
Abstract
Closed digital artery injury with secondary acute ischemia is a rare phenomenon. The most common injury pattern involves a crush mechanism with a resultant transverse fracture in proximity to the interphalangeal joints. Secondary acute ischemia requires urgent surgical exploration with digital arterial repair to avoid necrosis and associated decreased hand function. One should exercise an air of caution when examining significant closed trauma; neurovascular normality should be established by an adequately trained physician. We present a case of closed digital artery injury with secondary acute ischemia and a review of current literature.
The occurrence of digital artery injury with secondary acute ischemia is seldom associated with closed trauma; only 10 such cases have been documented thus far.1–⇓3 We present a case of closed digital artery injury, review the related literature, and discuss the associated implications.
CASE REPORT
A 36-year-old, otherwise fit and well, manual worker sustained a right hand crush injury with a 1-ton industrial chain. He presented with a painful index finger with vascular compromise as evidenced by pallor, coolness, and capillary emptiness. The finger was neurologically intact, without tendon injury, and with no skin breach over the zone of injury. A dorso-ulnar transverse laceration was, however, present over the fifth metacarpal head along with a superficial longitudinal laceration on the radial side of the fifth middle phalanx. All other digits were outside the zone of injury and neurovascularly intact. X-ray imaging showed a transverse proximal phalanx fracture of the right index finger along with dorsal dislocation of the little finger proximal interphalangeal joint (Figure 1).

Right hand x-ray demonstrating a transverse proximal phalanx fracture of the index finger and a dorsal dislocation of the little finger proximal interphalangeal joint.
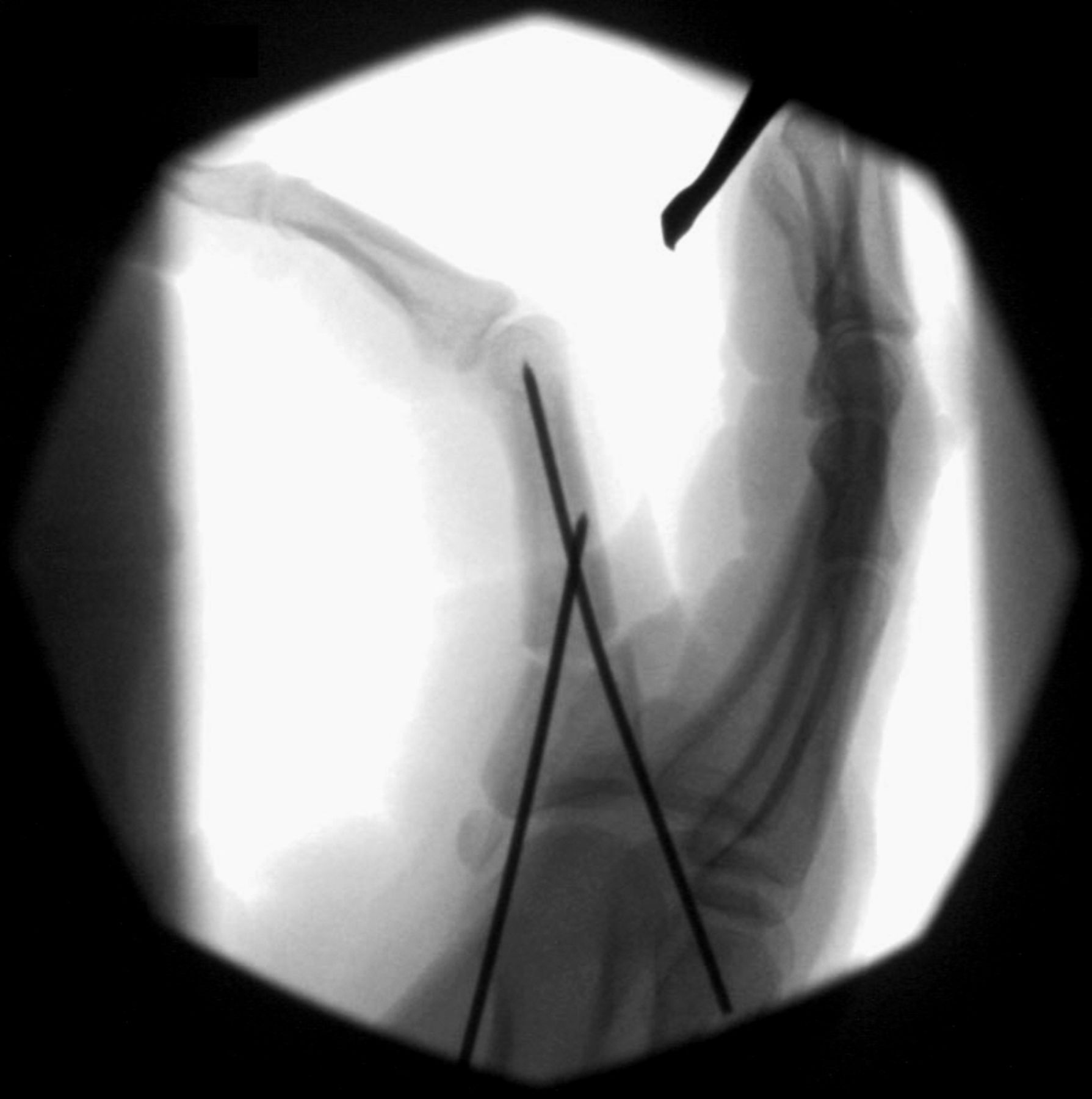
Urgent surgical exploration was organized for a preoperatively nonperfused finger based on clinical findings, with operative time lasting 90 minutes. Initial fracture reduction did not achieve index finger reperfusion. A modified Bruner incision was made (Figure 2); the radial neurovascular bundle was identified, and although the nerve was intact, the artery demonstrated transection at the level of the fracture (Figures 3 and 4). Primary radial digital artery repair with 10-0 nylon under microscopic magnification restored finger perfusion (Figure 5; compare to Figure 2). A full-thickness skin graft was used to cover the surgical wound to minimize compression on the arterial repair. The ulnar neurovascular bundle was not explored because clinically the ulnar digital nerve was intact and perfusion was restored with unilateral artery repair. The little finger proximal interphalangeal joint was manipulated and reduced. The index finger fracture was reduced and fixed with two 1.2-mm K-wires (Figures 6 and 7). All lacerations were explored, noted to be superficial, debrided, and closed primarily. The right hand was splinted dorsally.

Intraoperative nonperfused finger with modified Bruner incision.

Intraoperatively intact radial digital nerve.
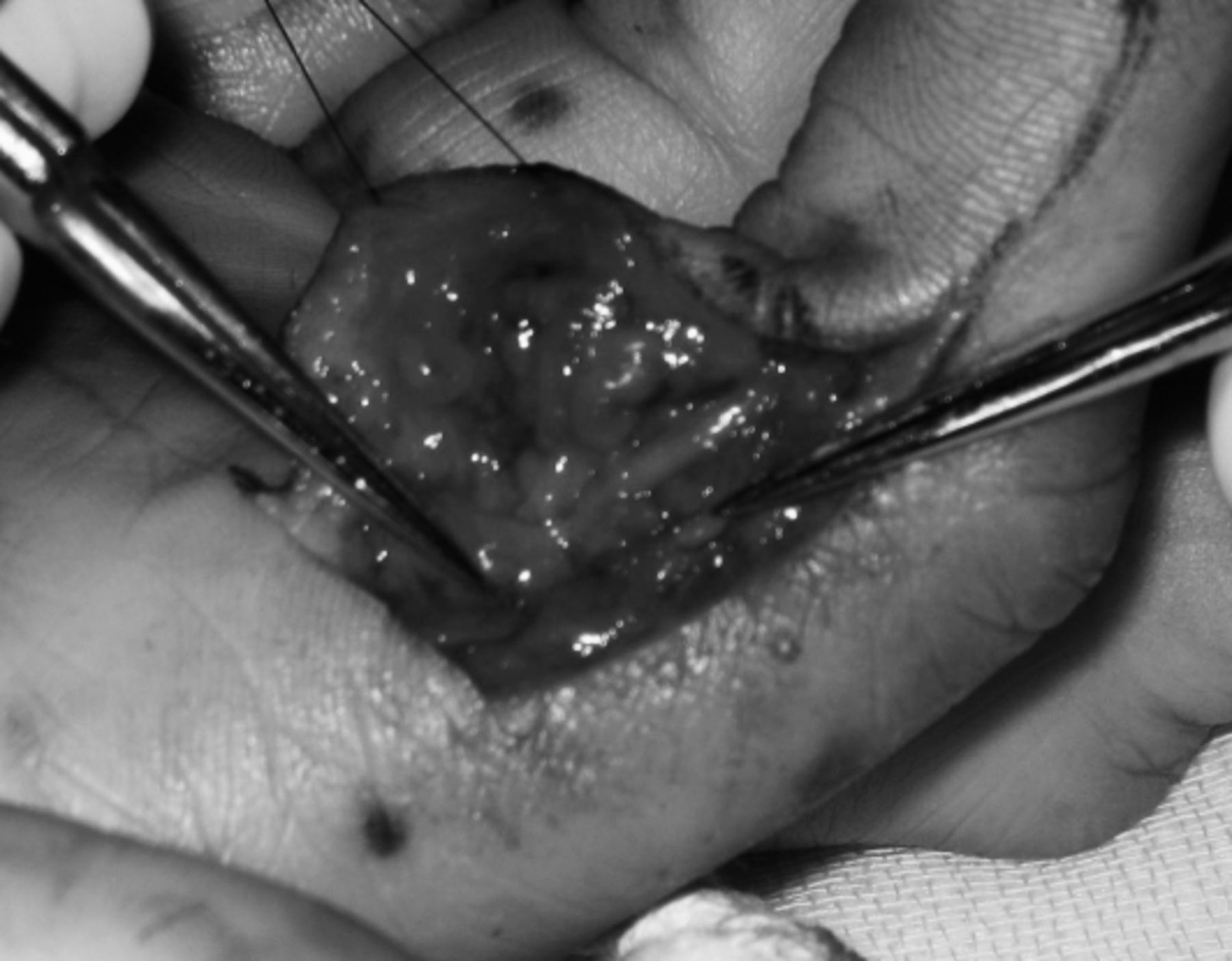
Intraoperatively avulsed radial digital artery.

Intraoperative perfused finger after digital artery repair.

Fluoroscopy view: Intraoperative index finger fixation with 2 K-wires (anteroposterior view).

Fluoroscopy view: Intraoperative index finger fixation with 2 K-wires (lateral view).
The index finger remained well perfused on discharge. At 5-month follow-up, the patient had a healed and fully neurovascularly intact index finger with good hand function.
LITERATURE REVIEW
A literature review of both Medline and PubMed isolated only 3 relevant publications: 2 case reports and 1 retrospective review.1-⇓3 Giddins and Burge1 first reported 3 closed digital artery injury cases, the first consistent with ring avulsion injuries and the latter 2 with crush injuries associated with impaired digital perfusion. Of the latter 2 cases, the first patient underwent surgical exploration and subsequent bilateral digital artery repair with good functional outcome at 3 months, whereas the second case involved bilateral fasciotomy only with resultant initially improved circulation but overall decreased hand function at 9 months. Faraj and Craigen2 reported a single case of a closed crush injury associated with digital ischemia that was surgically explored and required radial digital artery repair; no follow-up details were provided.
Reagan et al3 published the most recent and comprehensive review, with 2 new cases and 5 additional cases retrospectively identified during a 20-year period. All cases involved crush injuries and impaired digital perfusion. The first new case required surgical correction of digital artery tethering over a bone spike with good outcome at follow-up. The second new case was managed conservatively and progressed to necrosis, subsequently requiring partial digital amputation. The remaining cases were all treated surgically with either arterial repair of at least one digital vessel or alternatively a vein graft; all cases had a good functional outcome.
Diagnostically, Reagan et al3 described suggestive symptoms characteristic of closed digital artery injury: numbness, decreased sensation, cyanosis or pallor, and slowing of capillary filling. They proposed that nonsurgical management fails to resolve ischemia in closed digital artery injury and suggested surgical intervention for all closed digital artery injuries with secondary ischemia.
DISCUSSION
At present, only 10 documented cases of closed digital artery injuries can be identified, with our case making 11. Although uncommon, the occurrence of such cases warrants consideration with respect to several issues.
Reported cases thus far describe closed digital artery injury associated with secondary acute ischemia and therefore bilateral digital vessel involvement. However, it follows that unilateral injuries may occur at much higher rates without necessarily being diagnosed because of their asymptomatic nature. As such, literally taken, closed digital artery injury itself is a broader category, and all published cases could be more accurately classified as closed bilateral digital artery injury, as opposed to closed unilateral digital artery injury and rather than closed digital artery injuries per se.
A crush mechanism of injury can be attributed to all documented cases thus far. The most common fracture pattern involves a transverse phalangeal fracture in proximity to the interphalangeal joints. Avulsion of digital arteries in proximity to the associated fracture is the most common intraoperative finding, with primary arterial repair being the most common treatment. A sole case of digital artery tethering and an isolated case without fractures have, however, been described.
No strict criteria exist for digital ischemia, and the diagnosis is clinical, based on suggestive symptoms—pallor, coolness, capillary emptiness, and cyanosis. Our case had no indication for investigative confirmation; however, it has been suggested that Doppler, oximetry, and arteriography may be of value if the diagnosis is unclear.3
A closed digital artery injury with secondary acute ischemia requires urgent surgical intervention. Exploration and subsequent digital artery repair are most likely to be required in suspected ischemia. Failure to operate with the aim of restoring digital perfusion has been documented as causing necrosis or decreased hand function in 2 of the 11 cases detailed previously. Conversely, adequate surgical repair has been documented as restoring perfusion and normal hand function in the remaining 9 cases. Good surgical outcome (survival in 6 cases and good functional outcome in 3 others) is correlated with the restoration of perfusion regardless of whether bilateral or unilateral arterial repair is performed; bilateral repair was only performed in 2 of the 9 cases with good surgical outcome.
CONCLUSION
The rarity of closed digital artery injuries presents a diagnostic challenge that can easily be overlooked because of its unexpected presentation. A crush mechanism, with suggestive symptoms, and a transverse phalangeal (distal or proximal rather than mid-shaft) fracture should be alerting factors. It is commonplace to send all closed injuries to clinic the following day for assessment; however, a capable physician should assess all significant closed traumas to exclude an ischemic component. In uncertain circumstances, physicians should err on the side of caution, and urgent referral to a specialist center is warranted.
- Academic Division of Ochsner Clinic Foundation
In this issue








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.