
Abstract
Intracranial hemorrhage (ICH) in full-term neonates with hemophilia is uncommon. Retrospective studies estimate the incidence to be 3.4%-4.0%. However, ICH is the second most common initial hemorrhage for all infants with congenital hemophilia. Nearly half (41%) of the hemorrhages occur within the first week of life, and most hemorrhages are related to traumatic deliveries. But clinical signs of ICH in neonates are difficult to assess and often result in a delay in the diagnosis. The timely diagnosis of ICH is critical; however, the early and intensive factor replacement therapy that the patient needs is associated with the risk of inhibitor formation. We report a case of ICH in a neonate with severe hemophilia A, no family history, and inhibitor development after intensive therapy.
INTRODUCTION
Intracranial hemorrhage (ICH) is the abnormal accumulation of blood in the cranial vault that may occur within the brain parenchyma or in the surrounding meningeal spaces.1 ICH is the second most common initial hemorrhage for all neonates with congenital hemophilia,2,3 and its incidence is 40-80 times higher than in neonates without hemophilia. Nearly half (41%) of these hemorrhages occur within the first week of life. Most (81%) are related to traumatic deliveries and the use of fetal scalp monitors, forceps, or vacuum extraction.3-5 ICH is the most feared complication of hemophilia; 20% of infants with ICH die. Timely diagnosis and prompt initiation of therapy with ICH are critical, even though the clinical signs of ICH in neonates are difficult to assess.
Retrospective studies estimate the incidence of intracranial hemorrhage in neonates with hemophilia to be 3.4%-4.0%.4 The anatomical classifications of ICH include epidural and subdural hematomas, subarachnoid hemorrhages, intracerebral hemorrhages, and intraventricular hemorrhages.6-8 Bleeding disorders account for a small number of ICH cases.9,10
A patient experiencing ICH has several mechanisms of brain injury: primary direct mechanical injury as an evolving clot grows, increasing intracranial pressure with associated edema within the fixed intracranial space, decreased blood flow to the local area of the clot that causes neuronal ischemia, and cerebral herniation secondary to edema and mass effect.10,11
Data indicate the incidence of ICH in all patients with congenital hemophilia ranges from 3-12%, and an estimated 5-10% of people with severe hemophilia will have >1 ICH in their lifetime.12 Patients with inhibitors, young patients <10 years of age, and patients who experience head trauma are at significant risk for the development of ICH. However, the early and intensive factor replacement therapy needed to treat ICH is associated with the risk of inhibitor formation.13
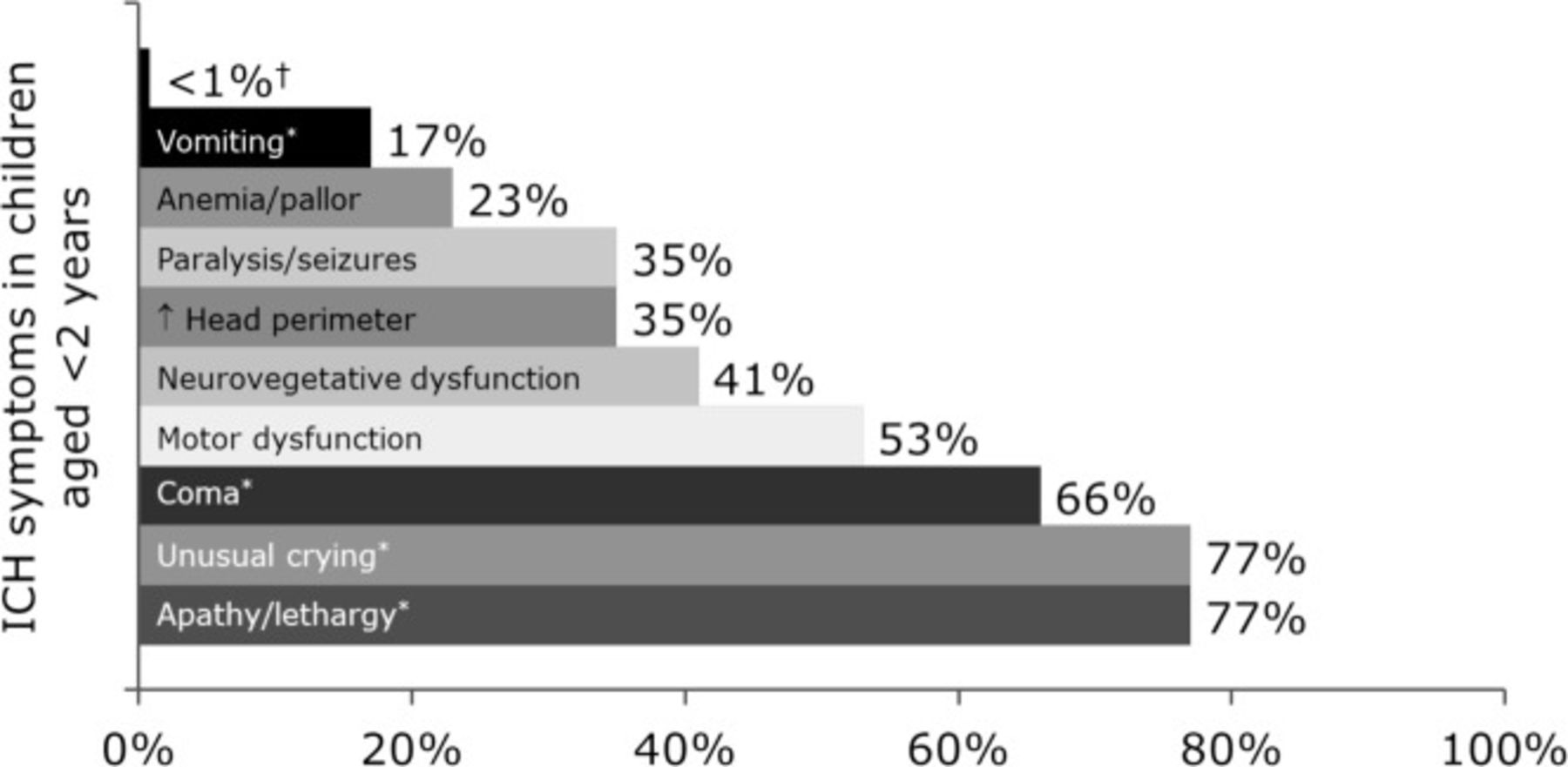
Even with knowledge of the risks, the early recognition of the clinical signs of ICH in at-risk neonates presents a significant challenge.14 The initial clinical presentation of ICH in neonates is often subtle and similar to that in many other conditions, including disseminated intravascular coagulopathy, meningitis, and sepsis. Anemia, lethargy, hypotension, and shock are also common findings in intracranial and extracranial bleeds. Seizures, bulging fontanels, and neurologic sequelae are more common in ICH.2,14 However, the most frequently first documented symptoms among children ages <2 years (Figure 1) are often nonspecific. However, a failure to diagnose ICH and a delay in the delivery of factor replacement therapy are associated with increased morbidity and mortality.

Possible clinical signs in neonates with intracranial hemorrhage (ICH).
†Hypotension, tense fontanelle, pupillary/ocular changes, and apnea.
*The most frequent first documented symptoms among children aged <2 years; often nonspecific.
We report a case of one neonate with ICH that involved diagnostic and therapeutic challenges.
CASE REPORT
A male infant experienced a normal spontaneous delivery at a rural community hospital at 40.5 weeks of gestation. On his first day of life, he had a prolonged hemorrhage after a circumcision. The excessive bleeding was treated with suture placement and aminocaproic acid. The bleeding episode prompted an evaluation for hemophilia that revealed Factor VIII activity of 0.6%. Following discharge, the diagnosis was confirmed by a pediatric hematologist located 4 hours from the patient's home. A local pediatric hematologist followed the infant's care after he went home. He was seen in the clinic shortly before 4 weeks of age because his mother reported that the baby had been “incredibly fussy” for 3 days and had “felt hot” for 2 days. The mother had not taken his temperature.
At 4 weeks of age, the infant was taken to the local emergency department (ED) with irritability and a temperature of 102.2°F. In the ED, he received 269 units of intravenous recombinant antihemophilic factor concentrate. Shortly thereafter, cerebrospinal fluid from a lumbar puncture was pink. A computed tomography (CT) scan of the brain subsequently revealed a subdural hematoma versus a subarachnoid hemorrhage of the right posterior fossa.
The ED physician contacted the state hemophilia treatment center and arranged transfer there. The hemophilia treatment center team assessed the patient in the pediatric intensive care unit.
The review of systems was significant for irritability and fever. The baby's past medical history was significant for hemophilia A but was otherwise negative. He was not taking any medicines and was not known to have any drug allergies. His previous surgical history was significant only for the circumcision. His mother and father noted that he was their first baby, and they denied any family history of hemophilia. His mother and maternal uncle had a history of spina bifida, but the family history was otherwise unremarkable. Additionally, the baby had been previously started on Nutramigen formula (Mead Johnson, Glenview, IL) with oatmeal because of clinical reflux.
On physical examination, his vital signs were temperature 99.7°F, pulse 158 beats per minute, respiratory rate 29 breaths per minute, blood pressure 90/41 mmHg, O2 saturation 100% on room air, and weight 9.9 lbs. He appeared irritable and had a grade 2/6 systolic ejection murmur. His anterior fontanelle was noted as normal, and the remainder of the physical examination was unremarkable.
Based on laboratory results from the ED and the hemophilia center (Tables 1 and 2), he had Factor VIII activity of 54.8%. He was then given a 25 unit/kg bolus of recombinant antihemophilic Factor VIII concentrate (50% correction) and started on a continuous infusion of recombinant antihemophilic Factor VIII concentrate with target Factor VIII activity of 80%-100%. He also received ampicillin 400 mg/kg/d divided every 6 hours and cefotaxime 200 mg/kg/d divided every 6 hours intravenously secondary to the history of fever. A repeat CT scan and magnetic resonance imaging (MRI) of the brain revealed a right cerebellar subdural hematoma, bilateral cerebellar superficial parenchymal hemorrhage, and foramen magnum hemorrhage (Figure 2).

T1-weighted axial magnetic resonance image of the brain, indicating a right cerebellar subdural hematoma, bilateral superficial cerebellar parenchymal hemorrhage, and foramen magnum hemorrhage.
Patient Laboratory Results on Presentation
Results From the Lumbar Puncture on Presentation
The infant remained stable and was discharged from the pediatric intensive care unit after a 4-day stay. He was transferred to the pediatric inpatient unit, where he continued his recombinant antihemophilic Factor VIII concentrate infusion for a total of 10 days. His irritability resolved, he was tracking visually and smiling, and his physical examination remained unremarkable. A follow-up CT scan revealed a stable hemorrhage with no increase in size. During his hospital course, a central line was placed without complication to facilitate the delivery of factor concentrate therapy in the hospital and to allow delivery at home following discharge. Four days prior to discharge, he was weaned to replacement every 12 hours with recombinant antihemophilic Factor VIII concentrate 50 units/kg for 14 additional days. Upon completion of the infusions, the treatment plan incorporated once daily doses of 50 units/kg. He then began prophylaxis 3 times weekly on Monday, Wednesday, and Friday with 30 units/kg.
After his 15-day hospital stay, he completed the remainder of the infusions with his new central line at home with the assistance of home healthcare providers. When he presented to a comprehensive hemophilia clinic for reevaluation the week following discharge, his parents reported that the twice-a-day infusions were going well, and they denied any problems or concerns.
Unfortunately, although the infant was doing well clinically, he was noted to have a positive inhibitor titer of 1 BU. His recombinant antihemophilic Factor VIII concentrate continued and was complete after 2 months, and the transition to prophylaxis occurred as planned. He was also scheduled to see the hemophilia treatment team once a week for follow-up for 4 to 6 weeks because of the increased risk of recurrent intracranial hemorrhage with the history of ICH and the development of a new inhibitor to exogenous Factor VIII.
The development of inhibitors in this setting is a well-known risk and presents a significant challenge in the future management and follow-up of this neonate. He will continue to receive prophylaxis 3 times a week with recombinant antihemophilic Factor VIII. For the next 6 months, he will be evaluated for abnormal findings associated with recurrent ICH, such as changes in activity level, lethargy, unusual crying, vomiting, nausea or changes in feeding, changes in affect, motor dysfunction, anemia/pallor, or seizures. During these monthly visits, he will be screened for abnormal bleeding while on prophylaxis, and blood samples for inhibitor titers will be followed to determine if additional intervention with bypassing agents is necessary. In the long term, he will undergo annual neuropsychiatric, speech, hearing, and vision evaluations to evaluate for subtle expressive language deficits, executive function deficits, attention deficit and hyperactivity disorder, specific learning disabilities, depression, and anxiety.
The appropriate management of an infant with a suspected ICH is to treat early and treat first with factor replacement therapy prior to any radiologic investigations, laboratory studies, or other procedures. When infants and other patients with hemophilia and suspected ICH present to the ED, factor replacement therapy is often not provided up front. The infant in this report has experienced an excellent outcome to date, likely in large part because of the prompt initiation of factor replacement therapy upon his arrival at the ED with irritability, a symptom that could be considered vague but certainly can be found in patients with ICH.
DISCUSSION
Although ICH is associated with increased morbidity and mortality, delayed diagnosis occurs for a variety of reasons, including vague symptoms—such as the irritability and fever in this case—that may be confused with other conditions or a lack of awareness that the baby has congenital hemophilia.2 ICH may be the first indication that a neonate has congenital hemophilia.15 As few as 23% of full-term and 3% of preterm newborns with documented ICH are evaluated by neonatologists for congenital hemophilia, and neonates with congenital hemophilia are almost never diagnosed prenatally. The incidence of congenital hemophilia in newborns who die at birth or in utero from ICH is not known.15
Prior to 1960, the mortality rate of people under 30 years of age with congenital hemophilia A and B was approximately 70%, and ICH accounted for approximately 31% of all deaths.16,17 Before the availability of Factor VIII and Factor IX concentrates in the 1960s, the mean age of death from ICH in this population was 23 years.18 The outcomes of people with hemophilia who experienced an ICH improved significantly in the 1970s because of the introduction of more sophisticated imaging modalities, such as CT and MRI.10 With the regular use of factor concentrates and prophylaxis (the use of infusions on a schedule to prevent bleeding), the mortality rates for ICH declined but remain a considerable challenge (20%-30%).10,14,19,20 Additionally, the risks of neurologic sequelae are substantial.9,21 Common neurologic sequelae include seizures (63% of cases), psychomotor (59%) and statomotor retardation (52%), and cerebral palsy (45%).22
In addition to serious neurologic sequelae, neonates with congenital hemophilia and ICH may also have subtle, long-term quality-of-life and neuropsychiatric problems. Studies report that boys with congenital hemophilia who experienced ICH are significantly more likely to have neurocognitive, academic, behavioral, adaptive, and motor functioning deficiencies.23 These findings strongly suggest that long-term follow-up of children with ICH, including neuropsychological assessment and intervention, is critical.24
The timely diagnosis and treatment of ICH are critical, but the early and intensive factor replacement therapy is associated with the risk of inhibitor formation, as demonstrated with our patient.13 Once a patient with severe hemophilia develops an inhibitor, the management of ICH requires additional and more intensive intervention that may include neurosurgical consultation (when appropriate), hemostatic therapy with bypassing agents, monitoring via imaging, and supportive physical, speech, or occupational therapy.
Previous studies have observed that hemophilia patients with inhibitors should be treated with bypassing agents immediately at symptom presentation and continue at full dose after an ICH episode.10,25,26 The duration of therapy, including posthemostatic dosing, continues to be an area of ongoing interest; the clinician determines duration. Because of ICH's elevated risks and high mortality rate, it is a true medical emergency and should be treated presumptively prior to any evaluation.
Knowing the diagnosis, the specific severity of disease (mild >5% circulating factor, moderate 1%-5%, or severe <1%), and the history of inhibitors or anaphylaxis is necessary to provide appropriate care.
CONCLUSIONS
Even the subtle signs associated with ICH should trigger the suspicion of an episode, and treatment should be given preemptively. In any case of suspected ICH in neonates or children with hemophilia, contact with a regional hemophilia treatment center immediately or prior to discharge from the ED or the hospital can be lifesaving. ICH should be managed in an experienced center; however, treatment should not be delayed until after transfer to the treatment center. Surgical intervention may be necessary, and the pediatric neurosurgical service should be notified. Finally, comprehensive rehabilitation and close long-term follow-up with the hemophilia treatment center are essential to an optimal recovery.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care and Medical Knowledge.
Footnotes
The authors have no financial or proprietary interest in the subject matter of this article.
- Academic Division of Ochsner Clinic Foundation
REFERENCES
In this issue








{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.