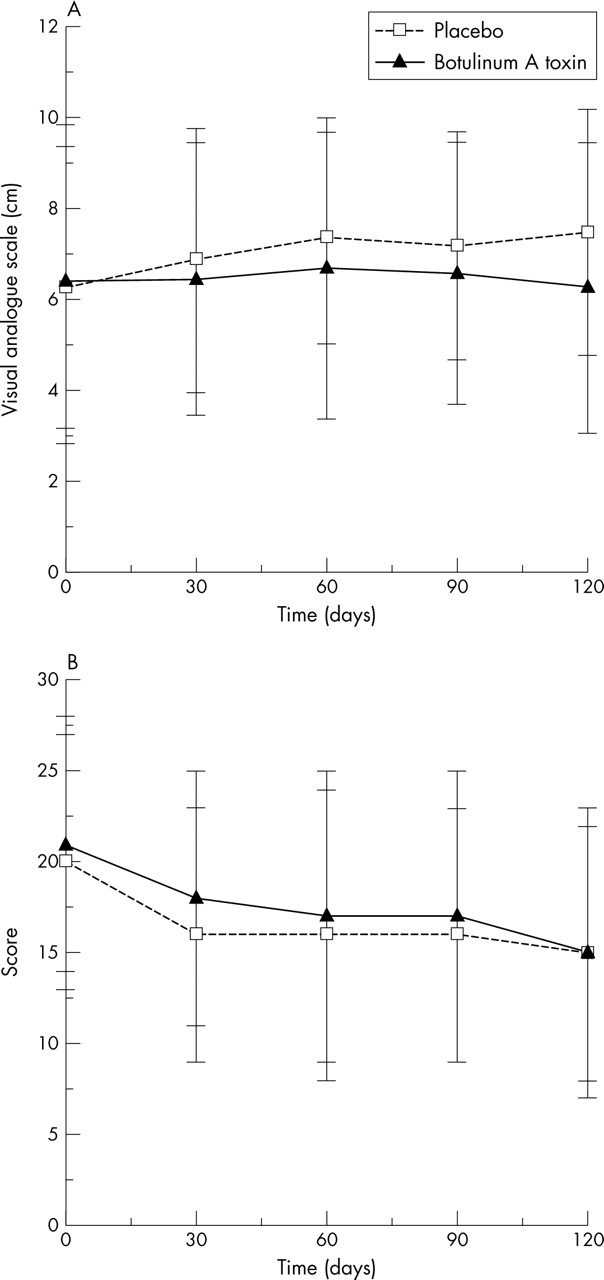
Botulinum A toxin significantly increased voiding volume, mainly at D30 and D60 (time effect: p = 0.81; treatment effect: p = 0.05; time×treatment interaction: p = 0.08; fig 4), without decreasing post-voiding residual urine volume (time effect: p = 0.28; treatment effect: p = 0.77; time×treatment interaction: p = 0.65; fig 4). There was no significant effect of botulinum A toxin on most of the variables which assessed the quality of voiding (obstructive symptoms, pollakiuria, urgencies) except incontinence which was slightly but significantly increased between D60 and D120 (time effect: p = 0.74; treatment effect: p = 0.04; time×treatment interaction: p = 0.56; fig 5). The IPSS significantly improved in both groups during the 4 months of follow up, but there was no significant effect of botulinum A toxin (time effect: p = 0.04; treatment effect: p = 0.79; time×treatment interaction: p = 0.48; fig 5).

Time course of voiding volume (A) and post-voiding residual urine volume (B). (A) ANCOVA adjusted on baseline values. Time: p = 0.81; treatment: p = 0.05; time×treatment interaction: p = 0.08; (B) ANCOVA adjusted on baseline values. Time: p = 0.28; treatment: p = 0.77; time×treatment interaction: p = 0.65.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Time course of incontinence (A) and International Prostatism Symptom Score (B). (A) ANCOVA adjusted on baseline values. Time: p = 0.74; treatment: p = 0.04; time×treatment interaction: p = 0.56. (B) ANCOVA adjusted on baseline values. Time: p = 0.04; treatment: p = 0.79; time×treatment interaction: p = 0.48.
Treatment safety
Twelve serious adverse events were reported in 11 different patients during the follow up. All of them were declared in the context of hospitalisation, in most cases in relation to an attack of multiple sclerosis (two and four patients in the placebo and botulinum A toxin groups, respectively). Other serious adverse events were pyelonephritis, lumbar radicular pain, and femoral fracture (one patient in the placebo group for each event), and uterine leiomyoma, drug induced confusion, and dyspnoea (one patient in the botulinum A toxin group for each event). No serious adverse event could be attributable to botulinum A toxin. Sixty four non-serious adverse events were also reported in 45 patients during the follow up. Thirty eight urinary tract infections were reported in 12 (29%) and 16 (36%) patients (p = 0.53), nine attacks of multiple sclerosis were reported in three (7%) and six (13%) patients (p = 0.49), four urinary leakages were reported in two (5%) and two (4%) patients (p = 1.00), in the placebo and botulinum A toxin groups, respectively. Moreover, one faecal incontinence was reported in one patient of the botulinum A toxin group.
DISCUSSION
The patients included are clearly those that were expected and they can be considered to be representative of a population of patients suffering from multiple sclerosis with detrusor sphincter dyssynergia. Indeed, all subjects had a post-voiding residual urine volume at inclusion between 100 and 500 ml with a mean (SD) value of 218 (97) ml, very close to the 220 (120) ml expected at the planning phase. However, the alpha blocker did not show the expected effect (206 ml in the placebo group at D30 instead of the anticipated 170 ml) and the difference between the two groups at D30 was clearly lower than expected (20 instead of 70 ml). This result on the main endpoint strongly contrasts with the results reported in spinal cord injury. This is all the more interesting as the type of toxin, dose injected, and schedule of administration correspond to those generally used in the most recently published studies in spinal cord injury. Indeed, the first studies performed in patients with detrusor sphincter dyssynergia generally evaluated repeated (weekly or monthly) administrations of larger doses of botulinum A toxin.7–9 However, the risks of side effects and auto-immunisation along with the long duration of action of botulinum toxin progressively led to single injections of either 70–100 U Allergan or 150 U Speywood (Speywood Pharmaceuticals, Wrexham, Clywd, UK).10–13 Moreover, a significant treatment effect has been found on post-voiding residual urine volume at D30 using the same type of toxin, dose injected, and route of administration in spinal cord injury.13
In this context, two explanations can be discussed.
Firstly, the diseases. There are some differences between spinal cord injury and multiple sclerosis, not only in the distribution of genders, the former being observed almost exclusively in males and the latter being more balanced with a slight predominance of females, but also in pathophysiological features. Indeed, it has been underlined that detrusor pressures during voiding are higher in spinal cord injury than in multiple sclerosis.3 In spinal cord injury, these high detrusor pressures are probably linked not only to detrusor sphincter dyssynergia but also to the bladder over-activity which results from disruption of inhibiting supra-spinal pathways, neuroplasticity in bladder efferent and afferent neurones, and structural changes in detrusor smooth muscle.20,21 In multiple sclerosis, cortical centres are involved and total medullar disruption is rarely observed. Moreover, in multiple sclerosis, patients never suffer from autonomic dysreflexia as in spinal cord injury.22 These differences could explain the lower response to botulinum toxin.
Secondly, the methodology of published studies.7,8,9,10,11,12,13 All studies but two (performed in five and 13 patients, respectively)8,13 were non-controlled trials performed on small samples. In most of these studies, the post-voiding residual urine volume observed at the time of evaluation was compared to the value observed at the time of inclusion. Thus, it is also possible that botulinum toxin efficacy was overestimated in spinal cord injury due to the lack of a control group and therefore to the lack of randomisation and blindness.
The results on the secondary urodynamic endpoints are in line with those reported in spinal cord injury. They indirectly demonstrate that the lack of effect on the main endpoint is not the result of failure to deliver the botulinum toxin in the right place. They suggest that botulinum A toxin could contribute to protecting the upper urinary tract. Indeed, it is well known that high bladder pressures are connected to upper urinary tract complications. Indeed, a high correlation between type 3 detrusor sphincter dyssynergia and hydronephrosis has been reported.3 Although such a risk of complications is less important than in spinal cord injury, it has been estimated to be up to 55% and increases with the level of handicap.3,4 Many of our patients could therefore be considered to be at risk of urological complications. Thus, the significant reduction of pre-micturition and maximal detrusor pressures could contribute to decreasing the risk of urinary tract damage. However, this potential advantage has to be balanced against the risk of incontinence which is slightly increased.
CONCLUSION
In multiple sclerosis patients with detrusor sphincter dyssynergia, a single injection of botulinum A toxin (100 U Allergan) does not decrease post-voiding residual urine volume. General tolerance is good, but the risk of incontinence is slightly increased.
APPENDIX: PRINCIPLE OF THE TRIANGULAR TEST
The triangular test uses a sequential plan defined by two perpendicular axes. The horizontal axis corresponds to a first statistic V which represents the quantity of information accumulated since the beginning of the trial. The vertical axis corresponds to a second statistic Z which represents the benefit with the experimental treatment as compared with the control. Two straight lines, called the boundaries of the test, delineate a continuation region (situated in between these lines) from the regions of non-rejection and of rejection of the null hypothesis. The boundaries intersect, thus defining a closed continuation region with a triangular shape. The equations of the boundaries depend on the values of the benefit to detect, of its standard deviation, and on the type I error and power, as well as on the frequency of the analyses, defined in terms of the number of patients included between two analyses. Because this number usually varies at each analysis, the boundaries need to be adjusted concomitantly, thus defining a continuation region with a Christmas tree shape.
At each analysis, Z and V are computed from all the data collected since the beginning of the study and Z is plotted against V, thus defining a point on the sequential plan. The consecutive points define a sample path. The trial is continued and new patients are included as long as the sample path remains in the continuation region. A conclusion is reached as soon as the sample path crosses one of the boundaries of the test: if the sample path crosses the upper boundary, the experimental treatment is demonstrated to be significantly superior to the control; if the sample path crosses the lower boundary, the experimental treatment is not significantly different from the control.
Acknowledgments
We wish to thank Allergan Pharmaceuticals Ltd, Westport, Ireland, who graciously provided us with botulinum A toxin.
REFERENCES
Footnotes
-
This study was supported by the Fondation pour la Recherche Médicale, Paris (France), the Comité de la Recherche Clinique du Centre Hospitalier Universitaire de Rennes, Rennes (France), the Groupe d’Etude de Neuro-Urologie de Langue Française, Paris (France), and the Association pour la Recherche dans la Sclérose en Plaques, Paris (France). None of the above mentioned funding organisation participated in the design, conduct, interpretation, or analysis of the study or review or approval of the manuscript.
-
Competing interests: none declared
-
Study organisation: study chairmen: Philippe Gallien (principal investigator) and Eric Bellissant (methodologist); monitor: Jean-Michel Reymann; sequential statistical analysis: Véronique Sébille; data management and standard statistical analysis: Habiba Mesbah; quality assurance: Marie-Françoise Mordelet; clinical research assistant: Christelle Tual.
In addition to the authors, study investigators and institutions were as follows: M-P Dorval, Service de Médecine Physique et Réadaptation, Centre Hospitalier Universitaire, Brest, France and P Brunel, Service de Médecine Physique et Réadaptation C3RF, Centre Hospitalier Universitaire, Angers, France.