Article Text

Statistics from Altmetric.com
We report a 77 year old woman with a 14 year history of lymphoplasmacytic lymphoma initially involving the parotid gland, cervical lymph node, and hilar lymph node. She was treated with chlorambucil but the disease ran a protracted course with eventual multiorgan dissemination and required repeated chemotherapy. This time, she presented with bilateral hard, non-tender breast lumps for three months. The clinical diagnosis was lymphoma infiltration versus breast carcinoma. Mammographic examination showed a 2 cm, medium density, well circumscribed mass in the left breast and a 0.5 cm nodule of similar characteristics with macrocalcifications in the right breast.
Biopsy from the right breast mass showed amyloid deposits with foreign body giant cell reaction. The amyloid was Congo red positive with apple green dichroism under polarised light (fig 1), which persisted after 5% potassium permanganate pretreatment. It also stained positively for amyloid P and negative for AA protein immunohistochemically, confirming AL type amyloid. Ultrastructural examination showed the characteristic non-branching fibrils of indefinite length.
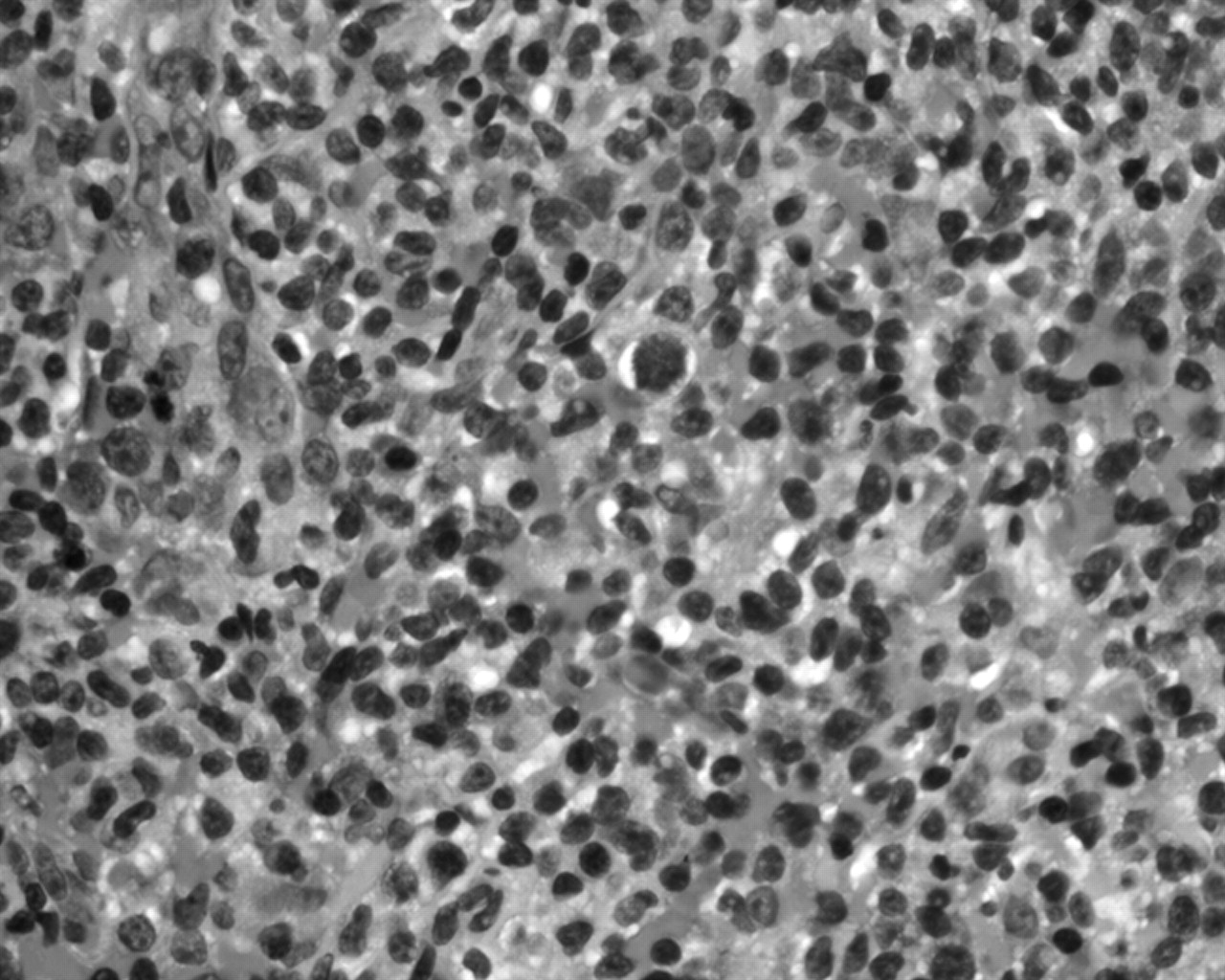
Image guided fine needle aspiration of the left breast mass showed atypical lymphoid cells that had enlarged nuclei and multiple small nucleoli, with mature lymphocytes and histiocytes in the background. Biopsy confirmed lymphoma, with the cells being immunoreactive for CD20 with κ light chain restriction, but not for CD3, CD5, CD10, or CD15, compatible with a diffuse large B cell lymphoma. No lymphoplasmacytic features were identified (fig 2). A small amount of amyloid was seen in the background.
Amyloidosis of the breast was first described in 1973,1 mostly involving elderly women. The amyloid deposits can either be isolated (amyloid tumour) or associated with plasma cell dyscrasia, connective tissue diseases, carcinoma of the breast, or non-Hodgkin lymphoma.2–7 Most patients are asymptomatic, although some may present with breast masses, breast tenderness, or peau d’orange. The role of fine needle aspiration cytology in breast amyloidosis is limited because most cases have been diagnosed retrospectively.4 Although our patient had a long history (14 years) of lymphoplasmacytic lymphoma, the short duration (three months) of the breast masses suggested that the amyloidosis was of recent onset. The absence of serum paraproteins and Bence Jones protein, together with the histological features of the breast lymphoma, indicated progression to a diffuse large cell lymphoma and not a recurrence of the lymphoplasmacytic lymphoma. The mechanism of lymphoma associated amyloidosis has generally been attributed to Waldenstrom’s macroglobulinaemia. Our case is unusual because the recent amyloidosis of the breast was not associated with serum paraproteins and the histological picture was compatible with diffuse large cell lymphoma. Because the amyloid in our case is of AL type, low amounts of immunoglobulin, which did not result in serum paraproteinaemia or Bence Jones proteins, may play an important aetiological role. Amyloid has to be considered in the differential diagnosis of breast lumps, particularly in patients with a history of malignant lymphoma. Although the conventional understanding of amyloid formation is related to raised serum paraproteins, as in Waldenstrom’s macroglobulinaemia associated with lymphoma, this may not be an absolute prerequisite for tumorous amyloid formation.

Photomicrograph of the right breast mass showing (A) amyloid deposits with foreign body reaction (haematoxylin and eosin stain; original magnification, ×100) and (B) orange coloured amyloid deposits (Congo red stain; original magnification, ×100).

{kind=link}
{kind=link}
Photomicrograph of the left breast mass showing a diffuse large cell lymphoma (haematoxylin and eosin stain; original magnification, ×400).