
Abstract
Background Self-assessments of health are a strong predictor of mortality. Whether self-assessment of health provides additional information beyond a physician's assessment is unclear.
Methods We analyzed data on 14,530 US adults from the Third National Health and Nutrition Examination Survey. General self-rated health (GSRH)—“In general, would you say your health is Excellent, Very Good, Good, Fair, or Poor?”—and a single question to physician examiners following a medical examination rating participants' health, both on a 5-point scale of Excellent, Very Good, Good, Fair, or Poor were assessed for the period 1988-1994. All-cause mortality was assessed through December 31, 2006 (n = 3,460 deaths).
Results Agreement between participant GSRH and physician-assessed health was 53.8% (42.1% Excellent/Very Good, 8.7% Good, and 3.0% Fair/Poor; weighted Kappa statistic = 0.20). After adjustment, participants who reported better GSRH compared to the physician assessment of their health experienced lower mortality (hazard ratio = 0.76, 95% CI: 0.66-0.87). Also, participants reporting worse health than the physician assessment experienced higher mortality (hazard ratio = 1.45, 95% CI 1.24-1.70).
Conclusions Individuals who reported worse health than was assessed by a physician had increased mortality. These results warrant evaluation of whether GSRH collection in the clinical setting improves outcomes.
INTRODUCTION
Community-based cohorts and clinic-based studies show a strong association between participants' responses to a single question about general self-rated health (GSRH) and subsequent need for health expenditures and health services.1-3 Patient responses are also strongly associated with subsequent mortality even when adjusted for an array of covariates.4,5 GSRH has also been demonstrated to improve the predictive power of claims-based and clinical models.3
GSRH has not been widely used for predicting patient outcomes because practitioners have assumed that it adds little value over what an informed physician assessment and other relevant objective data can provide. Although one might believe that GSRH and physician assessment of health would be highly correlated, few studies have addressed this association. We hypothesized that GSRH may add value to physician assessments of health because many of the other important influences on health and outcome of which the patient is inherently conscious (socioeconomic status, emotional health, etc) are not routinely captured by either the health system or the physician. Therefore, we assessed the concordance between patient GSRH and physician assessment of health after adjustment for an array of objective data, as well as the risk for mortality associated with GSRH independent of physician-rated health in a nationally representative sample of US adults.
METHODS
Study Population
The Third National Health and Nutrition Examination Survey (NHANES III) is a stratified, multistage probability survey designed to select a representative sample of the civilian noninstitutionalized US population. Overall, 17,030 adults 20 years of age and older completed the NHANES III interview and examination from 1988 through 1994. We excluded 9 participants who were missing GSRH data, 989 participants missing data for physician assessments of their health, and 20 participants who did not have follow-up information. Additionally, 1,482 participants with missing covariate data were excluded. After these exclusions, we used a total of 14,530 NHANES III participants in the current analyses. The protocol for NHANES III was approved by the National Center for Health Statistics of the Centers for Disease Control and Prevention's Institutional Review Board. All participants gave informed consent. Details on the NHANES III can be found elsewhere.6
Baseline Data Collection
NHANES III baseline data were collected during an in-home interview and a subsequent visit to a mobile examination center where a study physician conducted a medical evaluation. The medical evaluation included a physical examination, anthropometric and blood pressure measurements, and blood and spot-urine collection. Height and weight were measured and body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared. During the in-home interview, researchers used a standardized questionnaire to collect sociodemographic, behavioral, and health-related information such as prior diagnoses and medications being taken. Blood pressure was measured 3 times during the in-home interview and 3 additional times during the visit to the mobile examination center. All blood pressure measurements for each participant were averaged for analysis.
Blood samples were stored at −20° C. Total and high-density lipoprotein (HDL) cholesterol was measured with the Hitachi 704 Analyzer (Roche, Basel, Switzerland). Serum C-reactive protein (CRP) was quantified using latex-enhanced nephelometry, a low sensitivity assay. CRP levels ≥3 mg/dL were considered elevated. Plasma glucose was measured using an enzymatic reaction. Diabetes mellitus was defined as a fasting plasma glucose ≥126 mg/dL, a nonfasting plasma glucose ≥200 mg/dL, and/or a self-reported history of diabetes with concurrent use of antidiabetes medication. Serum creatinine was measured by the Jaffe modified kinetic method. Glomerular filtration rate (GFR) was estimated using the Modification of Diet and Renal Disease equation after aligning the serum creatinine concentrations with the assay employed in the development of the equation.7,8 Urinary albumin was measured using a solid-phase fluorescence immunoassay; urinary creatinine was measured using modified kinetic method of Jaffe (Synchron AS/Astra Analyzer, Beckman Coulter, Brea, CA). Albuminuria was defined as a urinary albumin to urinary creatinine ratio ≥30 mg/g.
Physician-Assessed Health and Participant General Self-Rated Health
The main exposure of interest was the cross-classification of physician assessment of health and participant GSRH. During the in-home visit, participants were asked to respond to a single-item GSRH question: “In general, would you say your health is…” with five category response options of Excellent, Very Good, Good, Fair, or Poor. Also, following in-clinic examinations, study physicians estimated the overall health status of participants. The following guidance was provided to the physician: “Make an estimate of the overall health status of the examinee based on your findings from the physician's examination, regardless of the completeness of the examination. Select one of the following: ‘1. excellent,’ ‘2. very good,’ ‘3. good,’ ‘4. fair,’ or ‘5. poor.’ Only one number should be selected.” Physicians were not blinded to participants' GSRH assessed during the in-home interview.
Mortality Follow-Up
Mortality for the current analysis was assessed through December 31, 2006. The method of probabilistic matching was used to link NHANES III participants with the National Death Index to ascertain vital status and cause of death. Matching was based on 12 identifiers for each participant (eg, Social Security number, sex, date of birth). Identical matching methodology applied to the NHANES I Epidemiological Follow-up Study for validation purposes found that 96.1% of deceased participants and 99.4% of living participants were correctly classified.9 Further information on the matching methodology used to identify deaths is provided on the NHANES III web site: www.cdc.gov/nchs/data/datalinkage/matching_methodology_nhanes3_final.pdf.
Statistical Methods
After assessing the distribution of the GSRH and physician-assessed health of participants, we collapsed responses of Excellent and Very Good into 1 category and responses of Fair and Poor into 1 category, creating a 3-category GSRH variable for both participant- and physician-assessed health status. This provided an adequate number of outcomes in each GSRH and physician-assessed health strata to achieve stable point estimates for all analyses.
The distribution of participants by cross-classification of GSRH and physician-assessed health was determined. Overall agreement and a weighted kappa statistic were calculated. Participant characteristics were calculated by self-reported GSRH for each level of physician-assessed health. Trends across GSRH category were assessed using least squares for continuous variables and maximum likelihood for categorical variables.
For the analysis of all-cause mortality, follow-up for each study participant was calculated as the time between their NHANES III examination and the date of death or December 31, 2006, for those still alive at the end of follow-up. Cox proportional hazards regression was used to calculate the hazard ratios for mortality associated with Good and Fair/Poor versus Excellent/Very Good participant GSRH. An initial model included adjustment for age, race/ethnicity, and sex. The next model included additional adjustment for education, income, physical activity, cigarette smoking, BMI, systolic blood pressure, use of antihypertensive medications, total and HDL cholesterol, diabetes, estimated glomerular filtration rate, microalbuminuria, and elevated CRP. A final model included additional adjustment for physician-assessed health. Subgroup analyses assessed the multivariable-adjusted (including physician-assessed health) association between participant GSRH and mortality for participants <65 and ≥65 years of age and by race/ethnicity and sex. Next, for each level of physician-assessed health, the multivariable-adjusted hazard ratio for mortality associated with participant-reported GSRH was calculated. Lastly, hazard ratios for mortality were calculated for participants whose GSRH was better than (eg, the participant reported excellent/very good health and the physician assessed the participant to be in good health) and worse than (eg, the participant reported fair/poor health and the physician assessed the participant to be in good health) the physician-assessed health. Data were analyzed using SUDAAN (version 9.0; Research Triangle Institute, Research Triangle Park, NC) to account for the complex NHANES sampling design, including unequal probabilities of selection, oversampling, and nonresponse.
RESULTS
Overall, 52.2% of participants reported Excellent/Very Good GSRH, and 32.9% and 14.9% of participants reported Good and Fair/Poor GSRH, respectively (Table 1). Health was assessed by the physicians as being Excellent/Very Good, Good, and Fair/Poor for 70.9%, 22.2%, and 6.9% of participants, respectively. Overall participant GSRH and physician-assessed health were concordant for 53.8% of participants (42.1% Excellent/Very Good, 8.7% Good, and 3.0% Fair/Poor). The weighted kappa statistic for agreement between participant GSRH and physician-assessed health was 0.20.
Cross-Classification of Physician-Assessed Health by Participant-Reported General Self-Rated Health
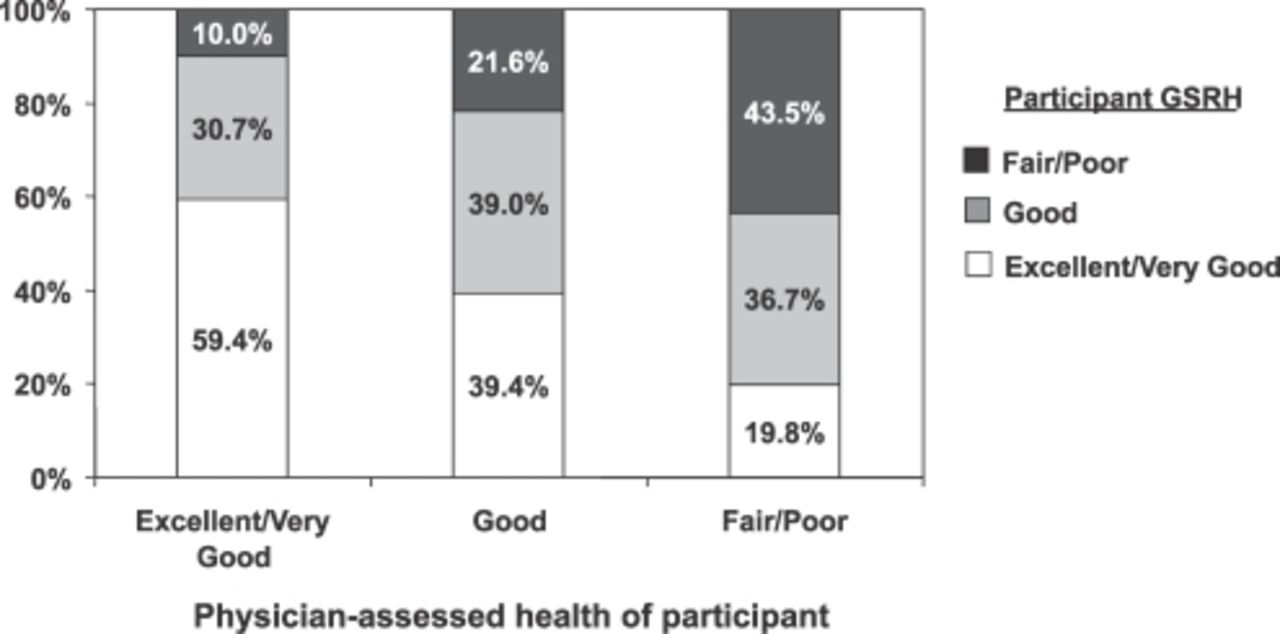
Among participants for whom their physician-assessed health was Excellent/Very Good, 59.4% reported Excellent/Very Good GSRH, while 30.7% and 10.0% reported Good and Fair/Poor GSRH (Figure). For participants whose physician-assessed health was Good, 39.4%, 39.0%, and 21.6% reported Excellent/Very Good, Good, and Fair/Poor GSRH, respectively. The distribution of participant GSRH was 19.8%, 36.7%, and 43.5% (Excellent/Very Good, Good, and Fair/Poor, respectively) among those whose health was assessed as being Fair/Poor by their physicians.
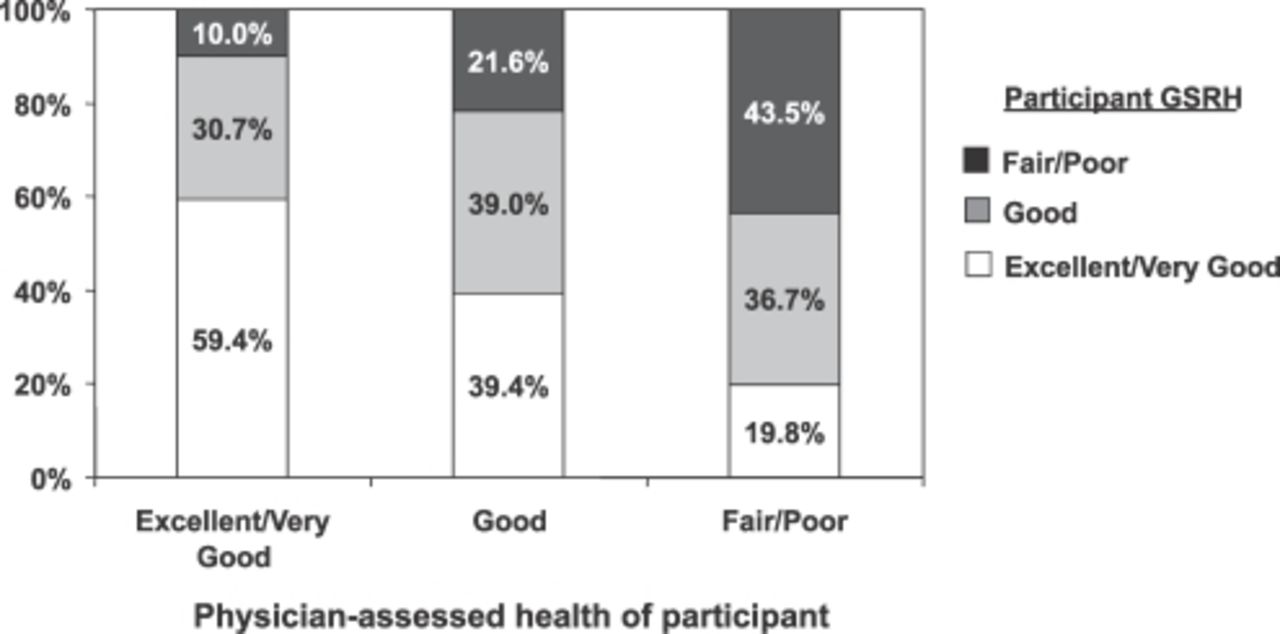
Distribution of participant general self-rated health (GSRH) by level of physician-assessed health.
Within each physician-assessed health grouping, participants with worse GSRH were older, more likely to be non-Hispanic blacks and Mexican-Americans, have less than a high school education, earn an annual household income <$20,000, and be physically inactive (Table 2). Worse GSRH was also associated with higher systolic blood pressure and diabetes.
Participant Characteristics by General Self-Rated Health Stratified by Physician-Assessed Health
Continued
Over a median of 13 years of follow-up (maximum follow-up: 18 years), 3,460 deaths occurred. The most common cause of death was cardiovascular disease (n = 1,512; 44%). Worse GSRH was associated with higher mortality rates before and after adjustment for an array of health conditions and physician-assessed health (Table 3). After multivariable adjustment, those with Good and Fair/Poor GSRH and physician-assessed health had 1.35 (95% CI: 1.18-1.55) and 1.74 (95% CI: 1.47-2.03) higher risk for mortality, respectively, compared to their peers whose GSRH was Excellent/Very Good. Patterns of increased hazard ratios for mortality associated with worse GSRH were present across subgroups defined by age, race/ethnicity, and sex as shown in Table 4. Within each physician-assessed health category, worse participant GSRH was associated with a significantly higher multivariable adjusted hazard ratio for mortality (Table 5). Results were consistent for the outcome of cardiovascular mortality (Table 6).
All-Cause Mortality Rates and Hazard Ratios for Mortality by Participant-Reported General Self-Rated Health
All-Cause Mortality Rates and Hazard Ratios for Mortality by Participant-Reported General Self-Rated Health in Subgroups Defined by Age, Race/Ethnicity, and Sex
Adjusted Hazard Ratio for All-Cause Mortality Associated With Participant-Reported General Self-Rated Health Stratified by Physician-Assessed Health
Adjusted Hazard Ratio for Cardiovascular Disease Mortality Associated With Participant-Reported General Self-Rated Health Stratified by Physician-Assessed Health
Following multivariable adjustment for age, race, sex, education, income, current and former cigarette smoking, BMI, systolic blood pressure, use of antihypertensive medications, total and HDL cholesterol, diabetes, estimated glomerular filtration rate, microalbuminuria, and elevated CRP, participants who reported better GSRH than the physician assessment of their health experienced lower mortality (hazard ratio = 0.76, 95% CI: 0.66-0.87). Also, participants reporting worse health than the physician assessment of their health experienced higher mortality (hazard ratio = 1.45, 95% CI 1.24-1.70).
DISCUSSION
In this analysis of a nationally representative sample of US adults, participant GSRH and physician perceptions of general health were not highly correlated. Participants with worse self-rated health had a significantly higher risk for mortality even after adjusting for physician perception of their health and an array of objective health data. This relationship was present in the overall population and was markedly consistent across age, race/ethnicity, and sex subgroups. Also, participants with self-assessed health worse than that rated by the study physicians experienced significantly higher mortality. These data suggest that GSRH provides important patient-centered information in addition to that readily available to clinicians.
The low level of concordance between GSRH and physician assessments of health observed in the current study is consistent with prior literature. Furthermore, physician-assessed health and GSRH may not always be concordant, especially if physicians do not consider nonclinical psychosocial information such as quality of life, income, and education.10,11 In a group of older patients, Finnish investigators reported significant discordance between individuals' self reports of health and their physicians' assessment.10 Also, in a study of 456 patients attending a primary care clinic, discordance between physician assessment of an individual's health and self-rated health was present in 32% of the patients.11 In a separate study of participants recruited in a primary care setting, overall agreement between patients' reports of their health and objective measures was only 54%.12 The current results are consistent with these previous findings; overall agreement and the agreement beyond that expected by chance (ie, kappa statistic) were low.
Reasons for the discordance between self-rated and physician-assessed health are not entirely clear. Patients with depression, advancing age, and lower socioeconomic status are more likely to have discordance with their physician assessments.10,13 Because patients capture a broad array of dimensions when assessing their own health that may not be incorporated into physician-assessed health, the rates of discordance are not surprising.14,15 Patients inherently know their past medical history, current symptoms (such as masked depression), social circumstances, and family longevity. All can contribute to mortality and can be easily missed by a physician assessment. Even when stratified by physician-assessed health, characteristics of participants in the current study varied widely by GSRH.
Prior studies have reported worse GSRH to be associated with increased mortality even after controlling for objective measurements of health, such as claims-based measures of chronic diseases.3,16-18 In one study, participants who rated their health as being better than expected based on the presence of chronic diseases had improved health outcomes. In contrast, those who reported worse health than expected based on the presence of chronic diseases (termed realists or pessimists) had higher rates of adverse outcomes.12 Although studies have documented that GSRH provides additional information above and beyond objective health information, few data are available on the additional information provided through self-rated versus physician-assessed health.
The added value of GSRH to physician assessments plus clinical data is expected given the broad array of dimensions captured in patients' general health assessments that are potentially not known to the clinician and not routinely part of what is collected in administrative and clinical databases. GSRH is a summative measure accounting for a variety of personal and relevant social characteristics. When considering their own health, individuals are known to consider their overall physical, mental, and social situation.19,20 GSRH is also highly correlated with a number of biomarkers that are associated with morbidity and mortality.21,22
Creating a more patient-centered health system will require systematizing patient perspectives on their health and healthcare. A single question assessing a patient's GSRH performs well in predicting future health states and needs. Because GSRH information takes only seconds to collect, it may be valuable to add to the routine data collected from patients to aid in predictive modeling. Collecting the answer to a single GSRH question could easily be added to routine intake information at primary care appointments for use by administrators. The information could be easily merged with patient age, sex, and race/ethnicity and could be useful for predictive modeling by payers and health system managers. GSRH responses add important information to administrative data for the prediction of future healthcare expenditures.3 Also, adding GSRH to the Framingham Risk Score improves prediction of future coronary heart disease incidence.23 In addition to the administrative value of adding GSRH to prediction models, the information captured through the collection of GSRH answers may prove valuable in guiding the patient into care management programs at the point of care. If GSRH information is collected in an automated fashion in an electronic health record, patients with poor or declining GSRH can be further evaluated for care management, even in the absence of physician referral. Given the discordance seen between patient and physician assessments of health and the significant impact patient GSRH has on outcomes when patients report worse health than their physicians assess, the use of GSRH could dramatically improve the identification of high-risk patients and earlier entry into beneficial care programs.
The findings from the present study should be considered in the context of potential limitations. GSRH is a subjective measure that can vary in response to significant life events whether physical or mental. However, it is a generally reliable measure and at the population level, sufficiently stable.24,25 Although the physician assessments were performed in a rigorous manner consistent with the NHANES protocol, the study physicians were handicapped by a lack of continuity relationship with participants. This limits the inclusion of a longitudinal perspective on participants' health when providing an assessment. Despite these limitations, the current study has many strengths. Most notably, NHANES III data were collected using a rigorous study protocol with extensive quality control procedures. The extensive data collection in NHANES III allowed adjustment for many objective measures of health (eg, the presence of hypertension, diabetes, albuminuria, inflammation, etc). The strong association between GSRH and all-cause mortality after controlling for these factors is noteworthy. Also, the results are representative of the US noninstitutionalized civilian population.
CONCLUSION
In this large nationally representative sample of US adults, GSRH and physician assessments of health maintained low agreement. Furthermore, regardless of physician rating of a participant's health, self-assessed health via GSRH maintained a strong, graded association with mortality. These results suggest that important prognostic information is contained in an individual's GSRH assessment beyond other objective data and physician impression of health. Routinely collecting GSRH may enhance the focus on patient-centered care.
This article meets the Accreditation Council for Graduate Medical Education competencies for Patient Care, Medical Knowledge, and Systems-Based Practice.
- Academic Division of Ochsner Clinic Foundation








{kind=link}