
Abstract
Endovascular treatment of abdominal aortic aneurysms (AAAs) is an exciting new minimally invasive treatment option for patients with this disease. Ochsner Clinic has been the only institution in the Gulf South participating in FDA clinical trials of these investigational devices. Early results with endovascular AAA repair demonstrate a trend towards lower mortality and morbidity when compared with traditional open surgery. Length of stay has been reduced by two-thirds with a marked reduction in postoperative pain and at-home convalescence. If the long-term data on efficacy and durability of these devices are good, most AAAs in the future will be treated with this minimally invasive technique.
Abdominal aortic aneurysms (AAAs) are fairly common, with a prevalence of 2% to 5% in men over 60 years of age; AAA rupture is the tenth leading cause of death in this patient population (1). Approximately 35,000-45,000 operations are performed annually to repair AAA in the United States (2). While the safety of AAA repair has improved significantly in the past 15 years, these procedures are still associated with considerable combined morbidity/mortality and postoperative pain. Patients undergoing open AAA repair have a mean hospital stay of 9 to 11 days (3) and a 3 to 6 week convalescence. There is clearly room for improvement.
Parodi performed the first endovascular repair of an AAA in 1991 (4). The last 5 years have witnessed an explosion of interest in this area by both physicians and the industry, which has produced a number of different endograft designs. Currently, there are no FDA approved endovascular grafts commercially available, but several endografts are in phase II and Phase III FDA trials. The first aortic endograft commercially available in the US will likely appear in the next 6 to 12 months.
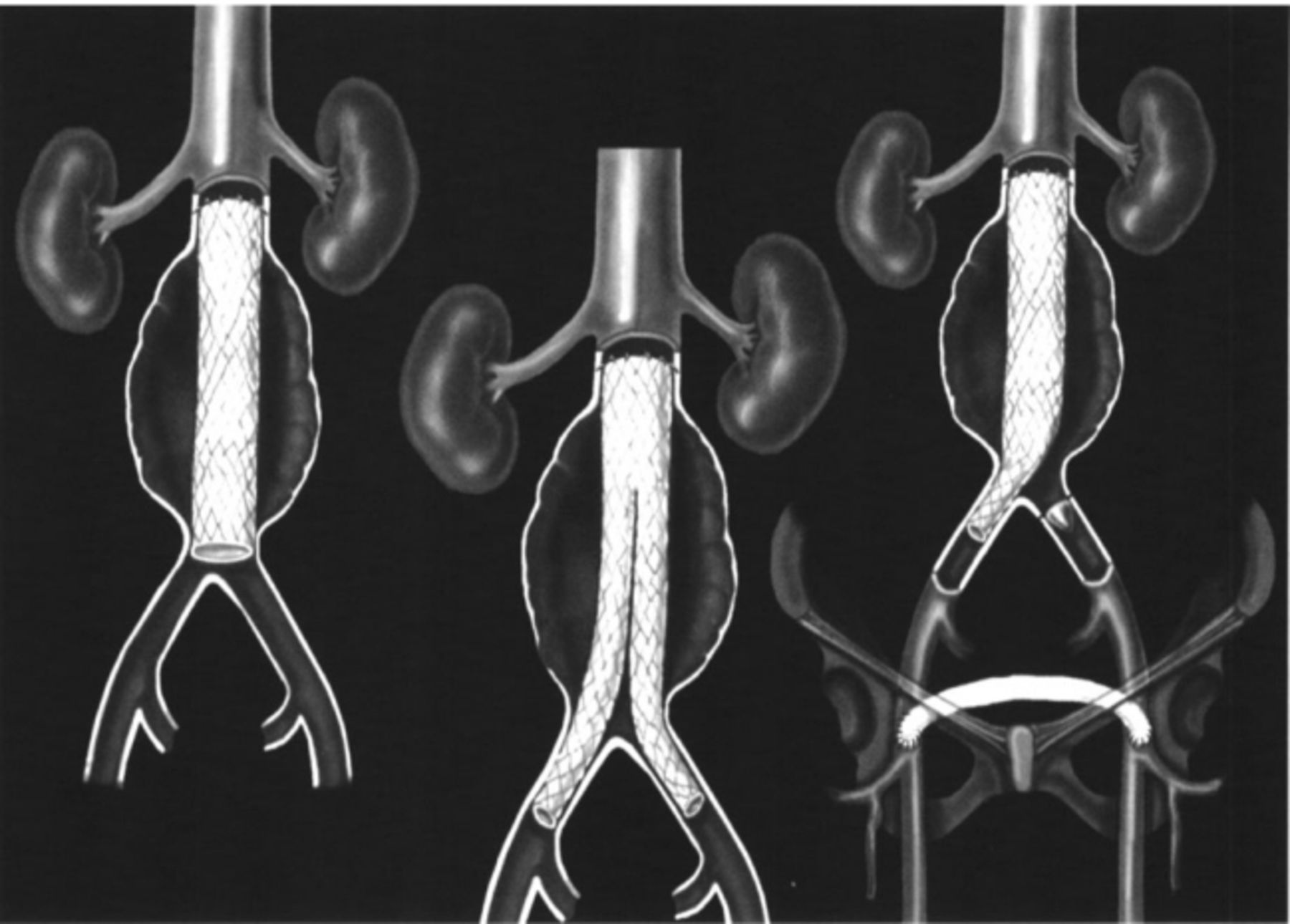
While there is great heterogeneity in the materials and design of these endografts (3,5-9), three basic endograft configurations have been developed (Figure 1): tube grafts, aorto-uni-iliac grafts used with a conventional femoral-femoral bypass, and aorto-bi-iliac (bifurcated) grafts, some delivered in one piece and others with a modular design. These devices are inserted retrograde into the AAA via the femoral artery. Because the delivery systems range from 18-27 Fr, a small “cut down” and formal femoral artery closure are required.
The first endografts developed were tube grafts (Figure 1A), with proximal and distal metal barbs and/or stents designed to anchor the otherwise unsupported graft in the proximal and distal non-aneurysmal segment of the AAA (7). Because few AAAs have non-aneurysmal segments before the iliac bifurcation, less than 10% of patients with AAAs were candidates for this graft. Large numbers of early and late failures were seen with this design, largely because of distal attachment problems. More recent endograft configurations have largely replaced the tube endograft.
Aorto-uni-iliac endografts (Figure 1C) attach proximally to the non-aneurysmal neck and distally to the iliac or femoral artery (10,11). The contralateral common iliac artery is then occluded with an endovascularly placed device, and flow is restored with a conventional femoral-femoral bypass. The advantages of this design are its relative simplicity of placement compared with a bifurcated system, especially in patients with severe tortuosity or narrowing of the iliac arteries. As such, its applicability is much greater. Utilizing this design with a “homemade” device, the group at Montifiere Hospital (NY) has been able to treat 80% of AAAs endovascularly (10). A theoretical disadvantage of this graft design is the extra-anatomic routing of blood to one leg via the femoral-femoral bypass. When used for occlusive disease, femoral-femoral bypass has distinctly inferior long-term patency rates when compared with “in-line” reconstruction with aortofemoral grafting (50% to 60% vs 85% to 90% at 5 years, respectively). However, as in these AAA cases, patency rates for femoral-femoral bypass may be higher in the absence of occlusive disease (11).
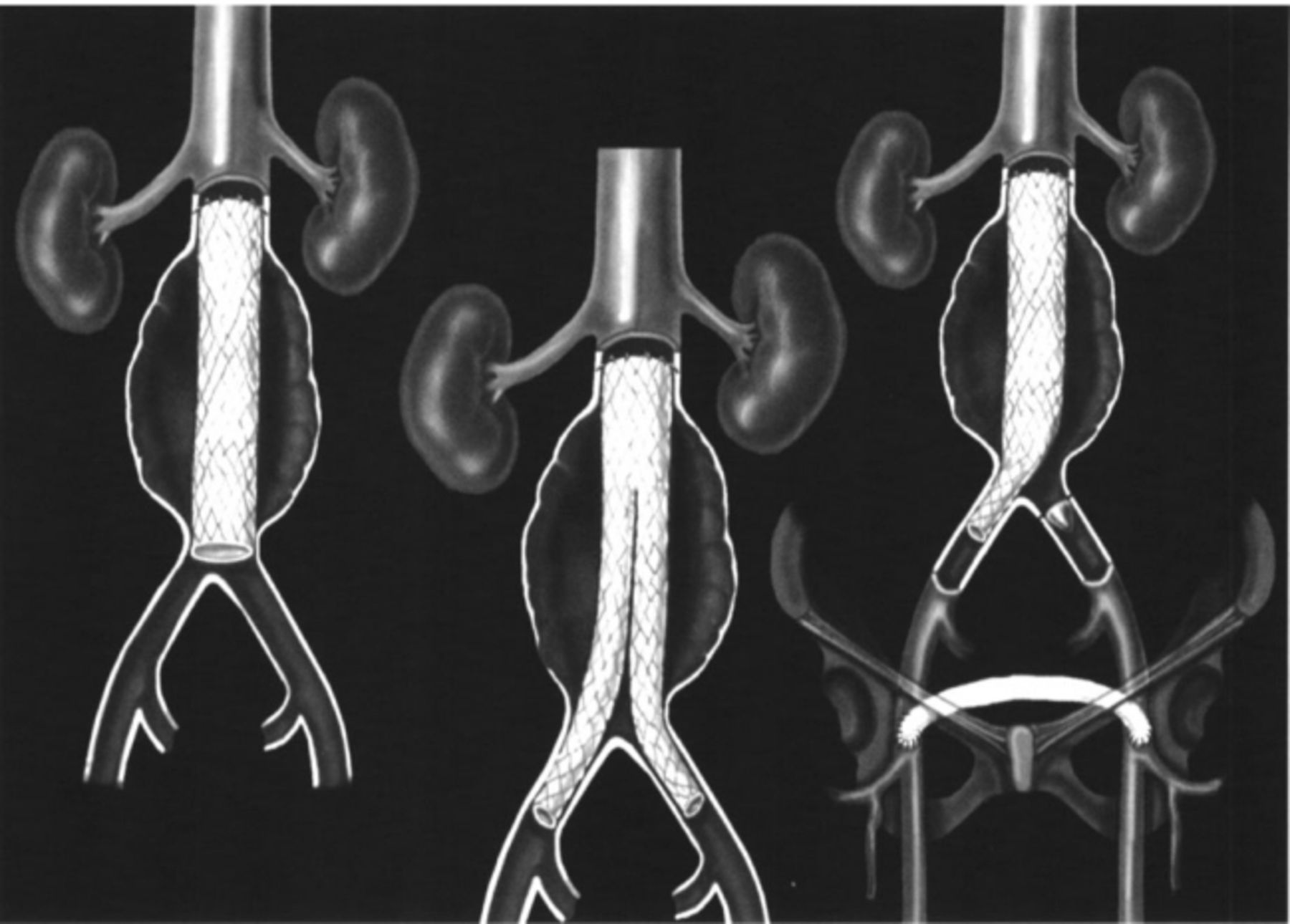
Endovascular tube graft (A), aorto-bi-iliac endograft (B), and aorto-uni-iliac endograft with conventional femoral-femoral bypass (C)
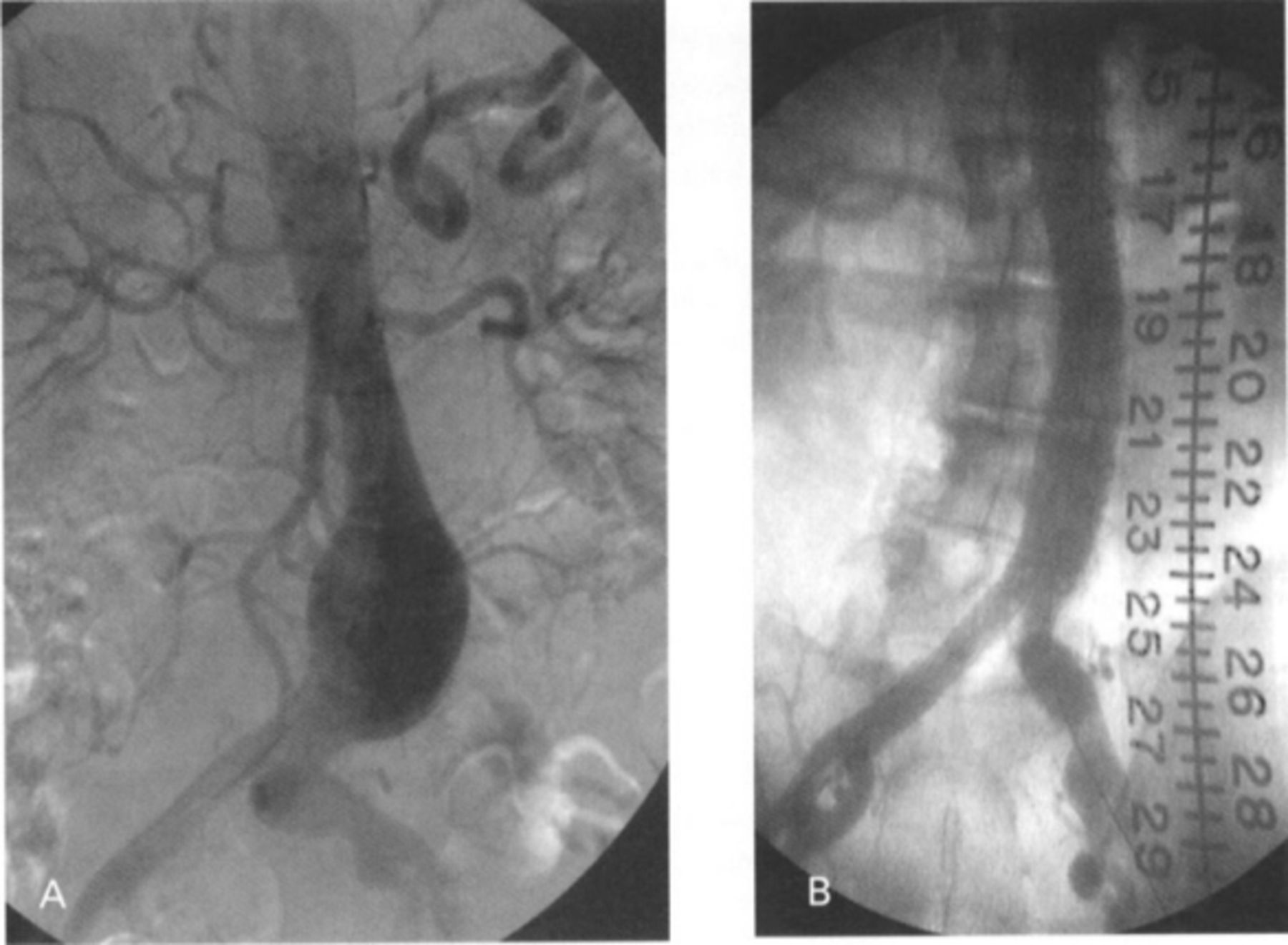
Aortogram demonstrating a AAA before (A) and after treatment with an AneuRx endograft (B)

CT scan demonstrating a AAA before (A) and after treatment with a AneuRx endograft (B). Note the two patent iliac limbs with no flow in the aneurysm sac (B)
Aorto-bi-iliac endografts (Figure 1B) are emerging as the most widely used graft configuration (3,5,6). These grafts overcome many shortcomings of the aformentioned configurations. A distal seal in the iliac arteries is more reliably obtained, and the graft provides in-line anatomic flow to the legs. These grafts are either unibody, with the entire device delivered via one femoral cutdown, or modular, with an iliac limb attached to the main device in vivo. The great advantage of the modular design is its ability to be customized to each patient's anatomic requirements at the time of implantation. Its potential drawbacks include increased difficulty in placement and the potential of leakage at the connection between the main device and the contralateral iliac limb. Current bifurcated endografts can repair 50% to 60% of AAAs.
At Ochsner, we have experience with all of these graft designs and currently favor the modular bifurcated configuration. At this writing, we have been the only institution in the Gulf South region participating in trials of endovascular repair of AAAs. Our initial experience was with tube, aorto-uni-iliac, and unibody bifurcated endografts manufactured by EVT (7) (Guidant Corp, Menlo Park, CA). Most recently, we have been utilizing the AneuRx (Medtronic, Santa Rosa, CA) device (3), a modular bifurcated graft which is constructed of a thin wall polyester with an exoskeleton of self-expanding nitinol metal stents. The main device is delivered via a 21 Fr system, and the contralateral iliac limb is delivered via a 16 Fr sheath. We are one of 12 sites in the United States conducting FDA phase II and III trials of this device.

Plain abdominal KUB showing metal exoskeleton of the AneuRx endograft
Ochsner Results
A total of 64 endografts for AAA treatment have been placed at Ochsner Foundation Hospital through April 1999. Between December 1995 and April 1997, 14 EVT endografts were placed; six tube, six bifurcated and two aorto-iliac devices. From September 1997 to April 1999, 50 AneuRx modular bifurcated endografts were implanted as part of FDA II and III clinical trials (Figures 2–4). The patient characteristics of these groups are presented in Table 1. Most patients were male, with significant co-morbidities as reflected in the American Society of Anesthesiologists (ASA) classification of 3.1-3.2. This classification scheme stratifies non-emergent operations from one to four, a greater number correlating with greater co-morbidities and therefore operative risk. Some patients deemed a prohibitive risk for open repair underwent endovascular repair on a compassionate use basis. These patients are included in the results. All endografts were implanted under investigational device protocols monitored by the Ochsner Clinical Investigations Committee. To be eligible for inclusion in these studies, the AAA had to be 5 cm or greater in size, rapidly expanding (>0.5 cm in 6 months), or saccular in morphology. Data are presented ±S.E.M.
Endografts were successfully deployed in 91% (58/64) of cases. Five patients required conversion to an open repair, 21% (3/14) in our early experience with the EVT devices and 4% (2/50) with the AneuRx device. One patient's iliac arteries would not accept the device, but this patient was not converted to open repair because of prohibitive co-morbid conditions.
There have been two postoperative deaths in the series, for a mortality rate of 3.1%. Both of these deaths occurred in patients who required immediate conversion to an open repair. Other investigators have also noted a significant mortality rate in patients requiring open conversion after unsuccessful endovascular repair (12). There have been three late deaths (3 months to 1 year) secondary to cardiac disease. Other adverse events related to endovascular repair are detailed in Table 2. Medical complications included pneumonia (1.6%), acute renal insufficiency not requiring dialysis (3.1%), stroke (3.1%), and gastrointestinal bleeding (1.6%).
Surgical time has decreased markedly for these endovascular procedures, currently at a mean of 2.5 hours (median 2.2 ± 0.2), down from 4.4 hours in our early experience (Table 3). Blood loss has also fallen, with only a small minority requiring blood transfusion. Finally, length of hospital stay (LOS) has been reduced, now at a mean of 2.7 days (median 2 ± 0.7). Several recent patients have been discharged on the first postoperative day.
In patients with 6 months of follow-up, the endoleak rate in the AneuRx group has been 10% (2/20 patients), similar to the 9% rate reported in the multicenter trial. The endoleak rate in EVT grafts has been higher (29%, 2/7). Two late secondary procedures have been performed to treat endoleaks: a laproscopic clipping of a patient's inferior mesenteric artery, and the placement of an aortic cuff. There have been no late conversions to an open procedure, and there have been no delayed AAA ruptures.
Discussion
Endovascular repair of AAA has the potential to revolutionize the treatment of this fairly common medical condition. Before any new form of treatment can supplant an existing one, however, it should attain comparable outcomes in regard to efficacy, durability, safety, patient comfort and acceptance, and cost.
Efficacy
The primary goal of AAA repair is to prevent rupture and subsequent hemorrhagic death. By replacing the aneurysmal segment of aorta with a prosthetic graft, open repair approaches 100% efficacy (primary immediate technical success). Successful endovascular repair of AAA excludes flow into the aneurysm by forming a hemostatic seal at the proximal and distal attachment sites. Continued perigraft flow into the aneurysm is known as an “endoleak.” Efficacy of endovascular treatment of AAA is critically dependent on the initial success rate of graft placement, prevalence and type of endoleak, and incidence of late rupture of AAA despite endovascular repair.
Demographics of patients with AAA treated with endografts from two manufacturers.
Adverse events in Ochsner AAA patients treated with endografts from two manufacturers.
Results of AAA endovascular treatments at Ochsner using endografts from two manufacturers.
While early tube endografts were associated with a 15%-20% rate of conversion to open operation (7), more recent reports with bifurcated devices show similar low conversion rates of 1%-5% (3,5,13). Improvements in graft design as well as operator experience share the credit for this significant improvement. We have found the modular bifurcated system especially useful in customizing endovascular repairs that would have otherwise required open conversion with earlier graft types. Severely angulated aortic necks and small, tortuous iliac arteries continue to be the major causative factors for unsuccessful endograft placement.
Type I endoleaks result from a non-hemostatic seal from the proximal, distal, or pant leg connection (14). Type II endoleaks occur from persistent collateral channel flow in the aneurysmal sac, most frequently from the lumbar and/or inferior mesenteric arteries. While Type I endoleaks are considered more dangerous, patients with Type II endoleaks have had continued aneurysmal expansion and even rupture.
The rate of endoleaks in early tube graft systems such as EVT were as high as 44% (7), but most recent studies with bifurcated systems have endoleak rates of 5%-10% (3,5,13). Many Type II endoleaks will seal without intervention, although coil embolization of collateral vessels or laparoscopic clipping of the internal mammary artery may occasionally be necessary. Type I endoleaks generally require adjunctive endovascular intervention. Patients with persistent endoleaks and an AAA expansion of 5 mm should be considered an endovascular treatment failure and converted to open repair. Late failures culminating in AAA rupture despite endovascular treatment have been reported (15,16).
The efficacy of endovascular repair of AAA has improved dramatically in the last several years with the introduction of second-generation devices. At present, efficacy as measured by the above parameters is approaching, but not equal to, that of open repair.
Durability
The durability of open AAA repair is excellent. In its widespread use over the last several decades, numerous reports have shown 5, 10, and even 20-year follow-up (17). Risk of delayed rupture of the original aneurysm is essentially zero. Modern graft fabrics may dilate modestly over time, but a primary failure/tear would be reportable. Late anastomotic pseudoaneurysms can occur in 0.296-5% with potential for rupture (18). Long term primary patency is 85%-95% at 5 years.
The durability of endovascular AAA is largely unknown. Large-scale trials have been enrolling patients in only the last 2 to 3 years. At this writing, most studies are just beginning to collect 1 to 2 year follow-up data. Some early graft designs had structural failures, including anchor barb fractures (7) and graft fabric tears (5), which became evident within the first year of placement. These product failures are not unexpected with completely new technology and have subsequently been corrected. Primary graft failures with current second-generation devices have not been reported.
Some late graft failures are now being seen as a consequence of aneurysmal sac shrinkage and remodeling (19). These changes in the excluded aneurysmal sac have caused graft dislodgment or kinking of an iliac limb. While reports of these late endograft failures have been relatively few, only further close follow-up will reveal the true incidence of this complication. Some endografts may be more susceptible to these late changes than others (20).
Safety
The perioperative mortality rate has been considered the single most important outcome parameter in AAA repair. Recent single center institutional series of open repair of non-ruptured AAA report mortality rates of l%-4% (17,21,22), with a mean of 2% to 3%. Multicenter and population based studies tend to have higher rates of 4% to 6% (23,24). Mortality rates for endovascular AAA repair have ranged from 0 to 4.2% (3,5,6,7,12,13). Most deaths have occurred in patients at too high risk for open repair (7/8 deaths in May series, 4.2%) (13), or have occurred early in a clinical experience. In the AneuRx study, mortality was reduced from 7.5% (3/40) in Phase I to 1.3% (2/150) in Phase II, suggesting that there is a significant learning curve, both with the technique as well as proper patient selection (3).
To date, mortality rates of endovascular AAA repair are at least comparable to those of open repair. When similarly designed studies are compared (ie, multicenter to multicenter), mortality may be lower with endovascular repair.
Major morbidity occurs in 15%-30% of patients after open AAA repair, partly because of the advanced age and prevalence of co-morbid conditions in this patient population (25). As documented in the AneuRx trial (3) comparing open vs endovascular repair of AAA, the latter was performed faster (3.1 hours vs 3.6 hours), with 66% less blood loss (641 ml vs 1596 ml), and without the requirement of general anesthesia. As presented, our operative times (2.7 hours) and blood loss have been similar to this multicenter cohort. Major morbidity was significantly less in the endovascular group vs open repair (12% vs 23%) in the AneuRx study (3). Interestingly, this difference was due to fewer medical complications; surgical complications requiring intervention were similar between the groups. Reported morbidity includes iliac limb occlusion or limb ischemia (1%-12%), need for dialysis (0 to 4%), and peripheral embolization (0 to 5%) (3,5,6,7,8,12).
In summary, endovascular AAA repair appears to be safe, with mortality rates trending lower than for open repair. Major medical morbidity also appears to be reduced, while surgical morbidity is fairly equivalent. As devices and experience improve, the surgical morbidity may fall to levels below that of open repair.
Patient Comfort/Acceptance
Open AAA repair requires a large painful abdominal incision, a 6 to 10 day hospital stay (national mean 9 days), and a 3 to 6 week convalescence. Endovascular repair affords much smaller incisions with a concomitant reduction in pain, decreased hospitalization by two-thirds, and a markedly shortened postoperative convalescence. Clearly, minimally invasive surgery such as this has tremendous appeal to patients. As laparoscopy has forever changed the treatment of gallbladder pathology, so will endovascular procedures change the treatment of AAA. Our patients will not only expect minimally invasive alternatives, they will demand them. It will be incumbent on physicians to ensure that this treatment is indeed efficacious and durable when compared with conventional therapy. As presented, not enough long-term data are available to render a definitive response to these last very important questions.
Cost
Innovation in medicine, whether it be new technology or new medication, is usually costly; endovascular grafts for treatment of AAA are no exception. While conventional grafts used in open repair cost $400 to $700, aortic endografts pricing will likely be 10-15 fold higher. Savings afforded by reductions in hospital length of stay may not be enough to offset this substantial graft cost (26). Because the majority of treatment of AAA is performed on Medicare patients with a fixed DRG payment to the hospital, these increased costs cannot be “passed on” to third party payers. As such, hospitals may be reluctant to embrace a technology whose use generates a net loss to their facility.
Conclusion
In this early stage of development, endovascular repair of AAA potentially represents a quantum improvement in the management of this common problem. Early data suggest that mortality rates may be lower and overall morbidity decreased compared with open repair, with a significant reduction in length of hospital stay and convalescence. If further follow-up of these cases reveals excellent long term efficacy and durability, most AAAs in the future will be repaired endovascularly.
Acknowledgments
We would like to thank Nicole Manord, RN, for her tireless work as research coordinator for these studies, and Susan Majorie, RN, for the data collection and tabulation used in this article.
- Academic Division of Ochsner Clinic Foundation
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
In this issue








{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.