
Over 100 years ago, the predominant afflictions of patients visiting physicians' offices were acute illnesses led by infectious disease. Infectious disease was the leading cause of death at the turn of the century and because of its epidemic nature, the American medical community developed a standardized assessment to help clinicians confront this disorder. This assessment, known as vital signs, included temperature, pulse rate, respiratory rate, and later, blood pressure (1, 2). Over time, the measurement of vital signs became an expected part of every clinical visit and an essential component of the database physicians use to evaluate, diagnose, and treat patients.
Early in this century, Alton Ochsner made seminal observations regarding the relationship between cigarette smoking and lung cancer (Figure 1) (3). As we enter the next century, American medicine is challenged by the complexity of chronic illnesses, which now predominate as the leading causes of death and disability in Western civilization. Cigarettes are now responsible for more than 430,000 deaths each year in the United States, costing the United States approximately 50 billion dollars annually in medical care (4). Over the last 60 years since Dr. Ochsner's original observations, it has been proven that cigarette smoking is the cause of 90% of bronchogenic carcinoma and 30% of all cancer deaths each year in this country (5). Furthermore, nearly one in five deaths from cardiovascular disease is attributable to smoking, and an additional 40,000 non- smokers die each year from cardiovascular disease as a result of exposure to environmental tobacco smoke (4).

DOONESBURY © 1993 G. B. Trudeau. Reprinted with permission of UNIVERSAL PRESS SYNDICATE. All rights reserved.
Because of the epidemic nature that smoking now represents to us as a society, it is important that all physicians and health care providers focus on two key measures in order to reduce the morbidity and mortality associated with smoking as we enter the next century: 1) to assess and document smoking status in all patients under the care of the physician; 2) to learn and use a brief intervention message to help patients quit.
Assessment and Documentation of Smoking Status
At least 70% of smokers see a physician each year, and more than 50% see a dentist (6, 7). Moreover, 70% of smokers report that they want to quit and have made at least one self-described serious attempt to quit (8). Furthermore, smokers cite a physician's advice to quit as an important motivator for attempting to stop. Unfortunately, clinicians are not capitalizing fully on this unique opportunity. Only about half of current smokers report ever having been asked about their smoking status or urged to quit. Fewer still have received specific advice on how to quit smoking successfully.
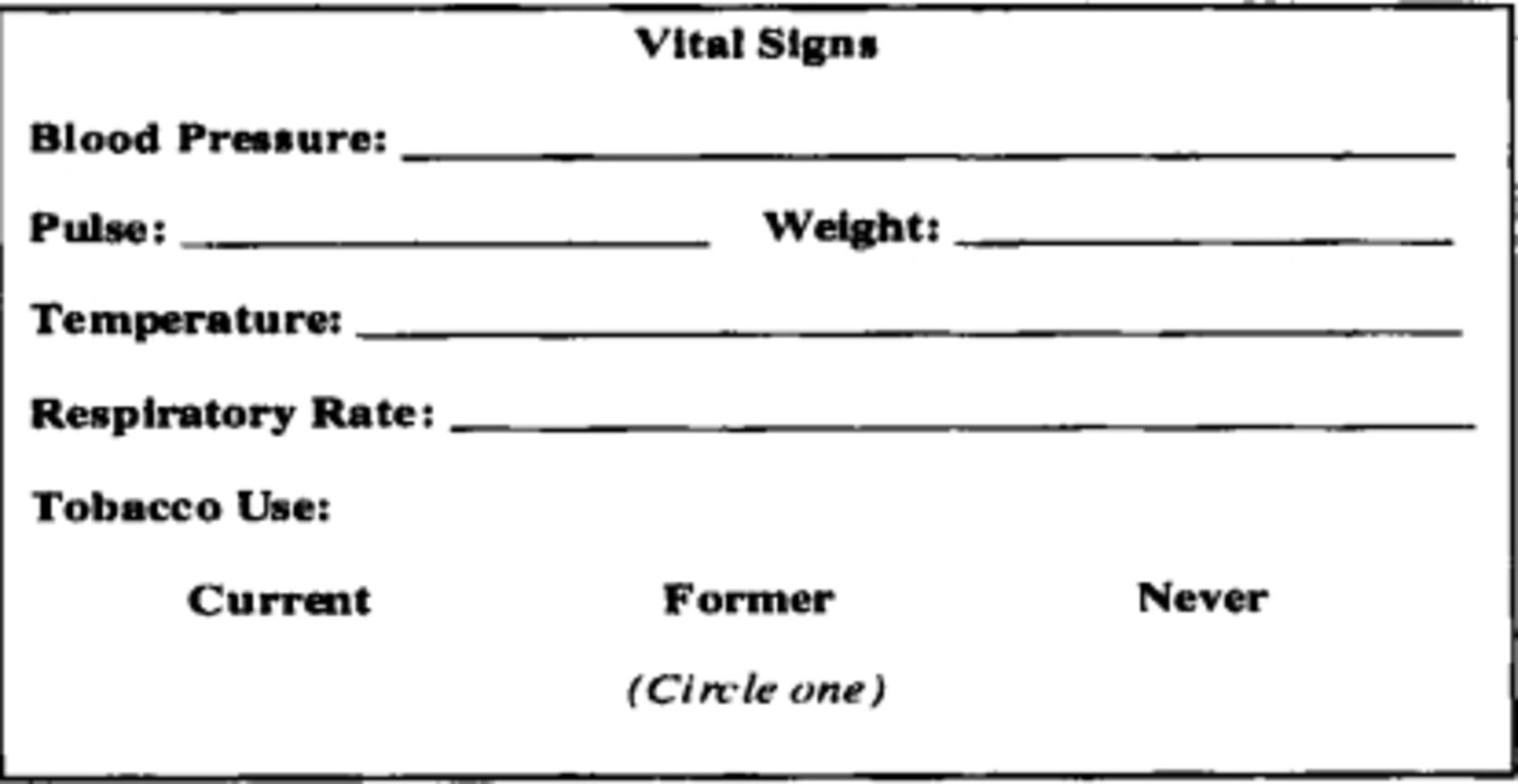
Because of the epidemic nature that smoking currently represents in the United States, the Agency for Health Care Policy and Research (AHCPR) has advocated making smoking status the “new vital sign” as a simple way of assessing and documenting smoking status for every patient during each clinical encounter (5,9). This small but fundamental change in clinical practice would address a current weakness in the way we practice medicine: the failure to universally assess, document, and intervene in patients who smoke (Figure 2).

A vital signs stamp or sticker that includes an indication of smoking status should be placed on patient's charts at each clinic visit. (Adapted with permission from: JAMA, 275:1270, 1996. © 1996 American Medical Association).
Most patients do not object to having their blood pressure measured during every clinic visit, and there are no data to suggest that they would object to the regular assessment of smoking status, particularly if presented in the context of routine preventive care (10, 11). Making smoking status a vital sign would also promote the guidelines of the United States Preventive Services Task Force (12) that “tobacco cessation counseling should be offered on a regular basis to all patients who smoke cigarettes,” and the National Health Promotion and Disease Prevention Objectives (13) for the year 2000 to “increase to at least 75% the proportion of primary care and oral health care providers who routinely advise cessation and provide assistance and follow-up for all their tobacco-using patients.”
Learn and Use a Brief Intervention Message to Help Patients Quit
Once aware of the smoking status of their patients, physicians can then focus on moving smokers from the stage of contemplating quitting to making an attempt to quit. As the National Cancer Institute's guidelines highlight, “It is essential to provide effective cessation intervention for all tobacco users at each clinical visit.” The AHCPR Consensus Statement includes a recommendation for actions and strategies for the primary care physician (Tables 1).
Nicotine Substitution
Nicotine substitution therapy has been the most promising pharmacological method studied to date. The rationale behind nicotine replacement has been to prevent or relieve nicotine withdrawal symptoms while stopping smoking behavior by replacing it with another behavior. Pharmacological nicotine comes in several forms, including nicotine polacrilex gum, nicotine nasal spray, and transdermal nicotine in the form of nicotine patches. The most widely used therapy is the nicotine patch that is now available over the counter in various formats. This form of nicotine substitution has been demonstrated to be two to three times more effective than placebo in maintaining smoking cessation at a six month follow-up (14-16). The 16-hour and 24-hour patches appear equally efficacious, and extending the treatment beyond eight weeks did not appear to increase efficacy in the majority of the patients (14). The clinical guidelines for prescribing nicotine replacement products are highlighted in Tables 2, and their use should be encouraged in patients attempting to quit smoking.
Cigarette Smoking is a Chronic Disease
As with hypertension, diabetes, chronic obstructive pulmonary disease, and congestive heart failure, cigarette smoking can be considered a chronic disease requiring on-going attention and treatment. Since smokers may be at various stages in the quitting process, physicians must continue to assist their smoking patients, often through repeated contacts over many months or years. Recent quitters are at particularly high risk for relapse for several months after quitting (4). As with other chronic diseases, the treatment of cigarette smoking must continue even in the face of very modest cure rates. A realistic smoking cessation rate of 5% to 10% can be expected from a brief clinical intervention and can be essentially doubled if this is combined with nicotine substitution (14). While most physicians would be elated by a 10% remission rate with unmedicated hypertensive patients, many patients become discouraged with smoking cessation interventions because of the high relapse rates. If clinicians universally achieve the 5% to 10% successful cessation rate each year among all of their patients who smoke, the impact would be enormous.
In summary, it is paramount that we identify all of our smokers in our respective practices and interact with them regarding their smoking behavior on each visit. Adding smoking status as a new vital sign will provide the institutional framework by which the epidemic of tobacco use can be universally confronted. With minimal intervention by the physician, and use of appropriate pharmacotherapy, we can expect to make significant reductions in this epidemic going into the new century.
Actions and strategies for the primary care clinician (Adapted with permission from: JAMA, 275:1270, 1996. ©1996 American Medical Association).
Clinical guidelines for prescribing nicotine replacement products (Adapted with permission from: JAMA, 275:1270, 1996. ©1996 American Medical Association).
- Academic Division of Ochsner Clinic Foundation








{kind=link}
{kind=link}