
Abstract
Hepatitis B is a serious liver disease that may require liver transplantation. Recurrence of the initial infection in the grafted liver occurs frequently, and this is a frequent case of death after transplantation. Treatment of recurrent infection with interferon has been ineffective, and the only therapy that has been shown to prevent infection is high dose hepatitis B immune globulin (HBIg), a material that is very expensive and in short supply. In this article the author reviews the experience with lamivudine, an orally available nucleoside analogue, as a means of preventing and treating recurrent hepatitis B after liver transplantation. The results in both areas look promising, and it is possible that lamivudine maintenance therapy may obviate the need for life-long use of HBIg after liver transplantation. This will undergo study over the next several years in a multicenter trial supported by the National Institutes of Health.
Introduction
Each year in the United States, 5,000 persons die from complications associated with hepatitis B virus (HBV) infection. Liver transplantation has been life saving in patients with acute fulminant hepatitis and chronic liver failure secondary to hepatitis B. Unfortunately, patients who undergo liver transplantation for hepatitis B, particularly those with decompensated cirrhosis, frequently acquire recurrent infection in the liver graft (1, 2). Reinfection may lead to rapid disease progression and has been reported to be a frequent cause of death within the first year after transplantation (2, 3). Therapy of recurrent infection with interferon, the only licensed drug to treat hepatitis B, has been ineffective. Because of the high rate of recurrent infection and impaired survival following liver transplantation for hepatitis B, the United States Health Care Financing Administration does not include this disorder as a reimbursable indication for liver transplantation (4).
Attempts to prevent reinfection have until recently depended upon the use of hepatitis B immune globulin, a scarce and costly material. Alternative therapeutic strategies to effectively prevent as well as treat hepatitis B in liver transplant recipients are greatly needed. In this article, I discuss recent advances with an orally available drug, lamivudine. We have been fortunate at Ochsner Clinic to have been chosen as the coordinating site for the study of lamivudine in 2 multicenter trials, one designed to prevent HBV infection and the other to treat recurrent hepatitis B after liver transplantation.
Recurrent Hepatitis B Following Liver Transplantation
After liver transplantation hepatitis B either results from de novo infection or, more commonly, as a result of an already established infection. Both situations are frequently associated with serious liver disease in the graft, and patients with recurrent disease have been reported to exhibit rapid graft failure between 3 to 6 months after transplantation (1). Indeed, the Pittsburgh group found that recurrent hepatitis B was the most common cause of death after the 60th postoperative day in a group of patients undergoing transplantation for chronic hepatitis B (2). Presently, not much can be done to improve the outlook of the patient with recurrent hepatitis B. Unfortunately, interferon has been shown to be relatively ineffective once infection is re-established in the graft (5, 6). In addition, this agent has the theoretical disadvantage of promoting graft rejection.
Theoretical and Practical Advantages of Nucleoside Analogue Therapy for Recurrent Hepatitis B After Liver Transplantation
Nucleoside Analogue Therapy
Nucleoside analogues represent the most promising form of treatment on the horizon for recurrent hepatitis B after liver transplantation. These agents work as HBV DNA chain terminators. As a class, nucleoside analogues have several theoretical and practical advantages (Table 1). Unlike interferon, nucleoside analogues do not have any known effects on cellular immunity and, therefore, do not pose any risk to the graft. Lamivudine, the most promising of the currently available agents, has been shown to have potent antiviral activity against HBV in vivo and in the hepadnavirus animal model (7, 8).
Lamivudine for Recurrent Hepatitis B
A multicenter study in the United States and Canada has recently been completed in which 52 patients with recurrent hepatitis B after liver transplantation were treated with lamivudine (9). Because hepatitis B after liver transplantation is a potentially life-threatening condition for which there is no proven therapy, the study was designed as a non-randomized, open label trial to assess longitudinal changes in serologic and histologic markers of disease activity and to determine the safety profile of lamivudine in this setting. Each patient who entered the trial had detectable HBV DNA in serum by solution hybridization or polymerase chain reaction and 45 (87%) had detectable serum hepatitis Be antigen. Thus, all patients were actively replicating virus. Patients were treated for 52 weeks with lamivudine (100 mg daily). The primary endpoint was the undetectability of HBV DNA; secondary endpoints included normalization of serum alanine aminotransferase levels, disappearance of hepatitis Be antigen, and improvement in liver histology.

Line graph of median hepatitis B virus DNA (HBV DNA •) and ALT (•) levels in 52 patients completing 52 weeks of treatment. The differences between baseline serum HBV DNA level and the week 24 and week 52 values were statistically significant for HBV DNA at p = 0.0001. The differences between baseline serum ALT and the week 24 and week 52 values were statistically significant (p = 0.0002 and p = 0.0012, respectively). All calculations are by Wilcoxon's signed ranked test.
After treatment, 60% had undetectable HBV DNA by solution hybridization; 14 (31%) of the initially positive patients lost hepatitis Be antigen; hepatitis B surface antigen was undetectable in 3 (7%); and serum alanine aminotransferase levels normalized in 29% (Figure 1, Table 2). Importantly, liver biopsies were done within 2 months of entry and again after 24 weeks of treatment to determine preliminary efficacy and safety. Paired liver samples were evaluated by Dr. Gist Farr of Ochsner Clinic, who was blinded to the clinical data, date of biopsy, patient identifiers, and the sequence in which the biopsies were obtained. The paired biopsies were ranked in appearance as improved, the same, or worse with respect to the degree of necroinflammation and fibrosis. Additionally, each biopsy was evaluated for the component features of the histologic activity index (HAI), as previously described by Knodell et al (10), and improvement was considered to have occurred if a 2 point or greater reduction in the score of the parameter under evaluation was observed after 6 months of treatment. The blinded histologic assessments revealed improvement in the histologic activity index (P = 0.007 for periportal necrosis, 0.001 for lobular inflammation, and 0.013 for portal inflammation) (Table 3).
Virological and Biochemical Parameters During 52 Weeks of Lamivudine Therapy
Liver Biopsy Response After 24 Weeks of Lamivudine
One of the limitations of nucleoside analogue therapy is the emergence of drug resistant variants. This has been shown in the case of lamivudine to be due to de novo mutation in the so-called YMDD region of the HBV DNA polymerase gene (11). Using a type of molecular technique called restriction fragment length polymorphism, drug resistant mutants were detected in 14 (27%) of patients during the 1-year treatment program. A question arose as to whether or not the mutant virus is as damaging to the host as the original or wild-type virus. Thus, repeat liver biopsies were obtained to address this question in 7 patients with the mutant virus. The biopsies were unchanged in 2 patients, improved in 2, and worse in 3 when compared with the baseline histologic assessment. Moreover, in a majority of the 14 cases in which the mutant virus appeared, the serum aminotransferase levels after detection of the mutant did not substantially differ from those observed immediately prior to emergence of the mutation, and values for both HBV DNA and alanine aminotransferase often remained lower than pretreatment values. While the long term natural history of the mutant virus is unknown, the data collected thus far are consistent with recent findings that the YMDD mutant is less replication-competent or fit and may be less apt to damage the grafted liver (12).
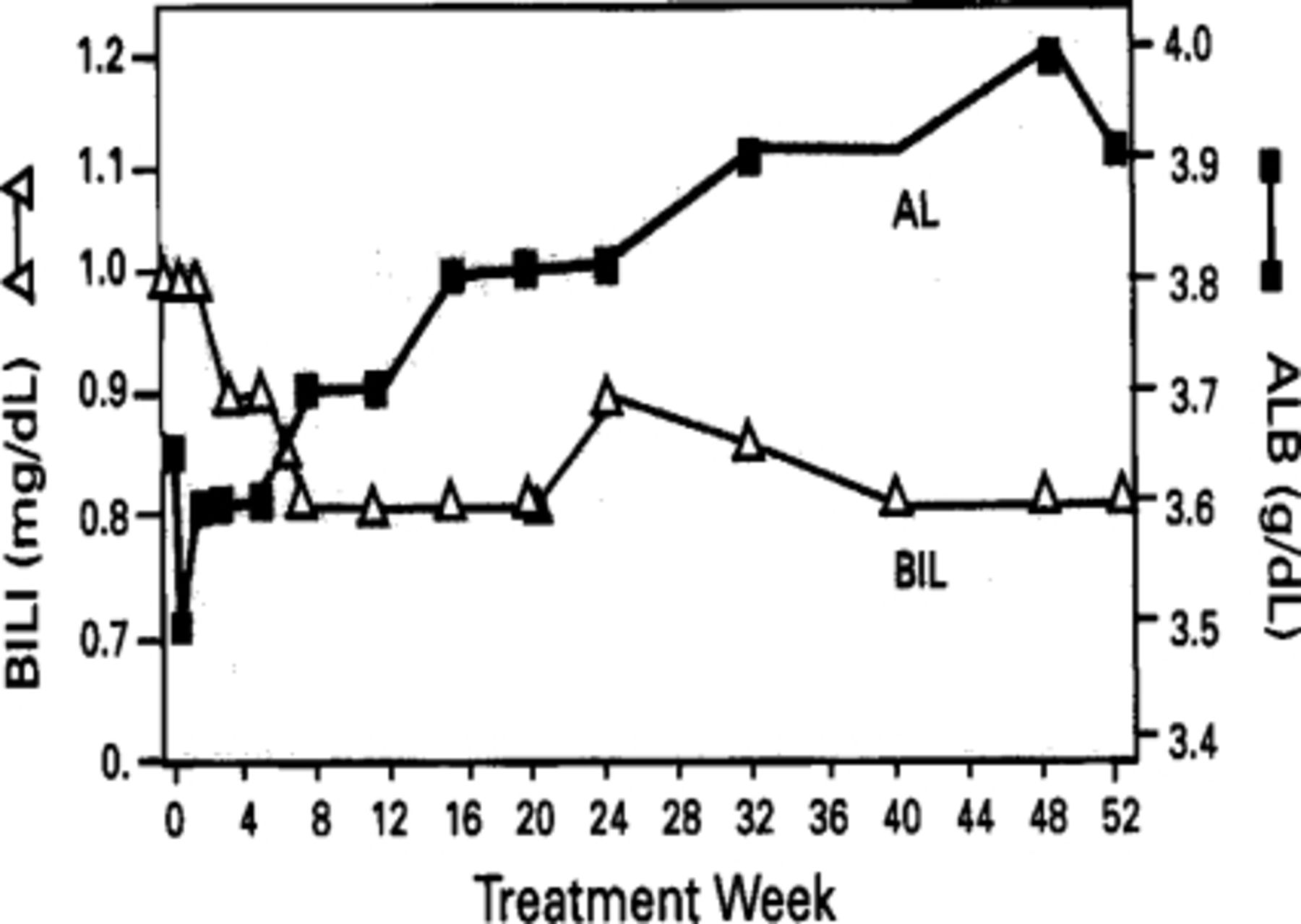
Line graph of median bilirubin (BILI $DL) and albumin (ALB •) levels in 52 patients completing 52 weeks of treatment. The difference between baseline serum albumin level and the week 24 value was not statistically significant but the difference was significant between baseline and the week 52 value (p = 0.0001). The difference between baseline serum bilirubin and the week 24 value had borderline statistical significance (p = 0.05) but the difference was significant between baseline and the week 52 value (p = 0.001). All calculations are by Wilcoxon's signed rank test.
Thus, we concluded from this study that lamivudine is a potentially effective therapy for hepatitis B after liver transplantation. Resistance to lamivudine occurs in some patients but is frequently not associated with clinical disease progression. Following the AIDS paradigm, it is possible that a lower rate of drug resistant mutants may occur if patients are initially treated with more than one nucleoside analogue. Alternatively, rescue therapy may be achievable with a second-generation nucleotide analogue, adefovir dipivoxil, which has been shown in vitro to be effective against the YMDD mutant. Studies are now beginning at Ochsner Clinic with this agent in nonimmunosuppressed patients with chronic hepatitis B.
Prevention of Hepatitis B After Liver Transplantation
It is clear that more can be gained from the prevention of hepatitis B after transplantation than in the treatment of recurrent disease. Unfortunately, this has been difficult to achieve until recently. The serious nature of hepatitis B after liver transplantation led European investigators in the early 1990's to propose the use of large amounts of Intravenous immunoglobulin containing high titers of neutralizing antibody (hepatitis B immune globulin or HBIg) (13). Typically, HBIg is administered intravenously at the time of transplantation and at periodic intervals thereafter to maintain a protective level of antibody (100 to 500 units). When used in this way, HBIg results in significantly lower rates of recurrent HBV infection and improves survival. However, there are several problems with this approach. HBIg has to be given intravenously to be maximally effective, and an intravenous preparation is currently not available in the United States. Moreover, it must be given indefinitely to be effective. Because HBIg is currently in short supply and is very expensive, with a yearly cost of $15,000 to $30,000 for the first year and $5,000 to $10,000 for each subsequent year, there are practical limitations to its use. Also, HBIg is not uniformly effective. The failure rate is 20% to 40%, and recurrent infection is most apt to occur in individuals who are actively replicating virus immediately prior to transplantation. It has been suggested that the effectiveness of HBIg therapy may be limited by the emergence of resistant mutants as is the case with lamivudine. In this situation, HBIg induces mutations in the S-gene which renders the virus non-neutralizable by antibody to the surface antigen (14). An alternative approach to prevention is greatly needed.
Starting in 1995, patients with end stage chronic hepatitis B were enrolled in a multicenter trial of lamivudine monotherapy to prevent hepatitis B after liver transplantation (15). In order to qualify for the study, patients had to be suitable candidates for liver transplantation. All were HBsAg positive and approximately 50% of patients were virus replicators when first ascertained. Lamivudine monotherapy was given to the patients as soon as they were listed for transplantation and continued for 1 year after transplantation. At the end of the 52-week treatment period, patients were asked to participate in a protocol for extended use of lamivudine if they had not reached predefinable endpoints (the loss of hepatitis B surface antigen and the development of detectable antibody to surface antigen).
At this time 37 patients have been transplanted. Nearly 70% of the patients who have completed at least 1 year of lamivudine therapy after transplantation have not been reinfected, as indicated by the absence of detectable hepatitis B surface antigen, The results are therefore quite comparable to those achieved with passive immunization therapy. Data relating to the duration and nature of this response are currently being analyzed.
Directions for the Future
There is reason to suspect that the combined use of HBIg and lamivudine will more effectively prevent recurrent infection than either approach alone. Recently, the National Institutes of Health has funded a multicenter grant to find the most effective way of preventing recurrent hepatitis B after liver transplantation. Ochsner Clinic is 1 of 5 centers represented on the steering committee of this important study, which will enroll 200 potentially transplantable patients with fulminant or chronic hepatitis B. Two treatment groups will be compared. Both groups will receive lamivudine and HBIg during the 6-month period after transplantation, at which point they will undergo randomization to either discontinuation of HBIg with continuation of lamivudine for a period of 3 years or continuation of both agents during a 3-year post-operative period. Whereas the primary aim of the study will be to compare the efficacy of these two approaches, a secondary aim will be to study their cost effectiveness. The results of this study are likely to determine future policies relating to transplantation for hepatitis B.
The last few years have witnessed the development of promising medical approaches to both the prevention and treatment of recurrent HBV infection after liver transplantation. The experience with lamivudine and other nucleoside analogues as well as the experience with aggressive passive immunization is sufficiently encouraging to warrant re-examination of current Health Care Financing Administration guidelines for reimbursement and to alter prevailing attitudes about the value of liver transplantation for patients with chronic hepatitis B.
- Academic Division of Ochsner Clinic Foundation
In this issue








{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.