Article Text

Abstract
Radiation to the mediastinum is a key component of treatment with curative intent for a range of cancers including Hodgkin's lymphoma and breast cancer. Exposure to radiation is associated with a risk of radiation-induced heart valve damage characterised by valve fibrosis and calcification. There is a latent interval of 10–20 years between radiation exposure and development of clinically significant heart valve disease. Risk is related to radiation dose received, interval from exposure and use of concomitant chemotherapy. Long-term outlook and the risk of valve surgery are related to the effects of radiation on mediastinal structures including pulmonary fibrosis and pericardial constriction. Dose prediction models to predict the risk of heart valve disease in the future and newer radiation techniques to reduce the radiation dose to the heart are being developed. Surveillance strategies for this cohort of cancer survivors at risk of developing significant heart valve complications are required.
Statistics from Altmetric.com
Mediastinal radiotherapy is used as part of the treatment regimen for a wide range of cancers including Hodgkin's lymphoma, non-Hodgkin's lymphoma, breast cancer and mediastinal testicular cancer. Hodgkin's disease has an incidence of 2.7 per 100 000 men and women per year with a peak incidence in the 20–34-year-old age group.1 The goal of therapy in patients with Hodgkin's lymphoma is curative.2 Treatment for early-stage Hodgkin's lymphoma is a combination of chemotherapeutic agents with radiotherapy as this may improve tumour control and survival.3 There has been a progressive increase in survival over the past few decades with 20-year survival now approaching 80%.4 ,5 Radiotherapy after breast-conserving surgery for early breast cancer reduces local recurrence and mortality.6 Furthermore, 20-year survival is around 60%.7
Radiation injury to the heart may manifest as accelerated coronary artery atherosclerosis, pericardial disease, myocardial systolic and diastolic dysfunction as well as valve disease.8 There is a long latent period before the effects of radiotherapy may manifest clinically. With increased long-term survival, there is a cohort of cancer survivors who are at risk of cardiovascular complications that potentially may have a major impact on outcomes and quality of life.
The purpose of this review is to identify the prevalence, pathophysiology, diagnostic modalities and optimal treatment of radiation-induced valvular disease. Furthermore, we identify factors that may predict future risk of valve disease and potential methods to modify this risk.
We searched for publications using PubMed containing terms ‘valvular’ or ‘valve’, ‘cardiac’ or ‘cardiovascular’ and one of the terms ‘radiotherapy’, ‘radiation’, ‘hodgkin’, ‘breast’, ‘testicular’, ‘cancer’. All publications from 1950 onwards were screened for use in this review.
Prevalence
Over the past three decades, investigators have attempted to identify the prevalence of radiation-induced valve disease (table 1).9–24 There is large variation in the prevalence between studies. This may be related to differences in study design, controls and inherent bias.
Summary of studies identifying valve disease in patients previously treated with mediastinal radiotherapy
Between 2% and 37% of patients who have previously received mediastinal irradiation for Hodgkin's lymphoma will develop valve disease (table 1). Two early studies by Gustavsson et al9 and Kreuser et al10 found a high prevalence of valve thickening (40–43%) but only 2–8% risk of valve dysfunction. Neither of these studies used colour Doppler as an adjunct for diagnosis, and therefore, quantification of valve regurgitation may be less reliable. The studies by Hull et al,13 Aleman et al,16 Schellong et al,19 Galper et al,21 Cutter et al23 and van Nimwegen et al,24 which reviewed clinical records to identify valve disease, found between 2.9% and 17% prevalence of valve dysfunction. These studies have the potential to underestimate the prevalence of valve dysfunction as patients with significant valve dysfunction who are asymptomatic may not be investigated. A further confounding factor is none of the studies included a baseline echocardiogram prior to radiotherapy and only two studies had a control group.
There were only two studies that specifically identified prevalence of valve disease in patients who received radiotherapy for breast cancer and found a 0.5–4.2% prevalence of valvular heart disease.17 ,20 These studies relied on the international classification of disease coding for valvular heart disease for the diagnosis. Therefore, it is not possible to identify the severity of valve disease examined. Furthermore, no control groups were studied. However, McGale et al20 studied the cardiovascular risk of radiation therapy by comparing incidence of cardiac complications between women with left-sided versus right-sided breast cancer. The rationale for this was the radiation dose to the heart in right-sided breast cancer would be considerably lower than in left-sided breast cancer and thereby serve as a control. The incidence of valvular heart disease in patients with left-sided breast cancer was increased compared with those with right-sided breast cancer (incidence rate ratio 1.54, 95% CI 1.11 to 2.13, p=0.009).
Risk factors
Radiation dose, interval from irradiation and the use of sequential chemotherapy are linked to development of radiation-induced valve disease. However, no study has examined the influence of these variables in patients with pre-existing valve abnormalities (bicuspid aortic valve).
Radiotherapy dose
Radiation dose is a key risk factor for development of valvular heart disease after treatment for Hodgkin's lymphoma. In a study of 1852 patients (83% of patients received mediastinal radiotherapy), there was a stepwise increase in risk of developing valve disease as radiation dose increased.23 For doses to the affected valve of 30 Gy, 31–35 Gy, 36–40 Gy and 40 Gy, the risk of valvular heart disease increased by factors of 1.4, 3.1, 5.4 and 11.8, respectively.
Interval from irradiation
The lack of prospective studies with regular interval screening means the natural history and radiation damage to heart valves is poorly understood. However, observational studies do demonstrate a long latent interval between radiation exposure and development of valve dysfunction. Although not linear, there is a progressive increase in development of valve dysfunction over time. Hull et al13 identified the actuarial incidence of moderate or severe valve dysfunction occurred in 1% at 10 years, 4% at 15 years and 6% at 20 years post radiation.
Chemotherapy
There is conflicting data on the effect of sequential chemotherapy prior to radiation therapy. Aleman et al16 found anthracycline-containing chemotherapy increased the risk of valve disease in patients receiving mediastinal radiotherapy by twofold, whereas patients receiving non-anthracycline-based chemotherapy had no increased risk. Furthermore, van Nimwegen et al24 identified that the dose of anthracycline received had a major impact on the risk of valvular heart disease. Anthracycline doses of between 35 and 200 mg/m2 had no impact on risk of heart valve disease (HR 1.1, CI 0.6 to 2) while those receiving 200–325 mg/m2 and 350–880 mg/m2 increased risk by 1.5 (CI 1.1 to 2.2) and 3.3 (CI 1.5 to 7.1), respectively. In contrast, Cutter et al23 found no association between anthracycline chemotherapy and the prevalence of valve disease. However, the investigators did not report the dose of anthracycline received by patients and it is possible the ratio of patients on low to high doses may have influenced the results.
Predictive models of radiation valve disease
Several studies in patients with Hodgkin's lymphoma have investigated dose–response relationships between dose to cardiac substructures and incidence of valvular heart disease. Cella et al25 showed that if >63% of the left atrium received 25 Gy or if >25% of the left ventricle received 30 Gy, this predicted development of aortic or mitral valve disease (ORs 5.7 and 4.4, respectively). Furthermore, they found that a maximum dose to the whole heart using a cut-off of 33 Gy predicted a high probability (OR 6.4) of heart valve damage. This suggests we may be able to predict future radiation-induced valve damage using dosimetric predictors at the time of radiotherapy. In a follow-up study, Cella et al26 demonstrated the risk of valve defects increased as the percentage volume of heart chambers (left atrium and ventricle) receiving 30 Gy increases (Spearman rank correlation coefficient 0.539, p<0.001).
Pathophysiology
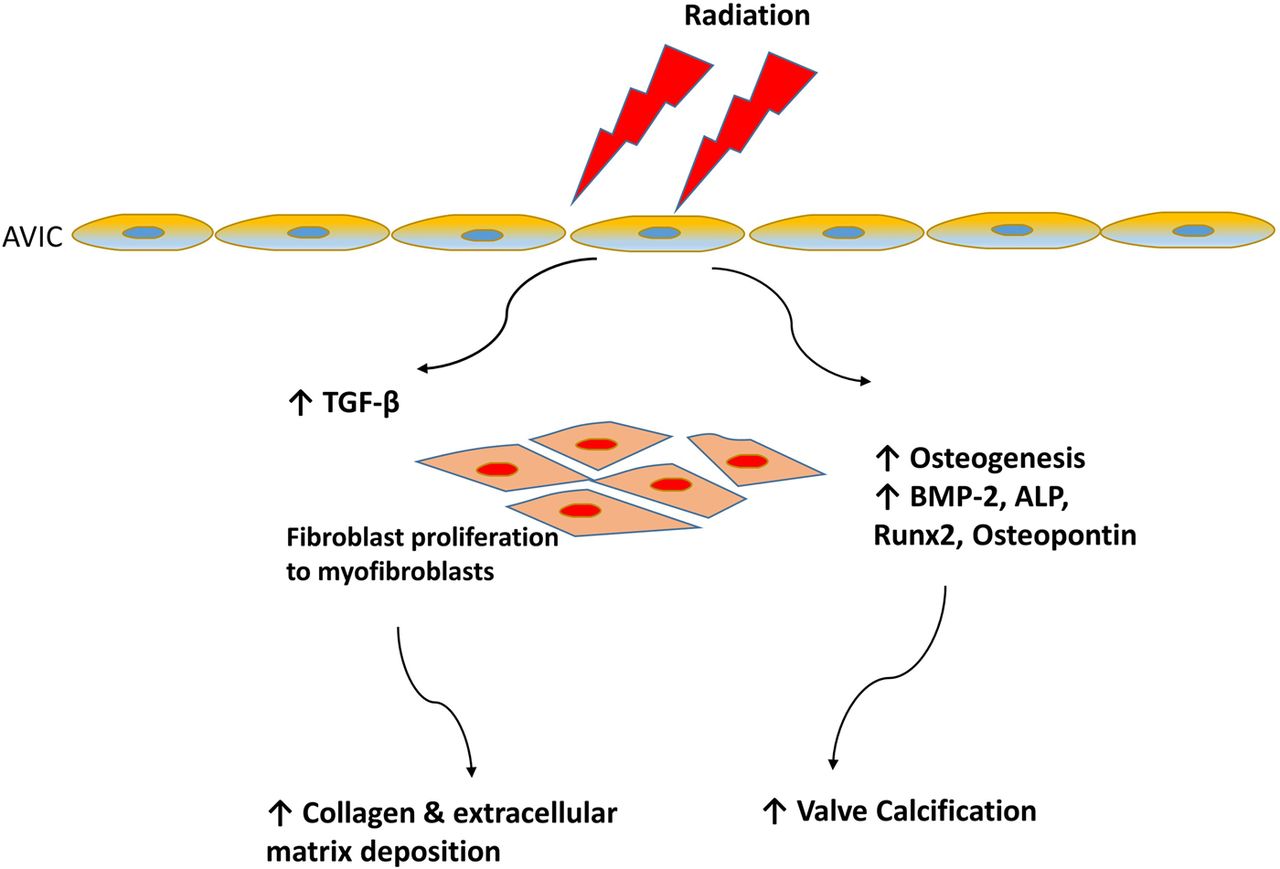
Autopsy studies have shown the valves of patients exposed to mediastinal radiotherapy exhibit diffuse or focal leaflet fibrosis/thickening together with calcification. No inflammatory changes or neovascularisation changes have been identified.27 ,28 The mechanism of radiation-induced damage to heart valves is not clearly understood with sparse data. However, radiation is known to activate fibrogenic growth factors including tissue growth factor β1, myofibroblasts and stimulate collagen synthesis in other tissues within the body.29 The role of radiation in valve calcification has recently been examined. Nadlonek et al30 demonstrated that irradiation of aortic interstitial cells induced an osteogenic phenotype. This resulted in increased formation of osteogenic factors including bone morphogenetic protein 2, osteopontin, alkaline phosphatase and the transcription factor Runx2. These are critical factors for bone formation and may explain why calcification of valves exposed to radiation is commonly seen (figure 1).

Pathophysiology of radiation-induced valve disease. Radiation exposure of aortic valve interstitial cells (AVICs) causes upregulation of fibrogenic growth factors including tissue growth factor (TGF) β1 leading to fibroblast proliferation and increased collagen synthesis. Radiation exposure also induces osteogenesis through increased formation of osteogenic factors including bone morphogenetic protein (BMP) 2, osteopontin, alkaline phosphatase (ALP) and the transcription factor Runx2 causing valve calcification.
Diagnostic techniques
The cornerstone of diagnosis involves identifying anatomical valve abnormalities, valve dysfunction and assessing the functional consequences of valve dysfunction on the ventricle. Echocardiography remains the optimal imaging technique for these. Cardiac MRI can provide complementary information where echocardiographic data are incomplete and can provide assessment of myocardial fibrosis. CT may be used to identify other sequelae of radiation heart disease such as coronary artery disease and pericardial thickening/calcification.31
Echocardiography
The early echocardiographic findings are characteristic but non-specific. Diffuse thickening of valve leaflets and subvalvar apparatus may occur without functional abnormality.32 Focal calcification of the valve leaflet/cusps typically involves the mitral-aortic curtain (anterior leaflet of the mitral valve extending to aortic root) (figure 2).33 ,34 Heidenreich et al14 demonstrated the presence of aortic-mitral calcification becomes more common as the time interval from radiotherapy increases. In their study, calcification of aortic, mitral or intervalvular fibrosa was present in 39% of patients examined within 5 years of radiotherapy compared with 90% of those examined >20 years after radiotherapy. The combination and variable degree of thickening and calcification leads to restricted motion and either valve stenosis or regurgitation. Importantly, unlike rheumatic valve disease, there is a lack of commissural fusion (figure 3).35

Echocardiogram from a patient who received mediastinal radiotherapy 24 years ago. Grossly thickened and calcified anterior mitral valve leaflet (white arrow). The calcification extends to non-coronary aortic valve cusp and sinus of Valsalva (red arrow). Ao, aorta; LV, left ventricle.

Three-dimensional transoesophageal echocardiogram demonstrating the difference between rheumatic valve disease and radiation-induced valve disease. (A) Rheumatic mitral valve with bilateral commissural fusion (black arrows). (B) In contrast in radiation-induced valve disease, there is no commissural fusion (red arrows).
Left-sided heart valves are more commonly affected, particularly the aortic valve. Pulmonary involvement is rare. In patients >20 years post irradiation, Heidenreich et al14 found moderate or severe aortic, mitral, tricuspid and pulmonary regurgitation in 15%, 4.1%, 4.1% and 0% of patients, respectively. Aortic stenosis was present in 16% of patients who were irradiated >20 years previously compared with <0.5% of age-matched and sex-matched controls.
Valvular dysfunction is progressive over time and may ultimately progress to severe dysfunction, requiring consideration of intervention. Wethal et al18 demonstrated 37% of patients with no significant regurgitation 10 years after radiotherapy developed moderate regurgitation after a further 12–14 years. Furthermore, 39% of their cohort with no aortic stenosis 10 years after radiotherapy developed varying degrees of aortic stenosis after a further 12–14 years. Cutter et al23 also noted the severity of valve dysfunction increased over time in 56% of their cohort with valvular heart disease.
Left ventricular myocardial systolic impairment is relatively common in patients exposed to mediastinal radiotherapy. Heidenreich et al14 found 36% of patients had evidence of left ventricular systolic impairment (fractional shortening <30%) compared with 3% of age-matched and sex-matched controls (p<0.01). Furthermore, the presence of regional wall motion abnormalities was independently related to radiation dose, age and time following irradiation. The use of deformation imaging (strain) can detect reduction in myocardial function after radiotherapy in patients with a normal left ventricular ejection fraction. However, data showing the clinical value or prognostic significance in this patient group are lacking.31 Radiation-induced pericardial involvement typically manifests as pericardial thickening14 or, more rarely, constrictive pericarditis characterised by thickened pericardium in combination with a restrictive filling pattern, significant respiratory variation in mitral inflow velocities and interventricular septal ‘bounce’.31
Management
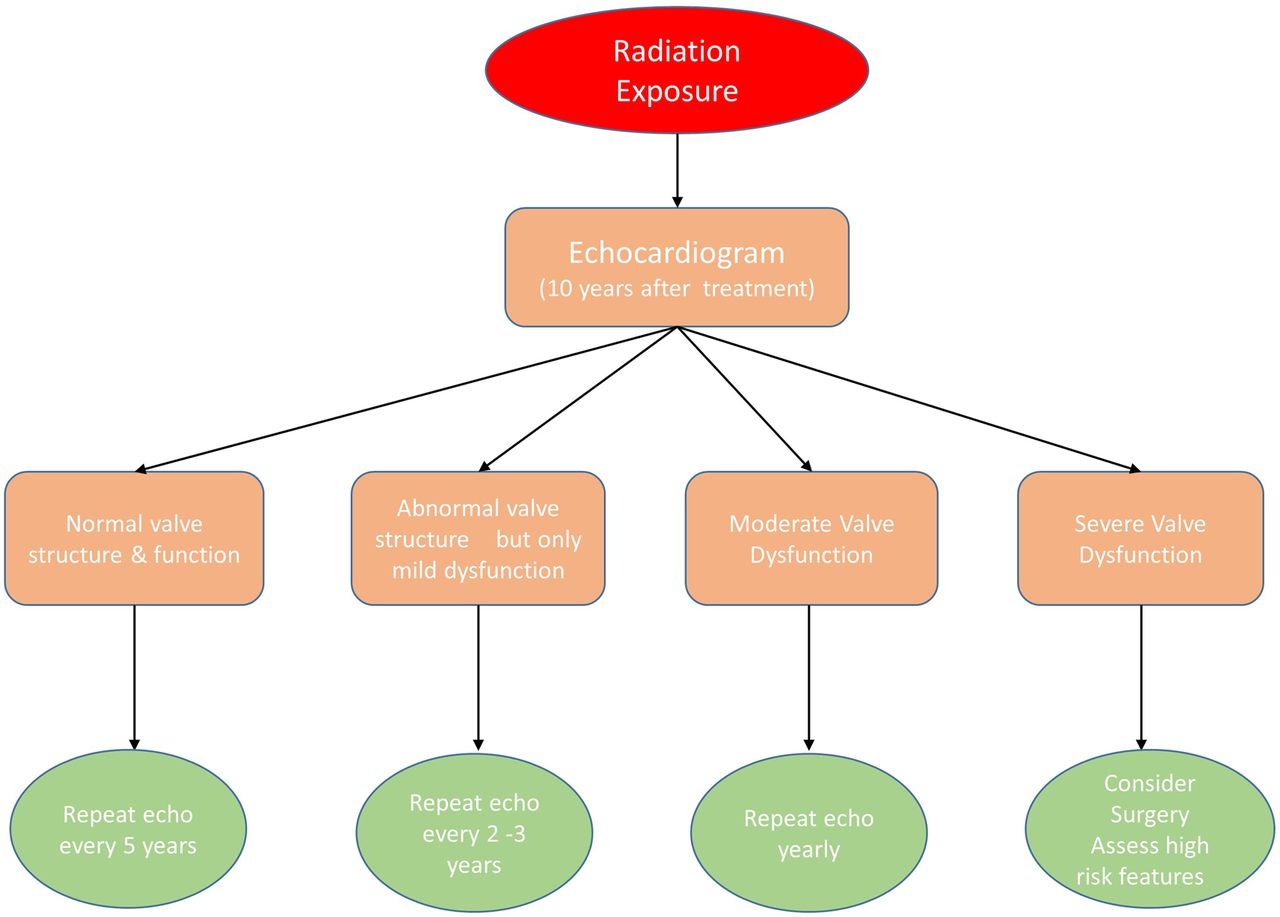
On long-term follow-up, a proportion of patients with radiation-induced valve disease will require intervention. Galper et al21 followed 1279 patients who were previously treated for Hodgkin's lymphoma. Seventy-eight (6.1%) patients developed moderate or severe disease at a median of 16.1 years after radiotherapy. Of these, 27 (34.6%) required valve surgery. The standardised incidence ratio for valve surgery compared with age-matched and sex-matched normal population was 9.2 (95% CI 8.1 to 10.3). A proposed algorithm for follow-up of patients exposed to mediastinal radiotherapy is presented in figure 4. There are no specific guidelines for the timing of surgery in patients with radiation-induced valve disease, and therefore, this should be performed according to current international guidelines.

Proposed algorithm for follow-up of patients exposed to mediastinal radiotherapy. All patients should be screened for heart valve disease 10 years after mediastinal radiotherapy. Those patients with normal valves require further 5-yearly follow-up. In patients with structurally abnormal valves (*calcification, thickening) but minimal valve dysfunction, closer follow-up is required (2–3 yearly). Patients with moderate valve disease require yearly follow-up. Patients with severe valve dysfunction should be assessed for valve surgery taking into consideration high-risk features (#pericardial constriction, left ventricular impairment and pulmonary fibrosis).
Risk stratification prior to cardiac valve surgery
Traditional risk stratification models used for assessment of perioperative risk in patients undergoing cardiac surgery do not account for specific complications related to radiation therapy. Patients with prior mediastinal radiotherapy undergoing valve surgery often have multiple comorbidities related to the effects of radiation on mediastinal structures. Handa et al36 identified radiation-induced cardiopulmonary comorbidities were common in a cohort of 60 patients with previous mediastinal radiotherapy undergoing cardiac valve surgery. Coronary artery disease, pulmonary fibrosis, constrictive pericarditis and conduction disturbances were found in 60%, 57%, 22% and 10% of patients, respectively. Perioperative mortality in this cohort was 12%. The main predictors of mortality in this period were a history of constrictive pericarditis, reduced preoperative ejection fraction and longer cardiopulmonary bypass times. Furthermore, there was a high prevalence of perioperative respiratory failure causing prolonged ventilator support (18%) and requirement for permanent pacemaker implantation (10%).
Chang et al37 identified the effect of the extent of mediastinal radiotherapy on the outcomes of 230 patients with previous mediastinal radiotherapy undergoing cardiac surgery. Patients were divided into subgroups depending on presumed extent of radiotherapy to mediastinum. Patients with extensive mediastinal radiotherapy had a higher in-hospital mortality than patients who received less mediastinal radiotherapy exposure (15.6% vs 2.4%) and were 3.5 times more likely to suffer respiratory failure. These two studies highlight the need for comprehensive assessment of cardiac and pulmonary comorbidities (in particular, constrictive myocardial physiology and pulmonary fibrosis/restrictive lung function) prior to cardiac valve surgery for optimal risk stratification.
Calcification of the aorta identified by CT has been reported in nearly 60% of patients with radiation-induced cardiac disease.38 Manipulation of the aorta during cardiac surgery in patients with extensive, circumferential calcification of the aorta (porcelain aorta) is associated with a high risk of cerebral embolism, and therefore, modification of the surgical approach or consideration of alternative percutaneous approaches is advised.38 Cardiac surgery in patients with mediastinal fibrosis/adhesions is challenging and associated with increased risk of damage to mediastinal structures. CT has been shown to be useful to identify adherence of vital structures such as the right ventricle to the chest wall/sternum.39 Other small series have shown a reasonable agreement for detection of adhesions between CT and surgical findings.40 However, the absence of adhesions on CT imaging does not reliably exclude mediastinum fibrosis.
Surgical or percutaneous valve replacement
The optimal choice of valve surgery in patients with radiation-induced valvular heart disease is poorly described. Crestanello et al41 examined the outcomes of 22 patients who had been treated with prior mediastinal radiotherapy and subsequently underwent mitral and/or tricuspid repair. Overall 5-year survival was no different from a cohort of patients exposed to mediastinal radiotherapy who underwent valve replacement (66% vs 63%, p=0.79). There was no difference in freedom from reoperation or transplantation between these groups (88% vs 94%, p=0.24) either. Although the data are limited due to small sample size, the benefits of valve repair over replacement are uncertain in this patient group.
Percutaneous valve techniques offer an alternative strategy for patients at high risk of cardiac surgery, including those with a ‘hostile’ thorax (mediastinal fibrosis, chest wall deformities) and porcelain aorta. Dijos et al42 found 10% of their cohort of patients referred for transcatheter aortic valve replacement had a history of mediastinal radiation exposure. These patients were younger (68 vs 83 years, p<0.05), exhibited a lower EuroSCORE (7% vs 22%, p<0.05) and had a higher frequency of hostile thorax (53% vs 29%, p<0.05) and porcelain aorta (63% vs 11%, p<0.05) compared with patients without radiation-induced heart valve disease. Patients with radiation-induced heart valve disease had a high procedure success rate (94%) with no mortality at 6 months post procedure. Transcatheter mitral valve repair (MitraClip) has been shown to be feasible in previously irradiated patients at high surgical risk with ≥ grade 3 mitral regurgitation and suitable mitral valve anatomy.43
Long-term outcomes
Patients with radiation heart disease who undergo cardiac surgery have greater long-term mortality than expected. Wu et al44 found survival of patients with radiation heart disease undergoing cardiothoracic surgery was 45% at a mean follow-up of 7.6 years compared with 72% in an age-matched and sex-matched group of patients undergoing similar surgery. Furthermore, the cause of death in the patients with radiation heart disease was due to cardiopulmonary disease in 49%. Interestingly, the same group of investigators identified aorto-mitral curtain thickness as the strongest predictor of long-term survival post surgery.45 In a study of 173 patients with prior mediastinal radiation who underwent cardiothoracic surgery (mean follow-up of 7.3 years), aorto-mitral curtain thickness was the strongest predictor of mortality (HR 5.75, 95% CI 1.57 to 21.03) while EuroSCORE (surgical risk stratification score) was only a modest predictor of mortality (HR 1.11, 95% CI 1.02 to 1.21).39 The reason for the high predictive value of aorto-mitral curtain thickness is not clear, but it may be a surrogate of the effect of radiation on the heart.
Techniques to reduce radiation dose
Radiotherapy techniques have evolved over the past few decades. Techniques to reduce radiation dose to normal tissues and/or the radiotherapy field size have emerged (figure 5). In patients with early-stage Hodgkin's lymphoma, reducing field size from extended field to involved field, and now involved nodal radiation therapy, does not result in any increase in local recurrence.46 Furthermore, Maraldo et al47 demonstrated significantly lower heart valve radiation doses in patients treated with small field involved node radiotherapy compared with large field mantle radiotherapy with an estimated 25-year absolute risk of any valve involvement of 0.8% (0–4.8%) vs 16.4% (4.7–49.85), respectively (p<0.000).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effect of reducing radiotherapy field size on cardiac structures. (A) Axial CT slice of mediastinal lymphoma (disease delineated in magenta) demonstrating extent of involved field radiotherapy (white arrow). Extent of radiation field depicted by red colour wash. (B) Coronal CT slice of involved field radiotherapy. Radiation field covers aorta (AO) and aortic valve (white arrow). (C) Involved node radiotherapy on the same patient reduces the size of radiation field (white arrow) to cover a margin around disease (red contour). (D) By reducing field size, the aorta and aortic valve are outside the field edge and receive considerably lower doses of radiation.
New techniques, including intensity modulated radiotherapy (IMRT) and proton therapy (PT), are better able to spare normal tissue by improving conformality to target structures. Radiation fields are shaped to target structures rather using than rectangular-shaped fields. Hoppe et al48 investigated radiation doses to heart valves with three-dimensional conformal radiotherapy (3DCRT), IMRT and PT. Compared with 3DCRT, IMRT and PT reduced the mean dose to both left and right ventricles, atria and aortic, mitral and tricuspid valves. This was confirmed by Maraldo et al.49 The same group of investigators also showed that the use of deep inspiration breath-hold rather than free breathing during radiotherapy treatment is associated with a reduction in heart dose for both IMRT and 3DCRT.50 The optimal field size and technique and respiratory gating will depend on the individual patient characteristics, including tumour size, location and nodal involvement and the use of individualised therapy to minimise normal tissue toxicity and long-term complications.
Conclusion
Radiation exposure is a risk factor for development of clinically significant valvular heart disease. Cancer survivors who received mediastinal radiotherapy require vigilance and screening for valvular heart disease many years after curative treatment. The predominant pathology is valve fibrosis and calcification. The risk is related to radiotherapy dose and progressively increases over time following exposure. Although the majority of patients are initially asymptomatic, a proportion of patients will require valve surgery. Long-term outcomes and risk of valve surgery are related to mediastinal complications of radiation including pericardial constriction, left ventricular impairment and pulmonary fibrosis. Modern radiotherapy techniques can be adapted to reduce dose to the heart and dosimetry models have been developed to predict future risk of radiation-induced valvular heart disease.
References
Footnotes
Contributors DMG and SB performed literature search and reviewed articles for inclusion. DMG, SB and GL drafted and revised manuscript and approved final version.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.