
Abstract
A new technique for the management of medial ectropion with a mild to moderate cicatricial component is presented that avoids the necessity for skin grafting. A subciliary incision is made inferior to the punctum and extending laterally, followed by preseptal dissection to the orbital rim. A base-up triangle of the posterior lamella is then excised lateral to the punctum. This is closed with a marginal mattress suture. Tightening of the posterior lamella in this fashion produces laxity in the anterior lamella, which can then be closed without tension, eliminating the need for skin grafting.
BACKGROUND
Medial ectropion repair has been approached by a variety of surgical techniques that attempt to tighten or shorten the medial eyelid without compromising the nasolacrimal system. The problem can be further complicated by contraction of the anterior lamella due to cicatricial forces from various causes (actinic changes, rosacea, prior surgery, or trauma).
The goal of surgery is to restore the proper anatomic relationship of the lid margin with the globe, either by releasing the anterior traction and grafting the defect with a free graft or a pedicle graft or by shortening the posterior lamella with a medical conjunctival spindle or with a lazy-T procedure.1 Given the cosmetic shortcomings of free grafts, the lazy-T is usually preferred, but a new approach eliminates the need for cicatrization of the posterior lamella.
METHODS
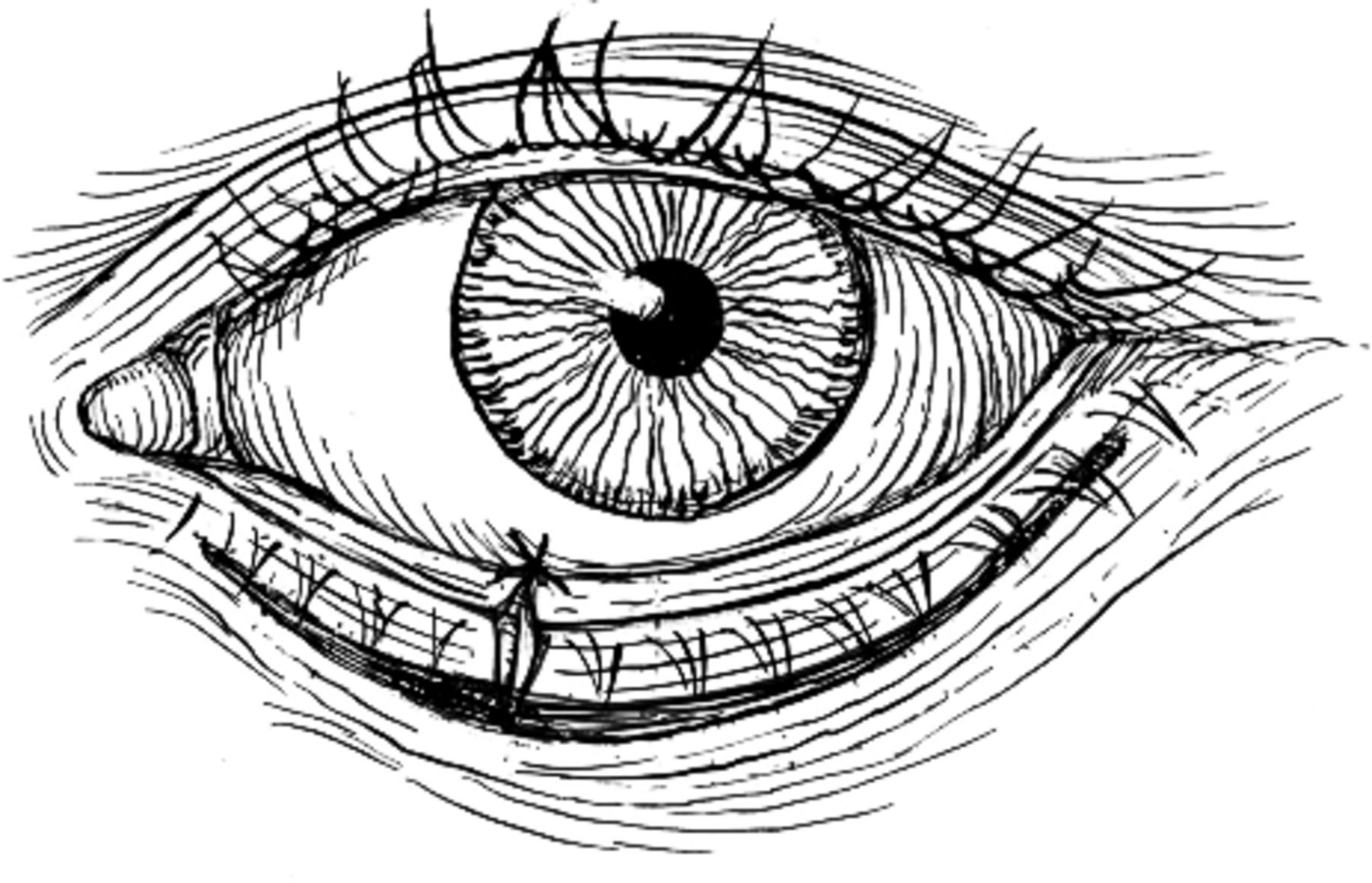
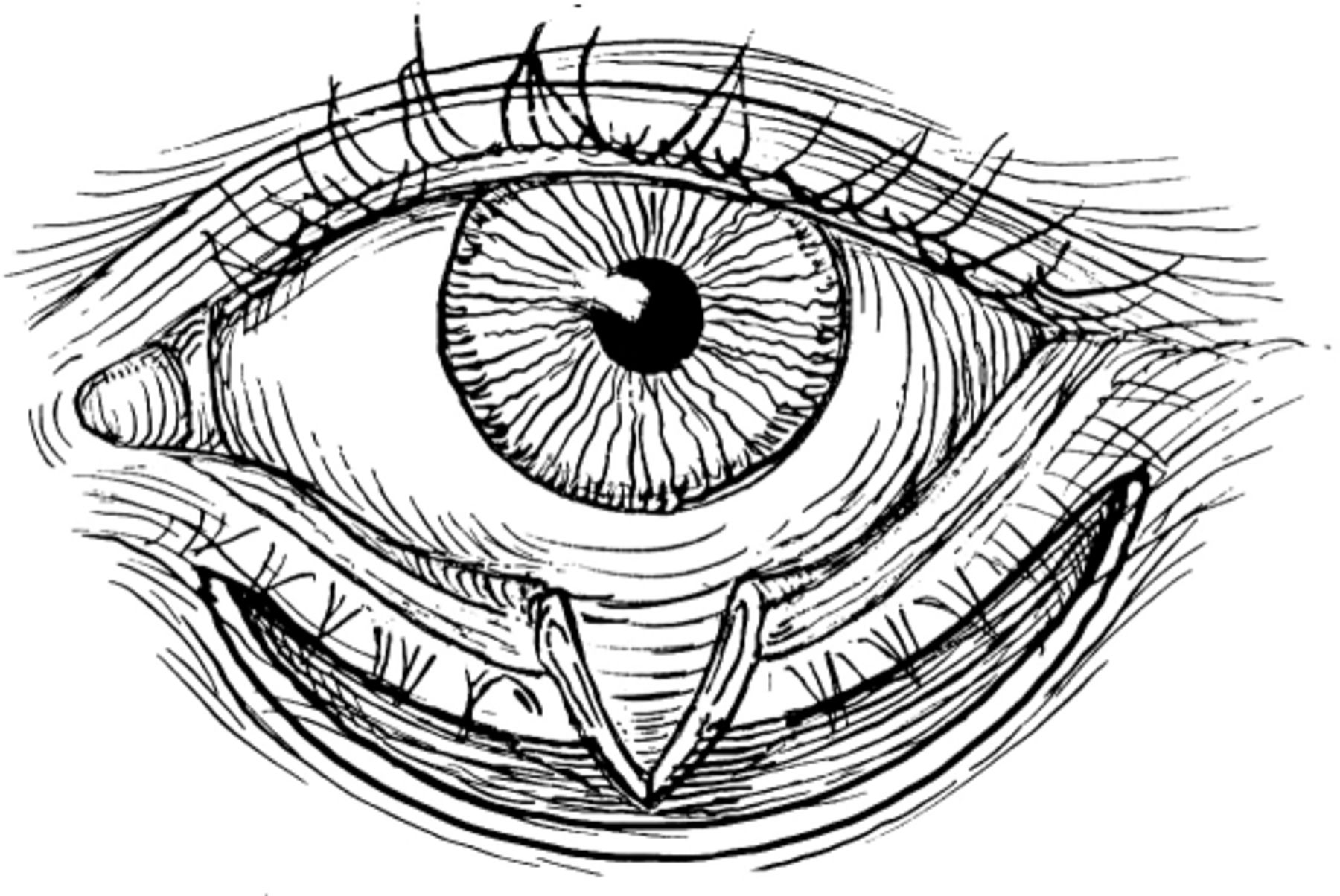
A subciliary incision is made 3 mm inferior to the punctum and extended laterally (Figure 1). The preseptal plane is then dissected down to the level of the orbital rim and hemostasis obtained (Figure 2). This produces a gap due to the tight anterior lamella (Figure 3). A base-up triangle of the posterior lamella (lid margin, tarsus, and conjunctiva) of sufficient size is then excised to effect a good apposition of the lid margin with the globe. This is closed with a deep tarsal suture and a mattress suture at the margin (Figure 4).

Subciliary incision.

Release of contraction and resultant gap.

Defect in tarsus prior to closure.
Closure of posterior lamella.
This horizontal shortening induces a laxity in the anterior skin/muscle layer, allowing closure without vertical traction (Figure 5). Theoretically, a conjunctival medial spindle could also inwardly rotate any residual punctal eversion, but this is rarely necessary.

Closure of anterior lamella.
RESULTS
A preoperative photo (Figure 6) shows left lower lid ectropion more prominent medially and tight anterior lamella. In Figure 7, results are evident at 1 week postoperatively.

Preoperative photo of ectropion left lower lid secondary to prior surgery for basal cell carcinoma, more prominent medially with tight anterior lamella.

Postoperative result at 1 week.
DISCUSSION
Cicatricial ectropion as described should be differentiated from eyelid retraction as in Graves disease. Thyroid ophthalmopathy involves the lower lid retractors and requires separate techniques of evaluation and management.
This technique is designed for mild to moderate tightening of the skin associated with some involutional laxity of the tarsus and medial canthal tendon. The surgical effect is insufficient in severe cases, as from burns or radiation, which still require grafting, as do some localized dermatologic conditions such as T-cell lymphoma or scleroderma. One can evaluate this by manually elevating the lower lid margin to estimate the degree of anterior contraction and then selecting the technique appropriate for the pathology. In some patients, attention must also be given to the upper midface and resupporting the orbitomalar ligament through a separate incision.
- Academic Division of Ochsner Clinic Foundation
In this issue








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.