Article Text

Abstract
A greater understanding of the natural history of acute pancreatitis combined with greatly improved radiological imaging has led to improvement in the hospital mortality from acute pancreatitis, from around 25–30% to 6–10% in the past 30 years. Moreover, it is now recognised that the first phase of severe acute phase pancreatitis is a systemic inflammatory response syndrome (SIRS), during which multiple organ failure and death often supervene. Survival into the second phase may be accompanied by local complications, such as infected pancreatic necrosis, which may be prevented by prophylactic antibiotics and treated by judicious surgery. Intensive care unit costs can be substantial, but might be justified because of the excellent quality of life of survivors. Reduction in multiple organ failure by agents such as lexipafant, an antagonist of platelet activating factor (PAF) (which plays a critical role in generating the SIRS), may contribute to intensive care unit cost containment, as well as reducing the incidence of local complications and deaths from acute pancreatitis. A further improvement in the human and financial costs also requires the centralisation of the management of patients with severe acute pancreatitis, to single hospital units whose concentrated expertise equips them to intervene most effectively in what is still recognised as a highly complex disease.
Statistics from Altmetric.com
Acute pancreatitis is a common disease with a relatively high morbidity and mortality.1-5 The aetiology of acute pancreatitis is varied and the outcome for an individual patient can be difficult to predict from the outset. The incidence has been reported to be as high as 38 per 100 000 population per year and seems to be increasing.4 ,6 Around 25% of patients will develop severe or life threatening complications which require high dependency nursing or intensive care support.1 ,2 ,5
Over the past 30 years or so the mortality has fallen from around 25–30% to 6–10%, but has now remained at that level for a decade or more.1-11 The initial improvement occurred principally because of better definition of the natural history of the disease,12 ,13 refined imaging techniques for identifying complications at an earlier stage during its pathogenesis,12 ,14 advances in critical care support,1 ,15 and avoidance of major surgery where it could increase morbidity and mortality.5 ,9 ,16 ,17Failure to even entertain, and hence make, the diagnosis of acute pancreatitis in patients admitted to medical and surgical wards has formerly, and may still, contribute to a higher mortality rate.3 ,4 ,18 A specific key development has been the recognition of extensive pancreatic necrosis12 ,13 and the distinction between infected and sterile pancreatic necrosis. This has enabled surgical necrosectomy to be targeted towards patients who may benefit from the intervention.5 ,9 More importantly, as clinically significant necrosis occurs in no more than 5% of patients with acute pancreatitis,2 extensive surgery which can undoubtedly contribute to an increased mortality can be avoided altogether.16 ,17 Similarly, patients with severe gallstone acute pancreatitis have an improved prognosis when bile duct stone clearance is undertaken via endoscopic sphincterotomy10 ,11 ,19 rather than via surgical techniques.16
Severe acute pancreatitis is now recognised to be a two phase systemic disease, comprising from the outset a (sterile) SIRS that may lead to multiple organ failure within the first 72 hours (fig1).20-23 SIRS is the clinical response resulting from widespread systemic effects of proinflammatory mediators, which is only termed sepsis when present with documented infection.24Unless this process is arrested and reversed by natural defences or therapeutic intervention, the second phase ensues, with progression to overt sepsis (usually becoming apparent in the second week of the illness) and local pancreatic and intra-abdominal complications.13 ,25 A vicious circle ensues which, unless interrupted by systemic measures and/or, in appropriate circumstances, treatment of local complications, results in irreversible multiple organ failure and death.1 ,15 ,26 Failure of more than one organ system from the outset is highly predictive of death.26 ,27

Schematic representation of the important pathways in acute pancreatitis leading to systemic inflammatory response syndrome (SIRS) and multiple organ failure. PAF, platelet activating factor; IL, interleukin, TNF-α, tumour necrosis factor α; PGE2, prostaglandin E2; TXA2, thromboxane A2; LT4, leukotriene series 4; IIs PLA2, type II (non-pancreatic) secretory phospholipase A2; NO, nitric oxide.
Inevitably, patients with severe disease remain ill for prolonged periods. Even within the resource restraints of the British health care system, the average intensive care unit stay is seven days with a total hospital stay ranging from 40 to 226 days.28 ,29 Yet patients who survive an attack of acute pancreatitis have a high probability of returning to normal activity and gainful employment.30 Counting the cost of treating patients with acute pancreatitis is coming under increasing scrutiny. The methodologies of hospital cost computation are rapidly evolving and problems pertain particularly to comparisons of different types of disease.31 Nevertheless it is clear that patients with severe acute pancreatitis are considerable consumers of health service resources.28 ,29
Successful research will enable the development of more effective treatment strategies. Already the recognition of the role of sepsis during the second phase of the disease has resulted in randomised trials of the use of prophylactic antibiotics.32 ,33Obtaining a defined end point in a complex systemic disease is not easy but these studies suggest a benefit in terms of major morbidity and/or mortality. Interrupting the disease during the initial phase, however, may offer the best prospects for success. Novel therapies targeted towards recently discovered intracellular processes need to be developed and tested.34-36 In addition, agents directed against the active molecules which are critical to the SIRS response, such as tumour necrosis factor α,37 interleukin (IL) 1,38 IL-2,39 and PAF,21 show considerable promise in reducing multiple organ failure.
Methodologies to analyse the human and financial costs of acute pancreatitis will need to be improved in order to evaluate better the benefits of emerging new therapies.
Classification and natural history
The Ulm (Germany) Group has done much to extend knowledge of the natural history of acute pancreatitis.9 ,12 ,26 In this system acute pancreatitis is related to the morphology of the gland: (1) parenchymal oedematous pancreatitis; (2) pancreatic necrosis which is divided into sterile and infected pancreatic necrosis; (3) pseudocyst; and (4) pancreatic abscess. The Atlanta Classification13 is an extension of this system in which the concept of mild and severe acute pancreatitis is incorporated into the morphological characteristics of the gland.
The use of high dose, intravenous, contrast enhanced computed tomography (CT) is the mainstay of determining the extent of pancreatic necrosis.12 ,14 This relation is imprecise,40however, and empirically derived prognostic systems such as the Glasgow clinico-biochemical method are just as good as prediction based on CT appearances.41 Moreover, a combination of morphological changes and clinico-biochemical criteria fails to improve the overall accuracy of prognostic prediction.41 Lesser degrees of necrosis—for example up to 30%, are a common feature of clinically mild acute pancreatitis.42 Extensive necrosis (more than 50%) is associated with systemic complications and/or the need to intervene surgically,9 ,42 but this will only arise in about 5% of the population of patients with acute pancreatitis.2 The extent of pancreatic necrosis may increase during the first or second week of the onset of the attack,14 with secondary infection resulting in infected pancreatic necrosis requiring surgical intervention occurring mainly from the second week onwards.26 ,43
Acute fluid collections lack a defined wall and may occur within or near the pancreas. By definition, pseudocysts contain pancreatic enzyme-rich fluid and are lined by a (non-epithelial) wall of granulation or fibrous tissue. They usually require four weeks or more to evolve.13 These fluid collections occur in association with either oedematous or necrotic pancreatitis, but their natural history is usually spontaneous resolution. Acute fluid collections arise in 30–50% of cases, and were previously often confused with pseudocysts. Such misdiagnosis may have accounted for the apparent high “success” rate of percutaneous aspiration. Although most acute fluid collections resolve, some may evolve into a pseudocyst which becomes clinically significant in 10–15% of cases.
A pancreatic abscess is a well defined collection of pus and arises usually very late (six weeks or more) in the evolution of acute pancreatitis.13 Abscesses occur in about 1% of cases13 and can usually be treated by percutaneous radiological aspiration.44 The mortality from pancreatic abscess is very low; previously quoted high mortality figures may have been elevated by confusion between pancreatic abscess and infected pancreatic necrosis (which has a mortality of 20–50%).5 ,20 An infected pseudocyst is, by definition, an abscess,13 whether caused by natural secondary infection or iatrogenically by percutaneous needling.
The absolute indications for surgical intervention in acute pancreatitis are infected pancreatic necrosis and pancreatic abscess, when percutaneous aspiration is unsuitable or has failed.5 ,9 ,42-45 Unresolving pseudocysts require surgical drainage procedures when percutaneous or endoscopic techniques have failed or are unsuitable. Surgery is also indicated for extensive pancreatic necrosis with a deteriorating clinical picture as percutaneous catheter drainage is usually unsuccessful, particularly in the presence of semisolid necrosis.46 Intervention is required in up to 20% of cases for local complications, specifically, extensive pancreatic necrosis (usually >50%), infected pancreatic necrosis, pseudocyst, abscess, and haemorrhage.1 ,15 ,46
Haemorrhage caused by vessel erosion forming a pseudoaneurysm or bleeding into the retroperitoneal or peritoneal spaces may occur rarely, as does colonic necrosis.45 Bleeding into a pseudocyst may result in a spontaneous rupture.45 Fistulae into the bowel may also occur spontaneously, but more often arise in association with repeated laparotomies or inopportune use of surgically or radiologically positioned drains.45
Despite improvements in the understanding of the natural history of acute pancreatitis, several interconnected issues remain unresolved. Why is the relation between local pancreatic pathology and outcome relatively imprecise?41 How does central pancreatic necrosis compare with peripheral pancreatic necrosis in determining outcome?47 There may be massive extrapancreatic inflammatory infiltration and necrosis in the face of overwhelming multiple organ failure, and yet the pancreas is affected only by relatively mild inflammatory oedematous changes.
Death within the first week of illness is usually caused by systemic complications, notably organ failure.26 ,27 Death from local complications is more common after the first week, especially if infection supervenes.15 ,46 Pancreatic necrosis by itself is not particularly predictive of mortality, but if multiple organ failure is present also, mortality is higher.27
Prognostic systems of severity
Clinical assessment of severity has been shown to be notoriously unreliable when made in the 48 hours after disease onset.48 Yet the ability to predict the severe group of patients would be of great value. Most patients fall into a mild or severe group from the outset, and only a small proportion of patients progress from a mild attack in the first week of illness to a severe attack. The value of an accurate prognostic method is threefold: (1) to identify patients requiring intensive monitoring and support from the outset; (2) to institute measures to interrupt the progression of a severe attack; and (3) to permit comparison of patient groups between different controlled studies.
Although prognostic systems have been of enormous value in showing equatability of groups in randomised trials, they are generally inadequate to identify patients with severe disease—that is, those who develop organ failure and/or local complications.13 All systems provide optimum accuracy only at 48 hours following the onset of symptoms.48-50 The clinico-biochemical systems are only about 80% accurate at 48 hours and are not accurate at all before this time.48-50 The APACHE II system,51which has the best overall accuracy of all the systems,26 ,49 has the sensitivity of predicting a severe attack in only 61% of patients on admission.49 Single factor systems, such as serum measurement of C-reactive protein or IL-6,24 also lack accuracy before 48 hours.24Measurement of polymorphonuclear elastase,52 has not fulfilled its initial promise in subsequent studies, and some of the most recent factors to be measured, such as serum trypsinogen activation peptide53 and trypsin 2-α1-antitrypsin complex,54 have yet to be validated. The weakness of all of these systems is that the positive predictive values for severe patients are only of the order of 40–60% and the sensitivity is only 60–80%.26 ,48-50 This means that 20–40% of patients with severe disease will not be detected by these systems before it becomes clinically apparent that a patient is deteriorating, and therefore the window of opportunity for therapeutic intervention may be missed. As discussed previously, contrast enhanced CT imaging fares no better than other prognostic systems.40
It is important to recognise two fundamental points in relation to prognostic systems in acute pancreatitis. Firstly, that their use in randomised trials should not result in a false sense of security: although most patients with mild disease can be selected out, a high proportion of severe cases will be misclassified.26 ,48-50 Secondly, although inadequate, they remain better than clinical judgement.48 From a pragmatic viewpoint, there should be universal application of the simpler prognostic systems (such as the Glasgow score) but the threshold of clinical judgement in recognising a patient as having a potentially severe attack should be relatively low. Moreover, the management of patients with acute pancreatitis should be focused into a single hospital unit where expertise is high, rather than the usual method of being dispersed across many specialties.
Multiple organ failure
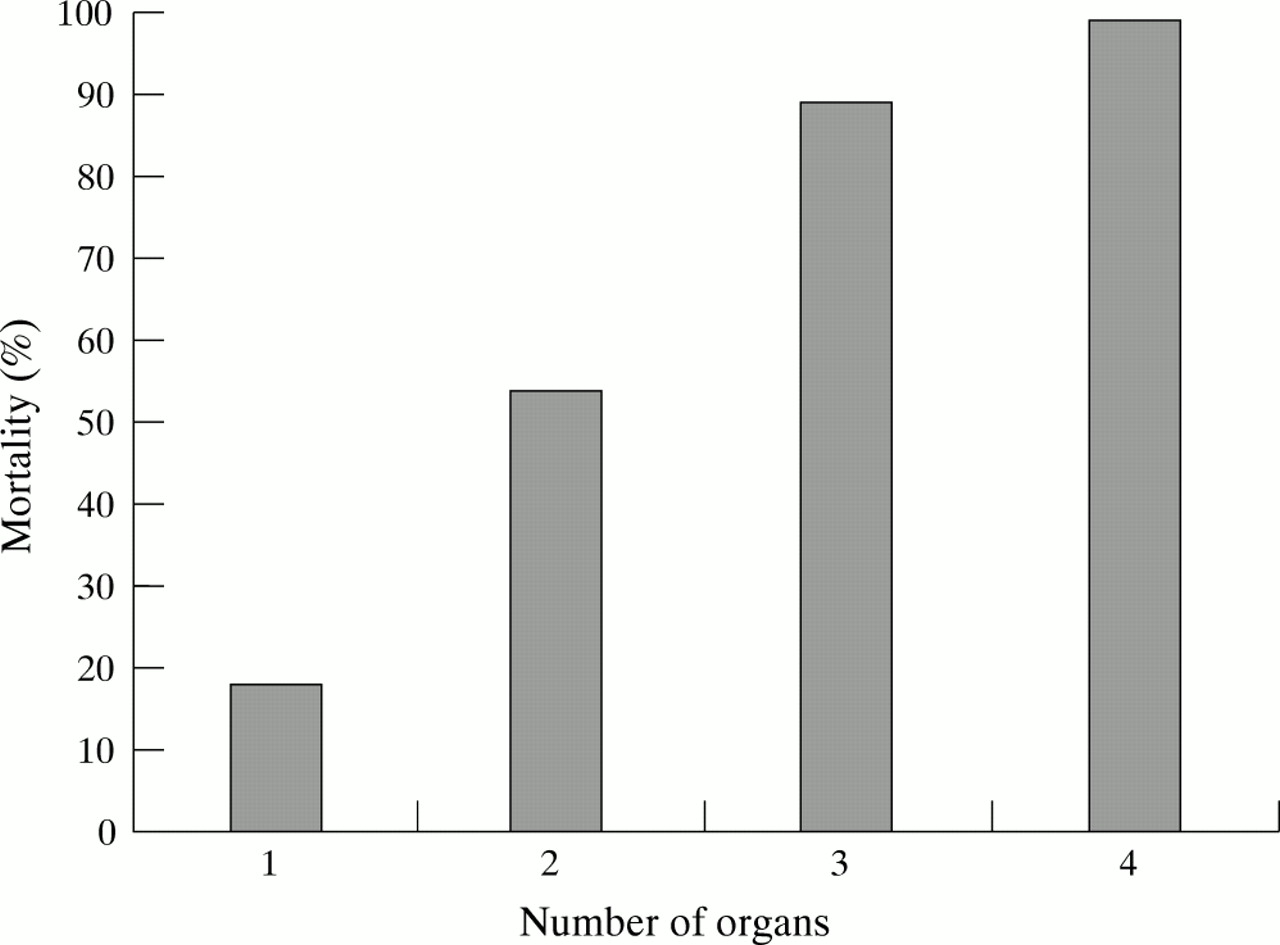
Although the natural history of local complications has become better defined and the indications for intervention have been greatly clarified, the pathogenesis, prevention and treatment of multiple organ failure must be tackled before any significant further advance can be made in acute pancreatitis. Multiple organ failure is defined as a syndrome of progressive but potentially reversible organ failure, involving two or more systems remote from the original insult. Symptoms may range from mild transient dysfunction to irreversible organ failure. The prognosis for the patient is closely related to the number of organs that have failed.27 ,55 Organ system failure complicates up to 92% of deaths26 and failure of more than one organ greatly increases the risk of death (fig2).26 ,27 ,55 The pulmonary, renal, cardiovascular, central nervous, and coagulation systems, in addition to the gastrointestinal tract,55 ,56 are most commonly affected. Other systemic complications include hypocalcaemia and hyperlipidaemia.56

{kind=link}
{kind=link}
Rising mortality in acute pancreatitis with increasing number of organs affected (adapted from Heath et al26).
Necropsy findings have confirmed clinical observations that pulmonary complications are a significant factor contributing to death, even if only moderate pancreatic damage is present.57 This study found that nearly 60% of deaths occurred within seven days of the onset of the attack and were associated with pulmonary damage. Arterial hypoxaemia occurs in more than 60% of patients during the first 48 hours of an attack and adult respiratory distress syndrome may occur in up to 20% of patients.46 Renal failure may supervene in up to 20% of cases and results in a mortality as high as 80%. Cofactors contributing to multiple organ failure include advanced age56 (although some studies dispute this), diabetes mellitus,57 smoking58 and obesity.5 ,59 ,60 Current treatment of multiple organ failure focuses on the prevention of organ injury and on supportive care, including source control, restoration and maintenance of oxygen transport and metabolic support.61 ,62
Management of severe acute pancreatitis on the intensive care unit
Patients with severe acute pancreatitis on the intensive care unit are among the most resource demanding in intensive care medicine.15 The mainstay of management is intensive monitoring and organ support, including (as required) intravenous fluid replacement, oxygen therapy and artificial ventilation, use of inotropes, prevention of stress ulceration, renal support by haemoperfusion and haemofiltration, pain relief, and nutritional support. Despite some continued controversy, all are agreed that urgent endoscopic sphincterotomy is required in gallstone induced bile duct obstruction in severe acute pancreatitis.10 ,11 ,19 ,63The case for prophylactic systemic antibiotics in severe acute pancreatitis has been strengthened by both clinical and experimental studies.30 ,31 ,64
Monitoring must include a baseline contrast enhanced CT scan or magnetic resonance imaging, repeated at least weekly or until there are signs of improvement. In the face of extensive pancreatic necrosis (usually >50%) and continued clinical deterioration, surgical necrosectomy is indicated, but under normal circumstances should not be considered until the start of the second week of illness.42 ,43 If there are doubts regarding surgical intervention, CT guided needle aspiration of necrotic areas of the pancreas should be performed to check for the presence of microorganisms.25 ,43 ,46 The demonstration of complete pancreatic duct disruption in the head of the gland by endoscopic retrograde cholangiopancreatography (ERCP) is indicative of central pancreatic necrosis, and may be an important indication for intervention.47
An early interruption of the initial SIRS phase of acute pancreatitis could greatly improve outcome by minimising multiple organ failure and preventing progression to the second phase of the disease. This latter phase is characterised by the development of local complications which in turn promote continuing remote organ failure. Antibiotics seem to act by reducing the infective complications of the second phase,32 ,33 but they do not abort the SIRS phenomenon to any significant degree.62 A variety of treatments have been used to try to prevent SIRS, including the use of antiproteolytic therapy,65 glucagon,8calcitonin,8 somatostatin,66atropine,66 peritoneal lavage,67 and fresh frozen plasma,68 ,69 but with a singular lack of success. The prophylaxis of ERCP induced acute pancreatitis by gabexate,70 an antiproteolytic agent, is controversial, as any therapeutic effect of this agent on established acute pancreatitis was insignificant in one multicentre study,71 and small in a subsequent meta-analysis.72
A paradigm shift has taken place, however, as a novel agent targeted against one of the key components of the SIRS phenomenon has shown beneficial responses in clinical73-75 as well as experimental studies.21 ,22 PAF is a bioactive lipid critically involved in neutrophil and endothelial activation, promoting neutrophil rolling along the endothelial surface, neutrophil–endothelial adhesion in conjunction with upregulation of cell adhesion molecules and neutrophil transmigration.21 ,22 ,76-78 To this extent PAF is somewhat of a misnomer, although it will indeed activate platelets also.
Lexipafant is one of a class of powerful antagonists of PAF which has been shown to reduce significantly multiple organ failure from acute pancreatitis in phase II trials73 ,74 and confirmed in a recent UK based phase III double blind randomised trial involving 290 patients with a high APACHE II score.75 This latter trial also showed a significant reduction in the development of pseudocysts in the lexipafant group (14 v 5%) and when administered within 48 hours of the onset of symptoms, significantly reduced mortality from 17 (18%) deaths out of 95 placebo treated patients to eight (8%) deaths out of 104 lexipafant treated patients.75 The results of a concurrent North American led multinational randomised trial of lexipafant are eagerly awaited, although the UK study is one of the largest randomised studies in acute pancreatitis ever conducted.
Cost effectiveness and quality of life
The reduction in the human cost of any disease, including acute pancreatitis, by advanced technological treatments (including the newer pharmacological agents) can only be sustained if the relative financial cost can be contained. The cost of intensive care unit care is considerable in all health care systems. In the UK the estimated daily cost of intensive care unit care is £1500 per patient per day.79 In the USA the estimate is US $3000–4000 per patient per day80 and accounts for 1% of the gross domestic product.81 For acute pancreatitis, the individual patient costs are probably even higher.28 For comparison, the cost of mechanical ventilation in the elderly (who comprise only a small proportion of patients on the intensive care unit) is equivalent to as much as 50% of all intensive care unit resources.81
Cost effectiveness analysis determines costs and benefits for a given set of alternatives, subsequently determining a ratio for each alternative. For health care, the costs are usually stipulated in monetary terms and benefits in numbers of survivors, years of survival, probability of survival or quality of life adjusted years (QALYs).81 In a recent study of patients with acute necrotising pancreatitis, the mean QALY gained per patient was 8.6 at a mean cost per QALY of £2157 using the assumption that all patients would have died without treatment and that patients who survived would have had a life expectancy of 75 years.28 The actual cost of treatment ranged from £9296 to £33 796, of which two thirds was attributable to hospitalisation, 20% to surgical and endoscopic interventions, and 16% to investigations.28 In a separate study of 37 patients with severe acute pancreatitis, followed up for an average of 6.2 years, 30 were in good health, and 24 out of 31 previously employed were back at work.30
More accurate systems are needed for costing intensive care unit care, not only for patients with acute pancreatitis.31 By and large intensive care units have been developed in most hospitals in a random manner and many of their real costs are absorbed into the general hospital budget.81 The development of alternative costing systems such as those based on the Therapeutic Intervention Scoring System (TISS) may prove to be more meaningful in the face of health care funding changes.82
Cost effectiveness implies that well validated (evidence based) diagnostic, prognostic and therapeutic procedures need to be applied generally. Failure to make a timely diagnosis of acute pancreatitis because—for example, the serum amylase was not measured or recorded in a patient with unexplained abdominal pain or because endoscopic therapy was instigated relatively late, may greatly increase the costs of subsequent care. Similarly, unnecessary, too early, or excessively delayed surgical intervention can lead to escalating intensive care unit costs.83 The introduction of novel agents such as lexipafant, which by dislocating the SIRS phenomenon can alleviate organ failure thereby reducing the human and financial costs of acute pancreatitis, are meaningful only provided the overall management remains optimal. This type of treatment may help to buy time for the patient and enable their transfer to a unit specialising in the management of acute pancreatitis. Such an approach should provide the best means of achieving cost effective care and quality of life in patients with severe acute pancreatitis.