
Abstract
A fibrolipomatous hamartoma—also known as a fibrofatty overgrowth, perineural lipoma, intraneural lipoma, and lipomatous hamartoma—is a rare, benign, congenital lesion most commonly found in the median nerve, usually at the level of the wrist or hand. To our knowledge, no published cases report a hamartoma arising from the median nerve at the level of the elbow. We report a case of a fibrolipomatous hamartoma in a 55-year-old woman that necessitated a surgical intervention because of its size and associated neurologic symptoms.
INTRODUCTION
A fibrolipomatous hamartoma of the median nerve is a rare, benign lesion first reported in 1953.1 Also known as a fibrofatty overgrowth, perineural lipoma, intraneural lipoma, and lipomatous hamartoma,1-3 a fibrolipomatous hamartoma is usually unilateral and has no known genetic component. Although it can present in childhood and early adulthood, it is believed to be of congenital origin.4
While most commonly found in the median nerve, studies have reported the lesion at other sites such as the radial, ulnar, sciatic, and plantar nerves5-7 and in the lungs.8 When found in the median nerve, the lesion is usually at the level of the wrist or hand. To our knowledge, no published cases have involved a fibrolipomatous hamartoma arising from the median nerve at the level of the elbow.
CASE REPORT
A 55-year-old woman presented with a 4-year history of medial right elbow swelling that was gradually increasing in size. This swelling was associated with tingling sensations in her right thumb. The lesion was smooth but tender and surrounded the origin of the forearm flexor musculature. No associated skin changes were present. Neurologic examination revealed altered sensation in the distribution of the median nerve. The remainder of the physical examination was unremarkable.
The ultrasound scans organized by her general practitioner at 1 and 3 years prior to her presentation revealed prominent brachialis musculature as being responsible for the mass. A magnetic resonance imaging (MRI) scan showed a 12 × 4.5 × 4.0 cm lesion surrounding the median nerve within the distal arm and proximal forearm (Figure 1). The appearance was that of a lipoma, and the orientation of the lesion suggested a perineural origin.

Coronal section. T1-weighted magnetic resonance image showing the fibrolipomatous hamartoma at the proximal forearm (arrow).
We performed an excisional biopsy under general anesthesia via a longitudinal incision in the elbow. The median nerve was identified proximally and traced distally. The lesion was well circumscribed, consisted of fatty tissue, and was intimately associated with the median nerve and its muscular branches in the proximal forearm. We carefully dissected the lesion, leaving the major branches of the nerve intact.
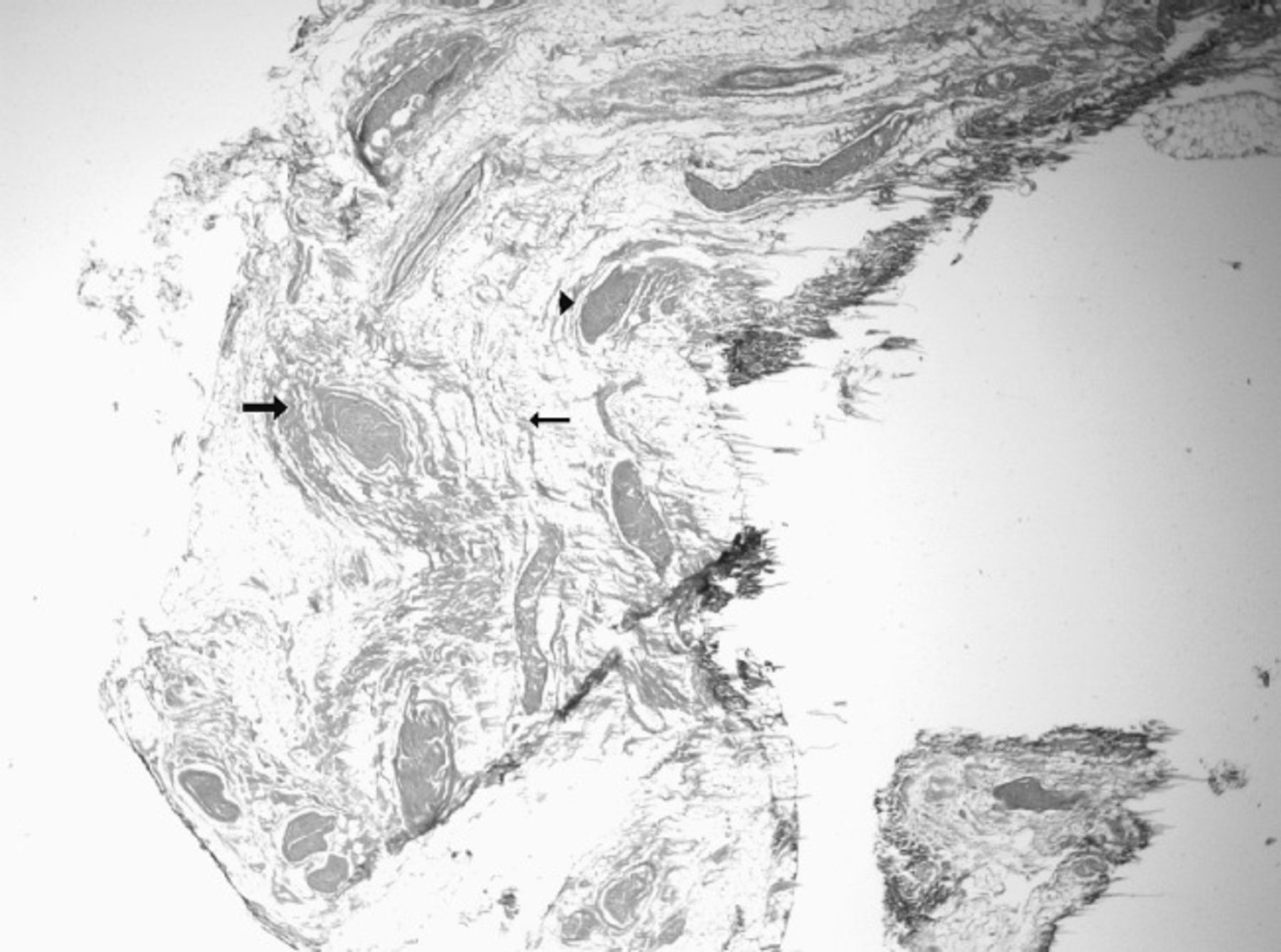
Macroscopically, the lesion had a homogenous fatty appearance. Microscopic examination revealed mature fibroadipose tissue that incorporated and separated small fascicles of the peripheral nerve. We also saw concentric perineural fibrous tissue around individual nerve bundles (Figure 2).

Histology of the lesion showing perineural infiltration of fibroadipose tissue separating nerve bundles (thin arrow), concentric fibrous tissue around the perineurium (thick arrow), and widely separated small bundles of nerves (arrowhead). The nerve bundles contain myelinated peripheral nerve fibers (axons) with their accompanying Schwann cells and some nonmyelinated nerve fibers (axons) (magnification ×16, hematoxylin-eosin stain).
The patient had an uneventful postoperative recovery with resolution of her neurologic symptoms. Her 12-month follow-up showed no clinical evidence of recurrence.
DISCUSSION
Fibrolipomatous hamartoma of the median nerve has been reported to be associated with macrodactyly and port-wine stain.9,10 Its natural history is a gradual increase in the size of the lesion along with symptoms of compressive neuropathy.11 These symptoms are not thought to be caused by the intraneural involvement of the tumor,12 but to be dependent on the level and the nerve from which the tumor arises. When the median nerve is involved, patients may present with carpal tunnel syndrome or a slow-growing painless lump in the wrist or hand.
The gold standard for investigation is MRI. The pathognomonic appearance is that of low signal nerve bundles surrounded by high signal fibrolipomatous tissue on T1-weighted images, also called the cable sign.13 No other tumors have been found to have similar MRI characteristics.14
Management of fibrolipomatous hamartomas can be conservative or surgical. Because MRI is often diagnostic, biopsy is often not needed to establish the diagnosis.14 Surgical intervention is controversial and is only recommended for symptomatic management of this benign lesion.13 Documented management has been restricted to fibrolipomatous hamartomas arising from the wrist or fingers: carpal tunnel decompression, fibrofatty sheath debulking, microsurgical dissection of the neural elements, and excision of the involved nerve with or without grafting.
The options are more limited in the elbow because excision of the median nerve at the elbow is associated with high morbidity and is not recommended. The main surgical options are debulking the fibrofatty sheath or microsurgically dissecting the neural elements. We used the latter option and achieved a good outcome.
CONCLUSIONS
Fibrolipomatous hamartoma is a benign condition that does not become symptomatic until it has been present for many years. Its symptomatology stems from compression of the nerve rather than intraneural involvement by the tumor. Intervention is only necessary when the patient is symptomatic. Although surgery is controversial in areas where excision is associated with a high morbidity and decompression is not possible, careful microsurgical dissection of the neural elements can achieve good results.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care and Medical Knowledge.
Footnotes
The authors have no financial or proprietary interest in the subject matter of this article.
- Academic Division of Ochsner Clinic Foundation
In this issue








{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.