
Abstract
Background: Opioid-based anesthetic techniques are commonly used during neurosurgical procedures. In the present randomized prospective study, we studied emergence after 4 anesthetic regimens combining intermediate duration opioids with isoflurane and nitrous oxide (N2O), in patients undergoing craniotomy for large (> 30 mm diameter with intracranial mass effect) intracranial tumors.
Methods: One hundred seven patients were randomized into 4 groups: Group A: fentanyl (≤ 5 µg/kg) + isoflurane (≤ 1 minimum alveolar concentration [MAC]), Group B: sufentanil (1-2 µg/kg plus infusion) + isoflurane (≤ 0.5 MAC), Group C: sufentanil (2 µg/kg bolus only) + isoflurane (≤ 1 MAC), and Group D: alfentanil (100 µg/kg plus infusion) + isoflurane (≤ 0.5 MAC). Boluses were administered as divided doses during induction, laryngoscopy, head pinning, and incision. Blood pressure was controlled at ±25% of baseline levels. All infusions were discontinued at the start of dural closure. Emergence was assessed using a mini-neurologic examination consisting of 7 questions. Groups were compared on time to emergence using survival analysis methods.
Results: The groups did not differ regarding extubation time, which occurred at a median of 4 to 6 minutes across groups after discontinuing N2O. The median emergence time ranged from 15 to 22.5 minutes and did not differ among groups. However, across all groups more women had emerged by 30 minutes compared with men (83% vs 57%, P = .002). The median emergence time in women was found to be significantly shorter (0-15 minutes) than in men (15-30 minutes) (P = .012).
Conclusions: No between-group differences in emergence time were observed; the study was stopped early because of evidence that no differences were likely to be found if the study were continued. However, in a post hoc analysis, female gender was associated with faster emergence.
- Alfentanil
- anesthetic drug combinations
- craniotomy
- delayed emergence
- fentanyl
- intracranial tumor surgery
- sufentanil
INTRODUCTION
Our prior work has associated delayed emergence (DE) with large intracranial tumor size.1 Nevertheless, anesthetic technique has been implicated as one of the most important factors influencing emergence.2-5 Appropriate matching of anesthetic dose to changing demand is therefore necessary to avoid relative overdose and is often accomplished with intermediate duration agents. Accordingly, we studied regimens primarily relying on volatile anesthetics as well as 2 opioids of intermediate duration: alfentanil and sufentanil. Anticipatory dosing of opioids encountered during craniotomy is advantageous to counteract stimuli. On the other hand, bolus plus infusion regimens have also been used successfully.6,7 We therefore also compared regimens with both an anticipatory bolus dosing scheme and a continuous infusion of opioids with respect to their effect on timely emergence.
MATERIALS AND METHODS
After institutional review board approval and written informed consent, American Society of Anesthesiologists physical status II and III patients scheduled to have elective, partial, or total excision of a brain tumor were enrolled. Preoperatively, patients were awake and oriented to time, place, and person and could follow commands. Patients with significant cardiopulmonary disease or those taking sedatives or opioids regularly were excluded. Anticonvulsants, antihypertensives, and steroids were continued until the morning of surgery.
Only patients with lesions associated with mass effect (supratentorial tumors > 30 mm, midline shift of > 3 mm and/or ventricular effacement and/or significant edema) were included. These characteristics are known to be associated with intracranial pressure elevations and have indicated higher neurologic risk in the perioperative period.8,9 Standard preoperative laboratory studies were obtained, and all patients had a 12-lead electrocardiogram and either a computed tomography or magnetic resonance imaging scan before surgery. No intramuscular premedication was given. Patients were randomized into 4 groups as shown in Table 1. Boluses were administered as divided doses during induction, laryngoscopy, head pinning, and incision. Blood pressure was controlled within 25% of baseline levels. All infusions were discontinued at the start of dural closure. Isoflurane and nitrous oxide (N2O) were discontinued during skin closure and after application of the head dressing, respectively.
Anesthetic Regimens A, B, C, and D Used in This Studya
All patients were evaluated for neurologic status immediately on arrival in the neurointensive care unit or postanesthesia care unit, then every 15 minutes for the first hour, then every 30 minutes for the next hour, and then hourly for the next 24 hours. Degrees of DE were determined with a mini-neurologic examination consisting of a series of 7 questions (open eyes; squeeze hand or move feet; stick out tongue; say name, day, or date; name place; name the current US President; and identify own last name). The time at which the patient was first deemed awake (at least 4 of 7 responses present) was used for the statistical analysis as emergence time.
Statistical Analysis
Sample size calculations were made based on previous observations by our group. To detect a clinically relevant difference in median time to emergence (15 vs 30 minutes) with 80% power at an overall significance level of 0.05 (Bonferroni correction for 6 pairwise comparisons), we would have needed approximately 55 patients per group, for a total of 220.
All data were analyzed using SAS software (SAS Institute Inc, Cary, NC) and are presented as mean values ± standard deviation or median (first quartile, third quartile). A time-to-event Kaplan-Meier analysis was performed to assess the pattern of awakening for each anesthetic regimen and to compare groups on time to awakening with a log-rank test. A time-to-event Kaplan-Meier analysis was also performed to assess the pattern of awakening for each gender. Cox proportional hazards regression analysis was used to compare groups on time emergence while adjusting for potential confounding variables. Groups were compared univariably on the dichotomous emergence outcomes at 15 and 30 minutes with either a chi square or Fisher exact test and on continuous outcomes with analysis of variance (ANOVA) or the Kruskal-Wallis nonparametric test, as appropriate. The significance level was 0.05 for each hypothesis, and a Bonferroni correction was used to maintain this significance level when making multiple comparisons.
RESULTS
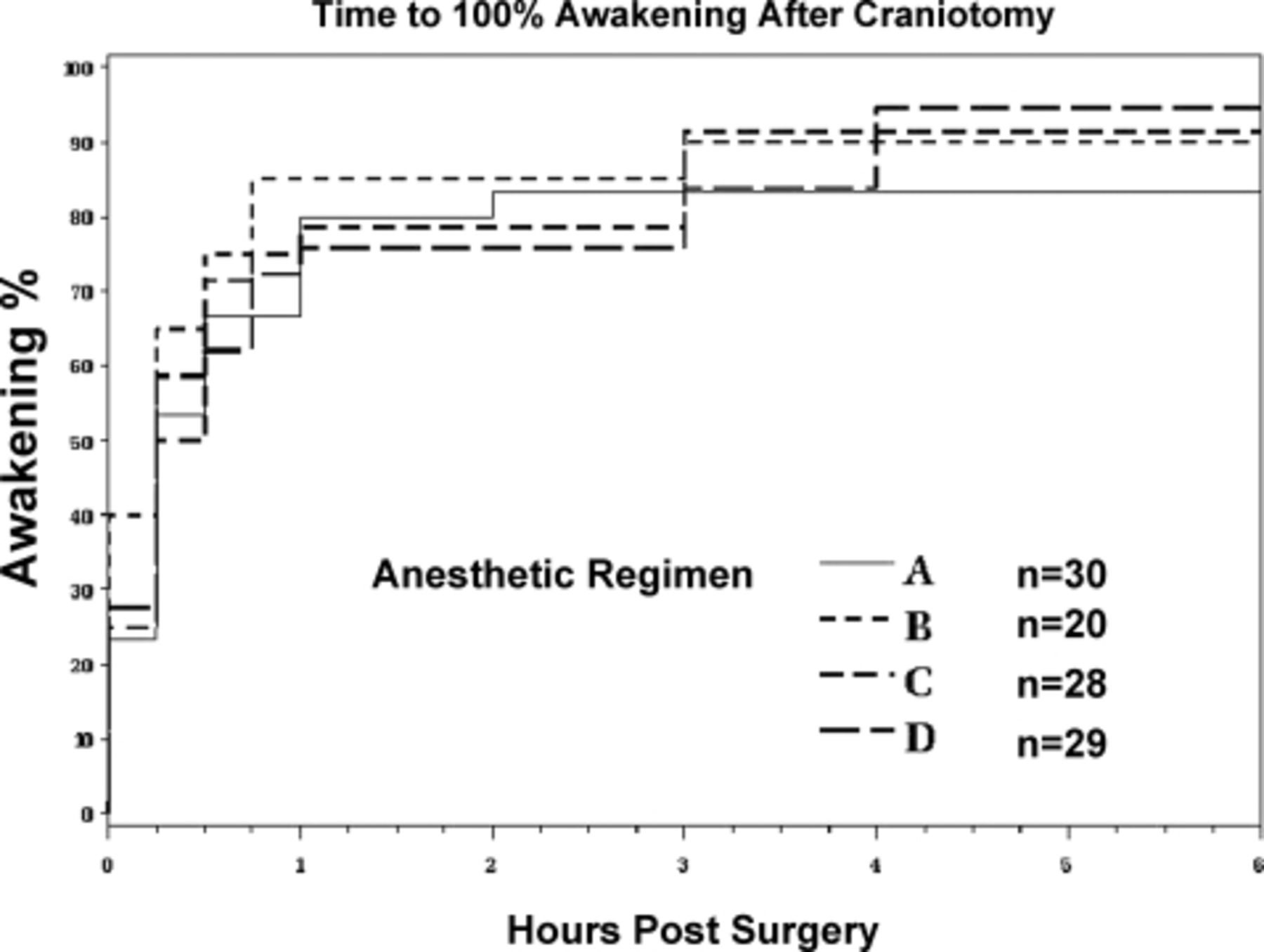
A total of 107 patients were studied. Patient characteristics for all the groups are described in Table 2. Surgical conditions were similar in all groups. No significant differences among the groups were identified for any of these variables except gender. Operative data are shown in Table 3. Group A (anticipatory dosing, volatile agent-based technique) received a higher mean total thiopental dose than Groups B, C, or D. Emergence outcomes at 15 and 30 minutes are shown in Table 4. Ten patients had not reached emergence criteria by 24 hours (1 in Group A, 2 in Group B, 3 in Group C, and 4 in Group D). Seven patients, although still tracheally intubated, were able to perform the squeeze hand or move foot functions and were deemed awake. Figure 1 shows that the pattern of awakening (Kaplan-Meier curves) was similar across the groups. By 15 minutes, 53% (95% confidence interval [CI], 35%-71%) in Group A had awakened, with 65% (95% CI, 44%-86%) in Group B, 50% (95% CI, 31%-69%) in Group C, and 59% (95% CI, 41%-77%) in Group D. The estimated time for 50% of patients awakening (median time) was 15 minutes in Groups A, B, and D and 22.5 minutes in Group C. No significant difference in awakening time was found among the groups (overall log rank P = .80). A conditional power analysis10 on the primary outcome of time to emergence indicated that if the current trend continued, the probability of rejecting the null hypothesis if the study were continued to the planned number of patients (n = 55 per group) was less than 20%. The study was therefore stopped at 107 patients.

Kaplan-Meier curves for the 4 anesthetic regimens. There was no difference in emergence performance (P = .80).
Patient Characteristicsa
Operative Data
Emergence Outcomes at 15 and 30 Minutes
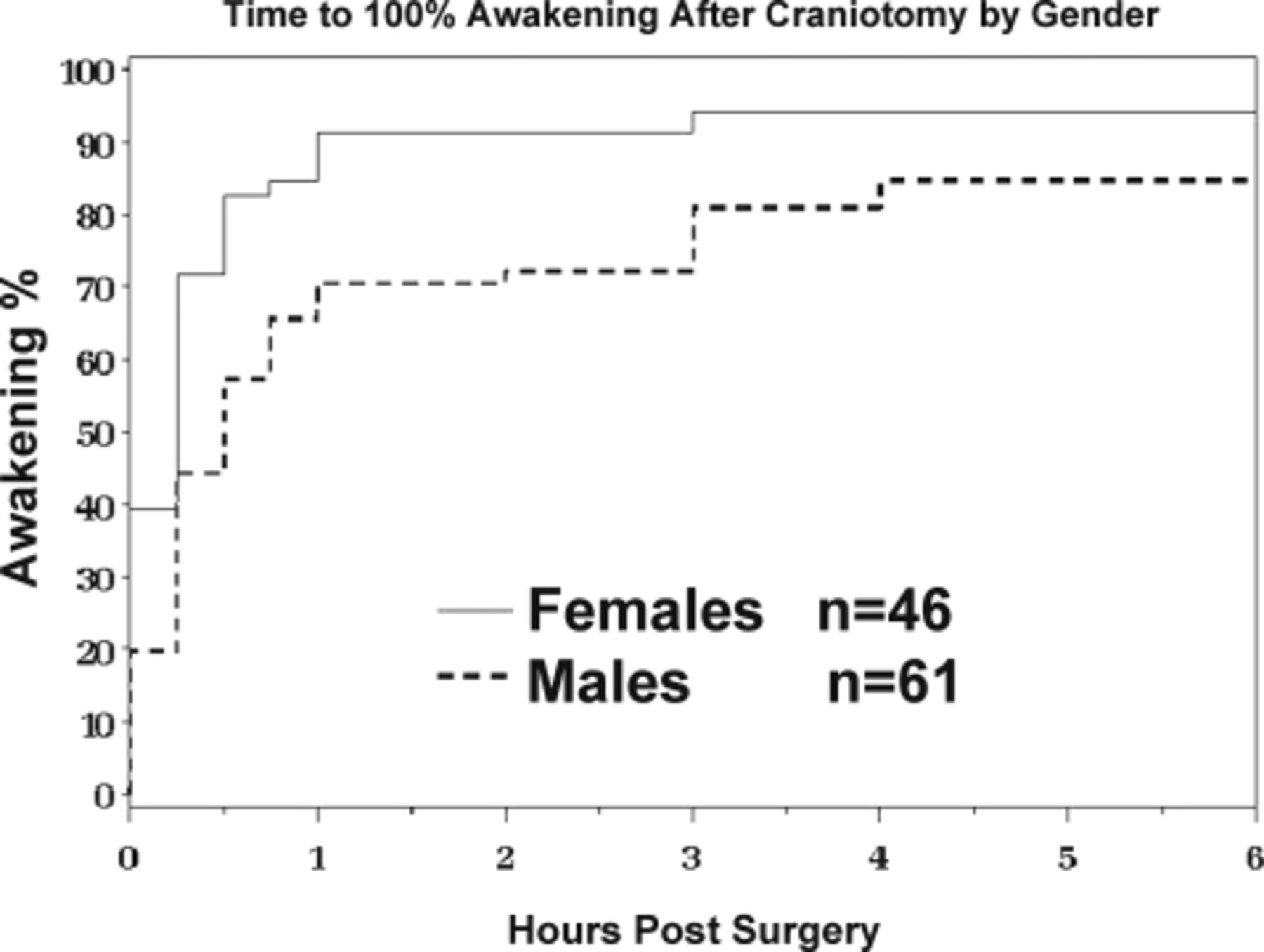
Gender was assessed as a potential confounder and modifier of the treatment effect. More women had emerged by 30 minutes compared with men (83% vs 57%, P = .002). The median emergence time in women was found to be significantly shorter (between 0 and 15 minutes) than in men (between 15 and 30 minutes) even after correcting for anesthetic regimen with the Cox proportional hazards model (P = .012). The Kaplan-Meier curves are displayed in Figure 2.

Kaplan-Meier curves for both genders. Emergence was significantly slower in males (P = .012).
DISCUSSION
The present study suggests that several combinations of intermediate duration opioids with isoflurane and N2O may be equivalent regarding speed of emergence from craniotomy for large brain tumors. Consistent with observations in general surgical patients,11-13 we also observed via a post hoc analysis that women undergoing intracranial neurosurgery emerged significantly faster than men.
Our inability to show differences in emergence speed with the anesthetic regimens chosen is consistent with prior observations. In a double-blinded prospective evaluation of 45 patients, From et al14 compared fentanyl, sufentanil, and alfentanil bolus plus infusion regimens in patients undergoing craniotomy and found no difference in level of consciousness postextubation or 30 minutes after arrival to the recovery area. Mutch et al7 reported no difference between fentanyl and alfentanil groups in 33 patients undergoing supratentorial craniotomy regarding emergence times to eye opening, extubation, or postanesthetic respiratory depression. Likewise, Grundy et al15 compared 2 groups of craniotomy patients each receiving either sufentanil or fentanyl and thiopental and N2O with a third group receiving only isoflurane and N2O. Again no differences in the time from discontinuing the anesthetic to eye opening were found.
Yet emergence after craniotomy may be influenced by the anesthetic regimen under certain conditions. Van Hemelrijck et al5 showed that a total intravenous anesthetic technique (propofol and alfentanil) was associated with more predictable emergence and shorter awakening time compared with thiopental, N2O, fentanyl, and isoflurane. The time from awakening to correct orientation was 7 ± 5 minutes versus 27 ± 23 minutes, and the time to correct performance of a test of mental concentration was 12 ± 12 minutes versus 35 ± 37 minutes. Todd et al16 compared 3 groups (propofol and fentanyl, isoflurane and N2O, and fentanyl and N2O) in patients undergoing supratentorial craniotomy, identifying a somewhat faster emergence (5 vs 10 minutes) with the fentanyl and N2O technique. Because gender and tumor size may influence emergence after craniotomy,1 studies seeking to define relationships between anesthetic interventions and emergence speed should account for the effects of the former. All patients in the present study had large tumor masses, making it unlikely that intracranial pathology obscured major differences in emergence speed. Our study protocol incorporated strict guidelines for the management of blood pressure, response to stimulating events, and discontinuance of anesthetics, decreasing the likelihood that individual practice patterns influenced emergence.
We did not include a group using the rapidly eliminated semisynthetic opioid remifentanil because we wanted to concentrate on opioids with similar pharmacokinetics (elimination half-lives of 110-500 minutes17). In spite of certain pharmacodynamic and pharmacokinetic differences among the 3 opioids that we used, few differences in their efficacy profile are observed for their use during craniotomy.18
The complex pharmacokinetic behavior of lipophilic opioids has been described by several investigators who introduced the concept of context-sensitive half-time. The time required for the plasma drug concentration to decline by 50% after terminating each infusion is referred to as the context-sensitive half-time, where context refers to infusion duration. The context-sensitive half-times for fentanyl, alfentanil, and sufentanil are markedly different from their respective elimination half-lives, but this relationship depends on the duration of the infusion.17 For example, although the context-sensitive half-lives for alfentanil, sufentanil, and fentanyl are 50 to 60 minutes, 25 to 40 minutes, and 100 to 125 minutes at 3 hours, respectively, they are 50 to 60 minutes, 40 to 50 minutes, and 250 to 300 minutes, respectively, at 8 hours of infusion duration.17 Because context-sensitive half-life describes the time to halving of the drug's plasma concentration after the infusion is stopped, this concept may be practically more useful than elimination half-lives in describing postinfusion recovery from opioid effect. For example, although sufentanil has a longer distribution and elimination half-life compared with alfentanil, emergence from sufentanil infusion may be similar to alfentanil infusion.19 These considerations explain, in part, why no difference in emergence time was seen in our study groups.
Evidence is increasing that gender may be an important determinant of recovery from general anesthesia, with females awakening faster than males. In a multicenter study of 274 general surgical patients, Gan et al11 demonstrated that time from end of anesthesia to eye opening was significantly less in women than in men (7.05 minutes vs 11.22 minutes, P < .05). Myles et al12 observed that women emerged significantly more quickly than men in 463 elective inpatients (11.3 minutes vs 13.4 minutes, P = .003 for eye opening and 12.4 minutes vs 15.3 minutes, P = .002 for obeying commands). Similar findings were reported in patients undergoing laparoscopic cholecystectomy. Women awakened faster than the men (6.6 minutes vs 11.6 minutes, P < .01). At emergence, there was a trend toward higher bispectral index values in women.13 Reanalysis of results from a large multicenter trial in volunteers demonstrated significantly higher bispectral index values in women when compared with men at the same plasma propofol concentration.20 Although multiple factors influence recovery from anesthesia, gender has emerged as a consistent effect across different patient populations and anesthetic regimens. Our results in patients undergoing craniotomy for brain tumor resection are consistent with these observations.
In patients who receive opioids intraoperatively, emergence characteristics have also been shown to be influenced by age,21 gender,22 and race.23 In vivo studies also suggest the existence of important gender-related differences in opioid-mediated analgesia.24 Prospective human studies on the interaction of gender and the analgesic or sedative effects of opioids, however, are scarce. Kappa opioids (nalbuphine, butorphanol) were associated with better pain relief in female than in male patients.25 Gender-based differences in opioid-mediated analgesia are likely the result of both pharmacodynamic and pharmacokinetic factors, although some evidence favors the former.26,27
Readers should consider a number of limitations in their interpretation of the findings of this report. First, the anesthetic regimens may not have been equivalent in their anesthetic potency; this, along with differences in other unaccounted factors, may have served to falsely equalize emergence speed among groups. Nevertheless, the regimens used have been reported previously and have been used clinically. Furthermore, opioid and minimum alveolar concentration doses were indeed roughly equivalent.28,29 Second, the study was not powered to detect small differences in emergence time. It is therefore possible that the equivalence in emergence time between the 4 groups was due to a type II statistical error. Third, the observation that female gender was associated with faster emergence across all groups was made post hoc and is therefore subject to exclusion bias. Table 2 indicates that the male and female gender groups were roughly comparable regarding anesthetic and other factors that could influence emergence speed. Sample size was calculated based on previously observed data from our group. To detect a fourfold difference with 80% power at the 0.05 significance level, approximately 60 patients per group were needed. Yet even an interim analysis provided evidence of a gender effect on emergence, strengthening our conclusion that females indeed may awaken faster from craniotomy for large tumor removal.
CONCLUSIONS
Our results therefore support the notion that isoflurane and N2O when combined with fentanyl, alfentanil, or sufentanil result in similar emergence characteristics after craniotomy for large intracranial tumors, recognizing that this study was not powered to detect small differences in emergence time. Neither the type of intermediate duration opioid used nor the method of administration (bolus vs infusion) appears to influence emergence to the degree that other factors do, such as size of intracranial tumor and gender. Our observations add to a growing body of evidence that points to the importance of gender as a determinant of the response to anesthetics and analgesics. Studies of emergence from anesthesia and anesthetic drug effects need to be designed specifically to address the repeatedly shown faster emergence of women in different patient populations regardless of the anesthetic regimens used.
- Academic Division of Ochsner Clinic Foundation
REFERENCES
In this issue








{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.