
Abstract
Family practice physicians have contributed significantly to the care of maternity patients nationwide, but since the 1970s the number of family practice physicians delivering babies has decreased at a steady pace. In rural areas especially, family physicians are often the sole providers of care. Without these rural doctors providing maternal care, the risk of poor maternal/infant outcome increases. In the 1990s, it was found that residents of family medicine who are taught obstetrics all or in part by other family practice doctors are more likely to provide this kind of care when they finish residency. With this information, the Residency Review Committee that oversees national residency guidelines added the requirement that in all family practice residencies at least one practitioner must provide maternity care in an ongoing basis. To meet this challenge the country's medical training institutions quickly had to find new ways to teach and provide coverage for family practitioners involved in newborn delivery. Ochsner has developed credentialling for staff family practitioners to provide this care. Staff family practitioners are involved in the prenatal care of pregnant patients and have the opportunity to supervise their residents during labor and delivery. With the assistance of the obstetrical staff the Family Practice Residents' experience has greatly increased, reaching nearly 70 deliveries in 1998 alone with projections of over 100 for 1999.
The Scope of the Problem Nationwide
Nationally, the number of family physicians delivering babies has declined over the last 15 years from near 50% in the mid 1970s to 26% by 1993 (1). Although recent estimates also show that in the southeast United States, only 12% of family physicians performed obstetrics in 1991, and in Florida only 2% of all family practitioners delivered babies in 1989 (2,3), the number of family practitioners providing maternity care rose nationwide to 28% in 1998, according to an unpublished 1998 Practice Profile Survey by the American Academy of Family Practice (AAFP).
Family physicians attend a substantial number of deliveries in the US, “attending an estimated 500,000 of the 4 million births each year” (4). In rural areas family physicians often provide 100% of the maternity care (5). But if the number of family physicians delivering babies in the United States continues to fall, this will mean further hardship on the 1 in 4 Americans living in rural areas, where obstetricians number 1% of all doctors and Family Practice doctors perform a necessary role (2). There is also a clear relationship between infant mortality and the availability of maternity care, which would obviously be affected by this decreasing trend in maternity care providers (6).
The Advent of ALSO®: Meeting the Challenge
Out of concern for the declining number of family physicians providing maternity care, especially in rural and underserved areas, and because of the need to maintain emergency care skills among low-volume providers, Dr. James R. Damos of the University of Wisconsin originated the Advanced Life Support in Obstetrics (ALSO®) course in 1990 using the same techniques as other established life support courses such as Advanced Cardiac Life Support (ACLS) and Advanced Trauma Life Support (ATLS) (6). Damos and colleagues felt that maternity care was a key stage of the family life cycle, and it should remain an integral part of the practice of family physicians. The first ALSO® course was given in 1991 and currently includes a syllabus, slide set, lectures, hands-on work station, an objective written examination, and a “mega-delivery” testing station that tests the hands-on ability of participants to effectively deal with serious potential problems of delivery.
In 1993, the AAFP acquired ALSO®. There are now over 300 approved instructors and over 80 advisory faculty. Since it began, over 7,000 participants have taken an ALSO® Provider course in the US, Canada, and England.
National Residency Training Issues
Sakornbut et al. demonstrated that if Family Practice residents are trained in obstetrics all or in part by another family practitioner they are more likely to deliver babies when they finish their training (7). As a direct result of this study, the Residency Review Commission (RRC), which oversees national residency guidelines, mandated in 1997 that all Family Practice residencies have at least one Family Practice staff member delivering babies in the teaching setting (8). The effect was that approximately 25% of Family Practice residencies had to rapidly respond to this mandate in order to ensure compliance. Issues such as retraining, practicing in non-supportive if not hostile environments, cross-coverage, insurance coverage, and extent of privileges, to name a few, have emerged.
Ochsner's Standing with Regard to Training
In 1988, Ochsner Clinic established a Department of Family Medicine and in 1992 began a Family Medicine Residency Program. The entering class of 1992 was the first to deliver babies at Ochsner, and at the time were the only known non-obstetrician physicians to have delivered at Ochsner Foundation Hospital, as well as the only known non-obstetrician physicians at the time to be delivering babies in the city of New Orleans. Even though many of the family practitioners at Ochsner had very good experience performing deliveries, none were active in the process. With the graduating class of 1995, 2 of 4 graduates went on to continue providing maternal care and teaching it to other residents (1 remains at Ochsner as staff). Deliveries on required obstetrics (OB) rotations ranged widely from 30 to 80, but there was a paucity of longitudinal obstetrical patients (that is, patients seen by the resident for their prenatal care and delivery). The residents averaged somewhat less than 10 deliveries a year for 1994-1996 and 17 deliveries for 1997.
The Plan
In 1997, after receiving a mandate from the RRC to increase the obstetrical experience of our residents and to increase the number of staff involved in obstetrical cases, a plan was put forth to better accomplish these goals. A goal of at least 50 deliveries by each graduating resident was set, of which 10 or more should be longitudinal. For 20 residents in the program, that translates to 200 deliveries in 3 years (9). Also, a plan was put in place for the credentialling of family practice staff to obtain obstetric privileges at Ochsner Foundation Hospital.
How It Was Accomplished
The Family Practice Residency Program site was moved to an area that had more access to underserved and potential Medicare maternity patients in the eastern portion of the city. At the same time, Ochsner obtained permission from the St. Thomas Health Clinic to provide prenatal care to its predominantly Medicaid population. The St. Thomas Clinic is a designated community health center serving a primarily indigent African American population in the inner city. The St. Thomas clinic alone has been predicted to provide 200 new maternity patients a year, of which 120 are likely to be deliverable at Ochsner Foundation Hospital. Attrition from the program of services would be due to high-risk transfers, relocation, or patient choice. One maternal fetal specialist, Ochsner's Dr. Douglas Montgomery, oversees the efforts and assures quality of care. Ochsner Family Practice faculty also staff the prenatal clinic.
Some Results
As a result of the involvement of the Maternal Fetal Medicine Section, headed by Dr. Montgomery, clear guidelines and standards for prenatal care have been established. Dr. Montgomery has maintained clear lines of communication with residents and staff alike to facilitate a high standard of care. Staff and resident obstetricians/gynecologists (OB/Gyn) on call assist in coverage of maternal patients that are seen by family practitioners.

Total longitudinal deliveries for Ochsner Family Practice Residency
Three Family Practice staff obtained proctored privileges to deliver babies at Ochsner, and 1 of these has obtained unmonitored privileges for vaginal deliveries, a first in this institution's history. These 3 staff members have also attended the AAFP sponsored courses in Family Centered Maternity Care and the ALSO® course and provide guidance to the Family Practice residents when their patients present to labor and delivery, One staff member has become a certified course instructor and cosponsored the first ALSO® course in Louisiana in November of 1998 in conjunction with the Family Practice Residency at Baton Rouge General Hospital.
Recently, longitudinal obstetrical patient numbers have dramatically changed for the residents. Family Practice residents delivered 17 longitudinal obstetric patients at Ochsner Foundation Hospital in 1997. That number reached almost 60 in 1998 (with just over half from the St. Thomas Clinic) and is predicted to reach 100 by the end of 1999 (Figure 1). In 1999, 70% of our deliveries are expected to come from the St. Thomas Clinic. This projected growth rate will more than meet our goal of 200 deliveries by our residents over the next 3 years.
My Results
Because there had not previously been a family practitioner at Ochsner Clinic who delivered babies, there was no family practitioner to provide coverage for me in the event that I was out of town when my patients delivered. Also, because there was not a formal credentialling process in place, my own practice, by design, has begun slowly and been built gradually over 3 years (Figure 2). I delivered maternity patients as the residents did with very close OB/Gyn staffing. The residents are expected to deliver 10 babies longitudinally in 3 years. I delivered 30, with the majority of those being in 1998. I expect to have over 30 for 1999 alone, averaging 2 to 3 deliveries a month with 10 to 15 of those being from coverage of resident deliveries. My personal goal is not to become an obstetrician (as is obvious by the overall numbers), but to become a family practitioner that provides high quality family-centered maternity care. Credentialling is now in place for other family practitioners to obtain privileges.
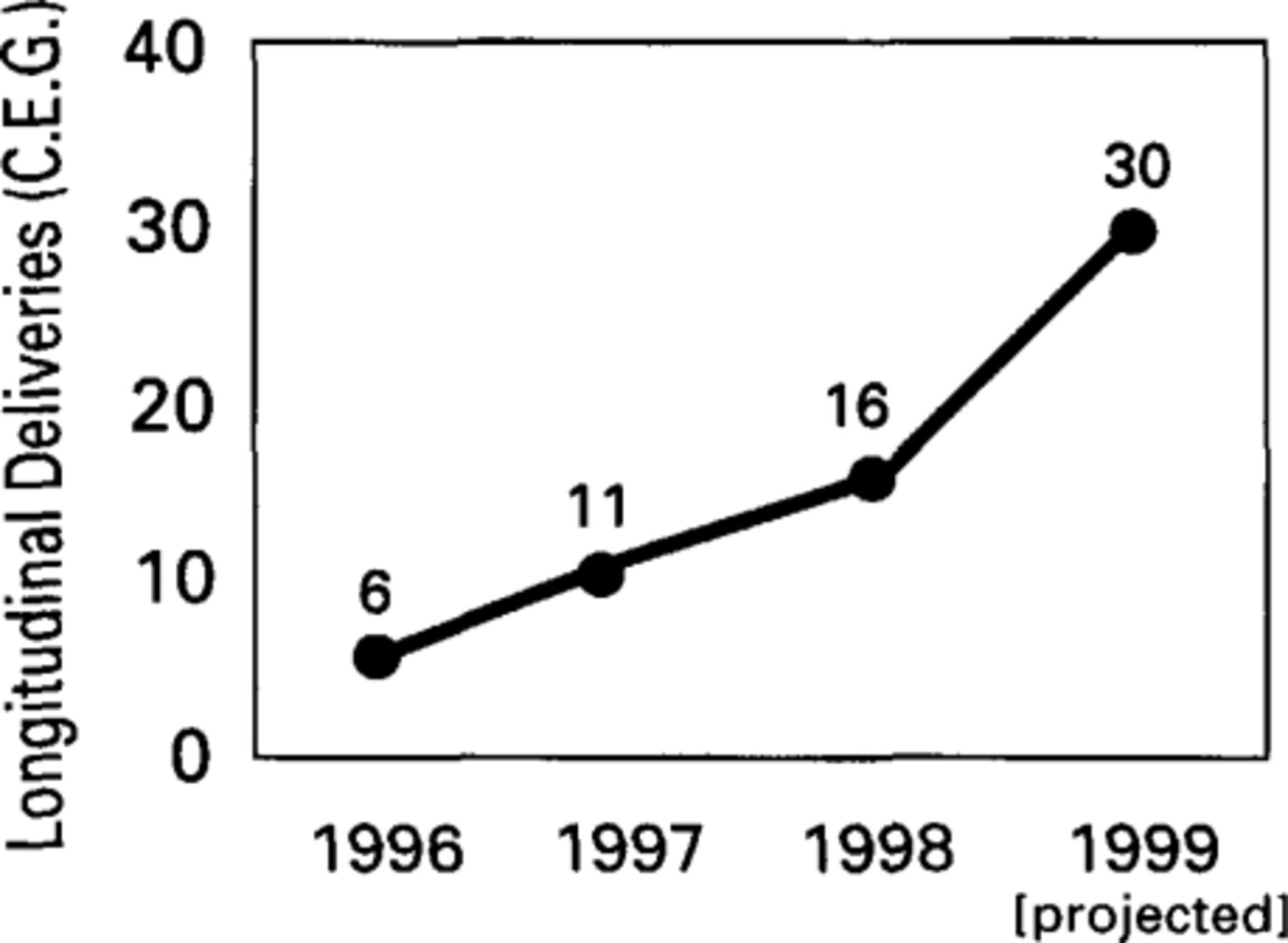
Longitudinal deliveries (C.E.G.)
Risk Assessment for Newborn Delivery (10)
Being involved in maternity care and the family care that follows has been a source of great satisfaction in my practice. It permits young growing families to see the same doctor. This has been shown to be part of the reason that family practitioners nationwide have continued to deliver babies (4).
Some Guidelines
The results of increased deliveries by Family Practice physicians at Ochsner might be viewed with skepticism by physicians in the OB/Gyn department without some clear guidelines for delivery by family practitioners and the setting in which this should take place. The ALSO® course provides some national guidelines, and joint efforts between the American College of Obstetricians and Gynecologists (ACOG) and the AAFP have established position papers on the subject. Locally, Ochsner's OB/Gyn department and Family Practice Residency Program have also provided guidelines for consultation.
As a rule of thumb, any condition likely to result in the delivery of a premature or low birth weight infant warrants delivery in a facility with specialized nursery and neonatologist. The local providers of care must establish clear lines of communication with their consultants and should develop protocols of action in the event a problem arises in the care of their patient. The family practitioner or obstetrician in a rural setting must be excellent in identifying patients at risk and be willing to refer them. The family practitioner in the tertiary care setting also must be constantly diligent in identifying risk factors in their patients and obtain appropriate consultation and treatment. Risk factor evaluation only identifies 50% of patients who will develop a problem sometime during their pregnancy. Table 1 (10) provides a partial list of problems that should encourage specialty consultation. Both pre-pregnancy and prenatal risk factors are listed. Factors such as age, race marital status, education level, smoking history, weight, and past obstetric history should also be included in risk assessment.
Conclusions
Family Practice physicians nationwide continue to provide high quality pregnancy care. Since 1970, the number of physicians delivering has been decreasing. However, with a nationally mandated increase in family physicians providing this care in the residency setting, the advent of joint cooperative declarations between ACOG and the AAFP (11), and the growth and development of the ALSO® course, the number of family physicians delivering babies has begun to increase. Improved access of rural patients to family practitioners who are properly trained in newborn delivery will help to decrease neonatal morbidity and mortality. Family Practice physicians who incorporate obstetrics into their practice can significantly impact this access. There continues to be a great need for providers in this setting who not only deliver babies but can also be continuously diligent in recognizing problems and risk factors while appropriately obtaining consultation to diminish risk and improve outcomes. There is also great need for providers of primary and tertiary maternity care to discuss problems early on and develop protocols for differing problems.
Ochsner Clinic has been very forward in the process. Because of recent involvement of Family Practice staff, obstetricians, and maternal-fetal specialists, graduates from Ochsner's Family Medicine Program will have improved experience and abilities, and because of Ochsner's support will be better able to provide family centered maternity care.
- Academic Division of Ochsner Clinic Foundation
In this issue








{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.