
Abstract
Background Through efforts to continuously improve the quality of care provided to hospitalized patients with diabetes by evaluation of adherence to standards and performance metrics, we identified an opportunity for improvement.
Methods A plan-do-study-act cycle was initiated with the goal of enhancing patient satisfaction with the timing of blood glucose monitoring, insulin administration, and meal delivery in the hospital.
Results Despite an educational intervention with the nursing staff, patient satisfaction with mealtime insulin administration decreased from 83% to 78%.
Conclusion Education of frontline staff was not adequate to achieve our quality improvement goal.
INTRODUCTION
A strong and growing body of evidence links high patient satisfaction and enhanced patient/family experience of inpatient hospital care to improved health outcomes.1 Improved patient experience leads to better management of chronic illnesses such as diabetes. The Joint Commission expects organizations to develop a comprehensive approach to performance improvement, to evaluate patients' perceptions of quality of care, and to use comparative data to review interventions. To maintain the Ochsner Medical Center–New Orleans (OMC) disease-specific certification by The Joint Commission in Inpatient Diabetes Care, a multidisciplinary team focuses on performance improvement related to the care of patients with diabetes. Patient satisfaction is one of the major performance metrics for the diabetes program. The diabetes program at OMC monitors patient satisfaction with patient experience surveys.
OMC is a 473-bed, tertiary acute care hospital with multiple bedded units taking care of patients with diabetes. A national vendor sends patient satisfaction surveys to hospital patients, but these surveys are not specific to patients with diabetes. Therefore, they cannot adequately provide actionable items for improvement specifically related to diabetes care. Moreover, the satisfaction surveys from the national vendor are sent via mail to patients after discharge from the hospital, requiring former patients to recall their treatment after the fact and to take the initiative to return the survey in the mail.
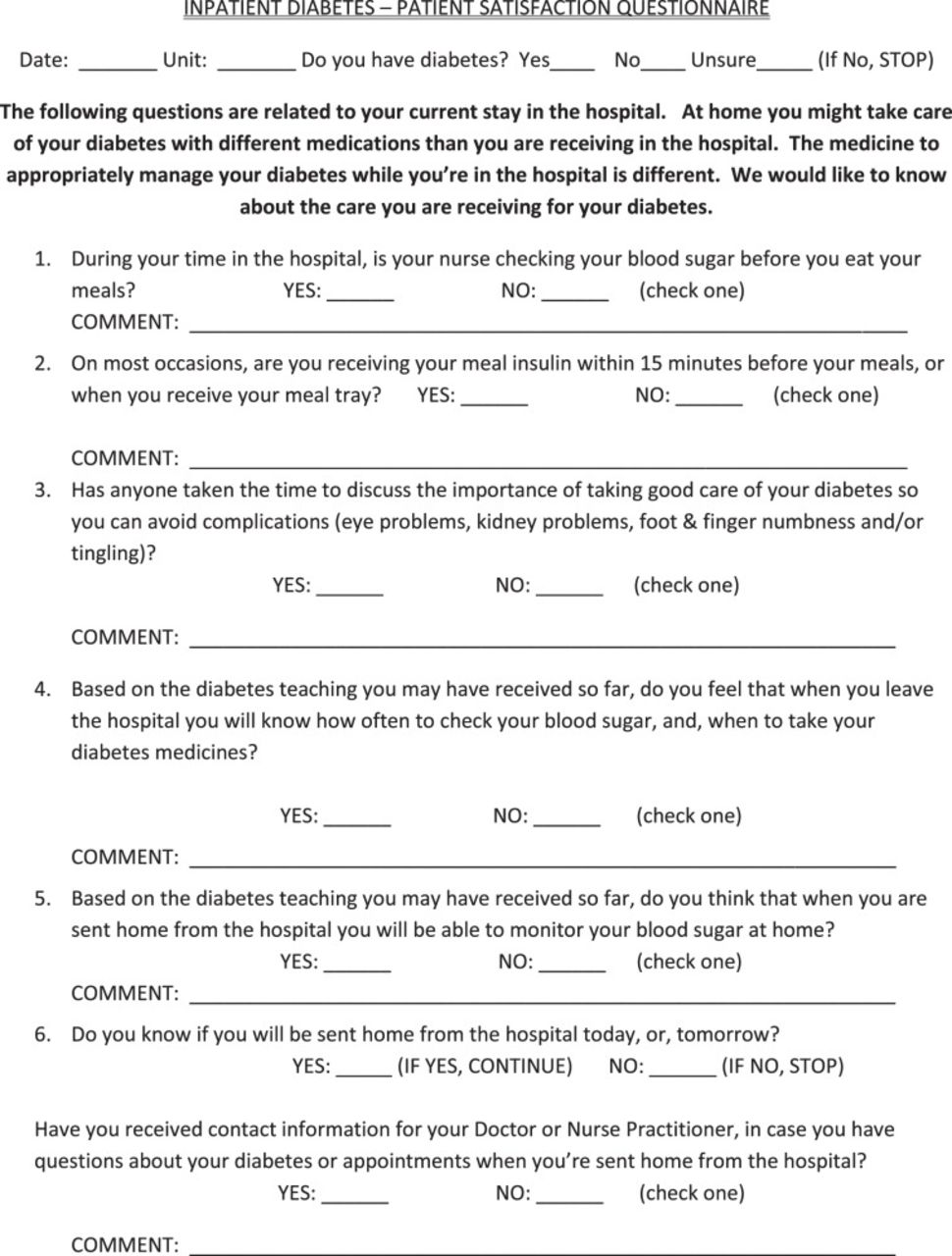
Consequently, a multidisciplinary team at OMC developed an inpatient diabetes patient satisfaction questionnaire to more specifically assess the care provided to patients with diabetes before they leave the hospital (Figure 1). This survey tool is used to identify the success of inpatient diabetes care, as well as to focus on areas to improve quality of care and adherence to best-practice standards. It is a means of self-assessment and performance review, two important factors identified by The Joint Commission.

Inpatient Diabetes Patient Satisfaction Questionnaire.
METHODS
The OMC patient satisfaction survey tool included 6 yes or no questions with space available to elaborate. The surveyors were dietary personnel, a student volunteer, and the diabetes program clinical coordinator. Patients were screened based on dietary lists taken from the hospital's electronic health record and were included in the survey population if they were placed on a diabetic diet, carbohydrate restriction, and/or daily caloric intake of 1,800, 2,000, or 2,200 kCal. Patients from 7 to 10 units were represented in the surveys monthly. Selected patients were visited in their rooms, and the surveyor read each question word for word. Only patients who responded yes to having diabetes were asked to complete the survey. If the patient were unsure of his or her diabetes status, the survey was discontinued. Up to 10 patients from each inpatient unit were surveyed each month. Multiple units were surveyed, but the intervention was conducted on 1 unit only. Data collected were entered into a spreadsheet configured so yes and no responses received scores; additionally, the spreadsheet provided a satisfaction score per patient. Each month the patient satisfaction results, per unit, were averaged to provide an overall percentage of satisfaction of diabetes care both per unit and overall. The scores for each question were averaged to indicate focus areas for improvement. The target for patient satisfaction addressed by each question is >90%.
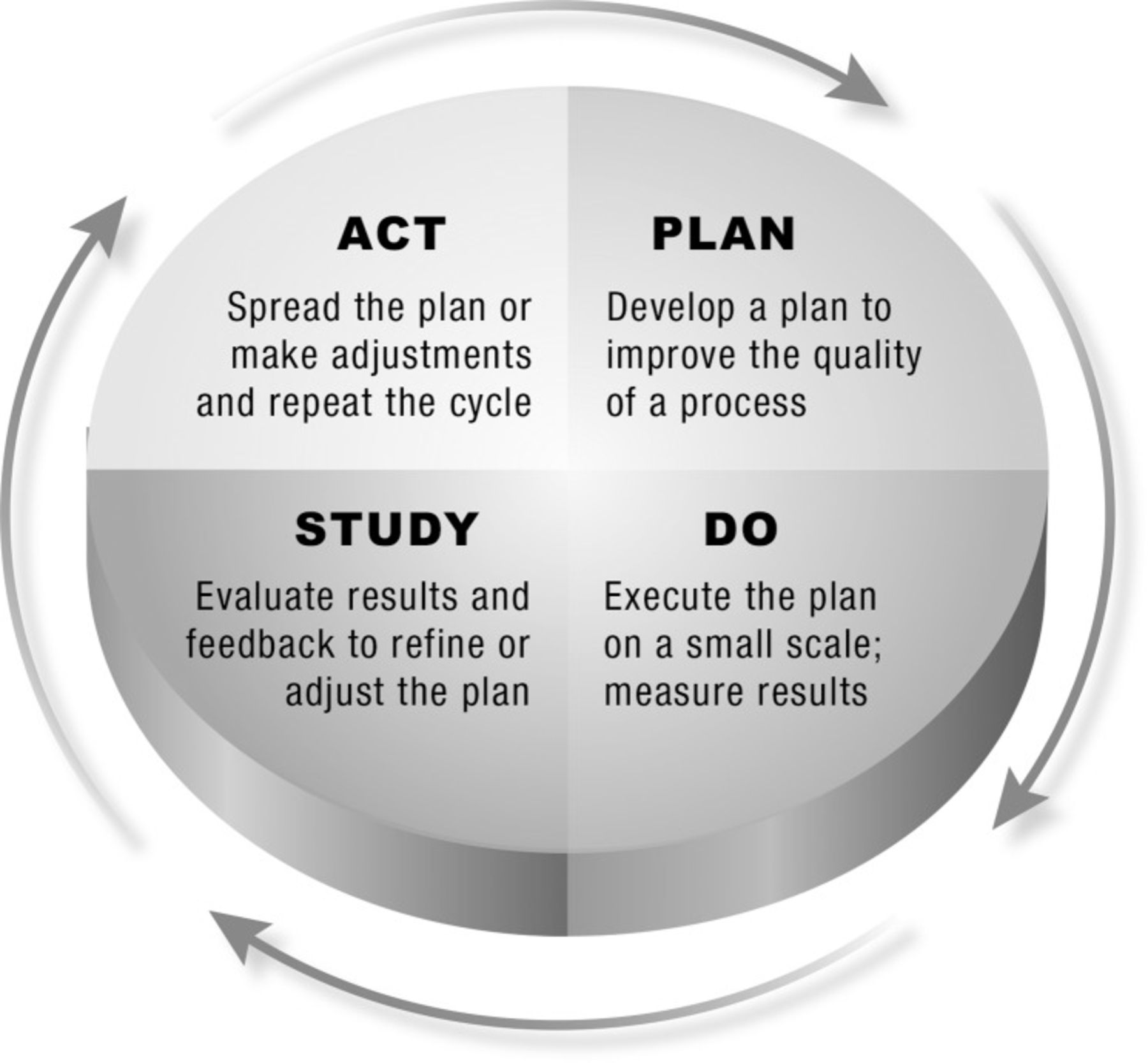
The Institute for Healthcare Improvement recommends use of plan-do-study-act (PDSA) cycles as a framework for process improvement in its Model for Improvement.2 The PDSA concept and application were first introduced by Walter A. Shewhart and W. Edwards Deming, who were pioneers in quality management and whose work influenced business leaders, corporations, and governments around the world.3 Initially used by Bell Laboratories and the post–World War II Japanese manufacturing industry for total quality management, PDSA is considered to be the mainstay of improvement science in healthcare. Starting with small changes and limited scope, the PDSA cycle may be used for rapid tests of change that build progressively with each cycle (Figure 2).

Plan-do-study-act cycle.
Survey data collected at OMC in the fourth quarter of 2012 pointed to the administration of mealtime insulin in relation to the delivery and consumption of meals as an opportunity for improvement. In response to this finding, a PDSA rapid-change cycle was initiated by an endocrinology fellow and the diabetes program coordinator (Figure 3). The aim was to improve patient satisfaction with regard to appropriate timing of blood glucose monitoring and mealtime insulin administration by 5% to 10% within 2 months' time. The intervention was enacted on a medical surgical unit chosen for the type of patients it treats and its abundance of new nursing staff. The intervention involved unit-specific education for the bedside nurses—sessions for both the day and night shifts—during scheduled monthly staff meetings. The sessions were led by an endocrinology fellow and the diabetes program clinical coordinator. The content of the presentations included the differences between type 1 and type 2 diabetes, stress hyperglycemia, and the pharmacokinetics of rapid- and long-acting insulin used to manage hyperglycemia in hospitalized patients. The intervention highlighted the importance of appropriate timing of blood glucose monitoring and insulin administration in relation to mealtimes, mimicking as closely as possible the normal insulin response by the pancreas linked to improved clinical outcomes. These sessions were well received by nursing staff.

Plan-do-study-act cycle for the insulin administration and meal delivery project.
RESULTS
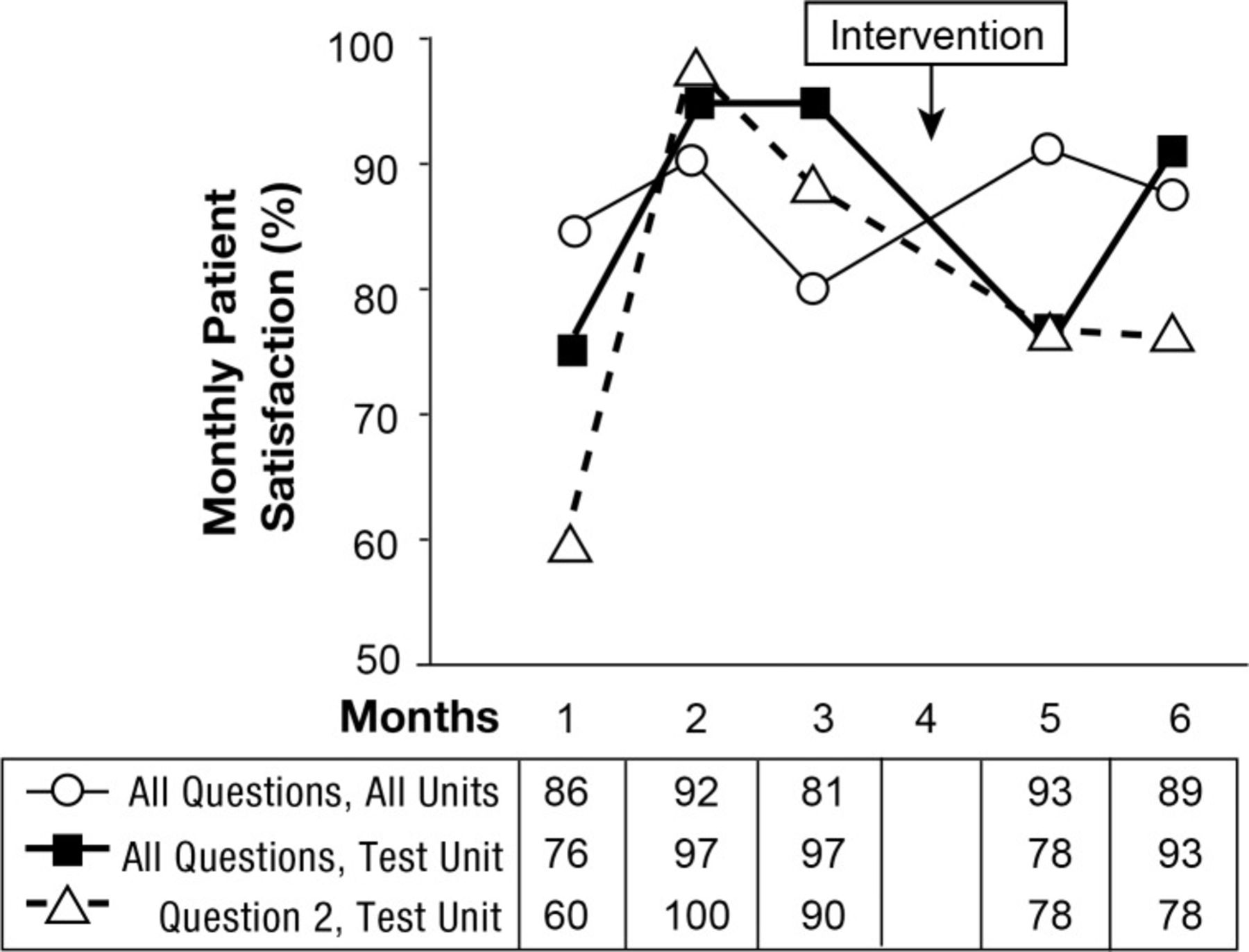
Baseline preintervention data for the test unit were obtained from questionnaire responses provided by 30 patients during October, November, and December 2012. Patient satisfaction with respect to mealtime insulin administration (question 2) was scored at 83% during this final quarter of 2012. Patient satisfaction for the same question and test unit was assessed after the intervention was implemented in January and found to be 78% for the 2 test months of February and March 2013. Because these data were based on convenience samples, the number of respondents varied between the preintervention and the postintervention surveys. Despite the intervention, the test unit's patient satisfaction score for mealtime insulin administration decreased by 5 percentage points, from 83% to 78%. However, the significance of this change is unclear because of the 6-percentage-point decrease in overall satisfaction with diabetes care during the same time period for the test unit (Table and Figure 4).
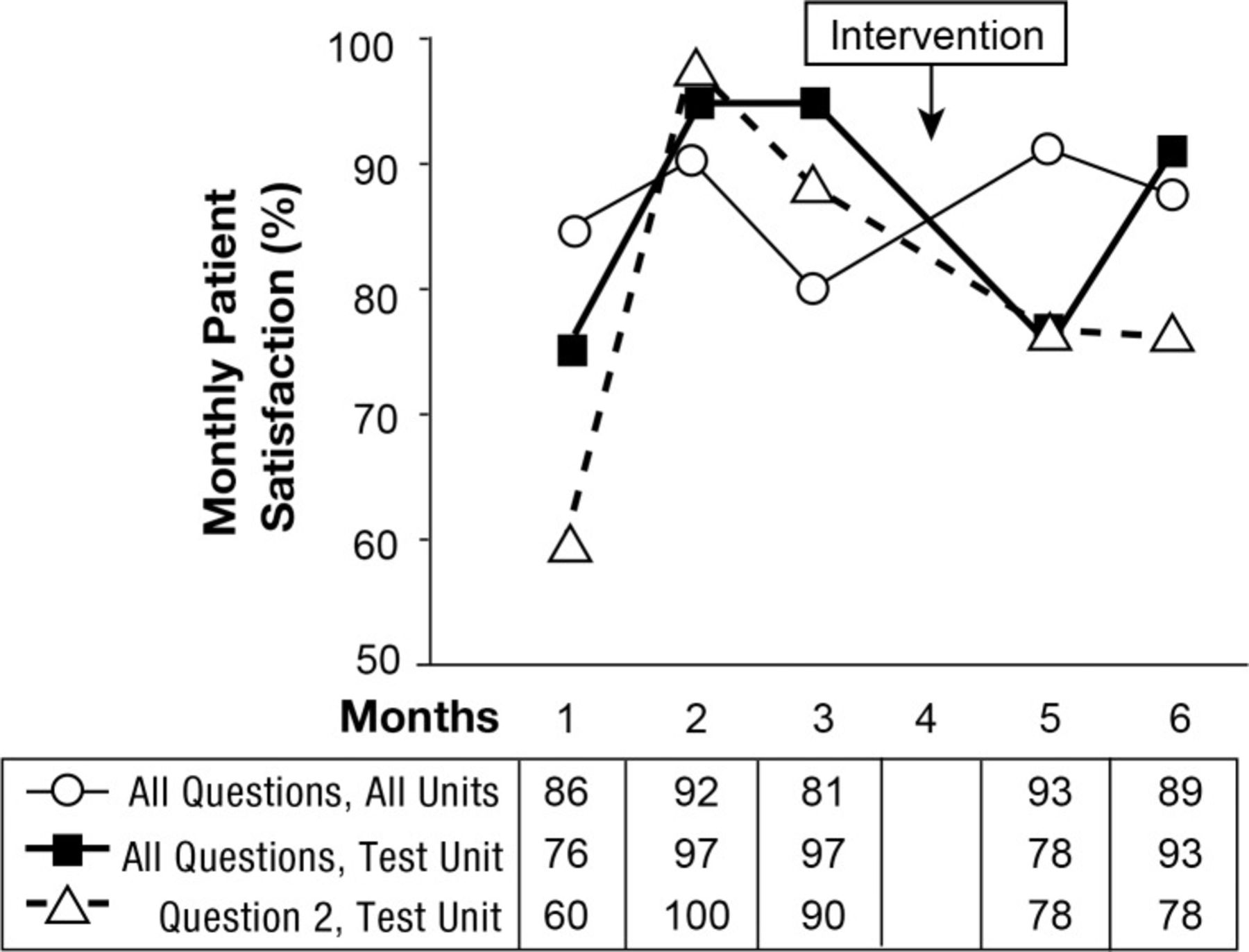
Monthly patient satisfaction scores before and after intervention.
DISCUSSION
The first cycle intervention proved ineffective, with results falling far short of the 5%-10% improvement goal. Both the survey and the intervention had limitations. The survey was affected by several biases, including recall bias (eg, patient forgetting) and response bias. In several instances, patients answered in front of family members and/or nurses and possibly wanted to supply the “correct” response. Furthermore, the survey population was not randomized. Although all patients who met the aforementioned criteria were included in the survey population, the first 10 respondents were sampled based on convenience and availability. The remarkably higher standard deviation for question 2 responses obtained per month (20.8) when compared to that for the other survey questions (12.1) may indicate that question 2 is more difficult for respondents to understand, thus creating variability in interpretation for an affirmative response.
Education alone is generally not the best intervention for quality improvement or medication safety. Nevertheless, the unit-specific education session with bedside nurses served to reduce variation in nurses' knowledge so that other system issues could be addressed in later stages of this rapid-change project. This particular approach of enacting, evaluating, and revising or adjusting a small-scale intervention is in line with the characteristic nature of PDSA methodology. These findings indicate that a different and/or additional intervention is needed. This first cycle relied completely on the interaction of the patient and nurse and the effectiveness of their communication. The next cycle should include a third factor.
Ideas for the third factor are being considered, including the distribution of educational pamphlets to patients when they are admitted to the hospital, the placement of posters in patients' rooms to remind both nurses and patients of the importance of matching the timing of insulin administration to food intake, and inclusion of dietary personnel in the process change.
The coordination of glucose testing, nutrition delivery, and insulin administration is integral to the safe management of hyperglycemia and diabetes in the hospital. Historically, national guidelines for the treatment of diabetes4 have called for consistent meal plans, which are preferred by many hospitals because of the enhanced ease of matching the prandial insulin dose to the amount of carbohydrate consumed that they permit.5 However, current nutrition recommendations for hospitals, as opposed to the historical approach of standardization, advise meal plan individualization based on glycemic goals, physiological factors, and medications used for treatment.4
Individualization of meal plans coupled with synchronization of insulin administration, glucose monitoring, and meal delivery presents significant challenges. One observational cohort study found that for most patient meals (84%), patients did not receive rapid-acting insulin within 10 minutes before or after the meal began, and glucose monitoring was performed within 30 minutes before the meal only 43% of the time.6 Many methods have been applied to improve the timing of insulin administration in relation to meal delivery for hospitalized patients, including nurse page alerts of meal trays en route to units, equal distribution of diabetic patients among nursing assignments, meal times posted in patient rooms, standardized food delivery schedules, no scheduling of inpatient procedures during mealtimes, signs on the doors of patients scheduled to receive insulin, engagement of dietary personnel and patients, and nursing education programs.7-9 While nurses are essential to these processes, they may not fully understand the importance to inpatient hyperglycemia management or be supported by optimal processes that ensure coordination of meals and insulin administration.
As hospitals move toward greater patient-centered care, patient-controlled diets are increasing in popularity. Patient-controlled diets empower inpatients to make menu selections and receive individualized nutrition education. The effect on glucose control for hospitalized patients is unclear. Medical nutritional therapy (MNT), individualized dietary assessment and instruction incorporating diet therapy counseling for a nutrition-related problem that is above basic nutrition counseling, has been a mainstay for inpatient glycemic control. For patients with diabetes, MNT usually includes a consistent carbohydrate meal plan.
Typically, nurses do not deliver meals and may be unaware of a patient's receipt of a meal tray. Patient-controlled diet plans not only require appropriate food choices but also engagement of the patient to alert the nurse for insulin administration. Dietary staff, nurses, and patients all require training. Processes involving alert systems will be needed. Patient education should start now by educating patients to notify their nurse when meal trays arrive, ensuring the meal will not be consumed until after blood glucose is monitored and prandial and correction dose insulin is administered. The literature regarding insulin therapy and MNT has yet to fully address the issue of patient-controlled diets for hospitalized patients, raising implications for patient-centered meal delivery in hospitals.
CONCLUSIONS
Self-assessment of diabetes care revealed an area for improvement regarding appropriate glycemic management of patients with diabetes, specifically poor patient satisfaction because of ill-timed blood glucose monitoring and insulin administration relative to meal tray delivery. It is therefore critical to educate both the patient and the patient's family on the importance of informing the nurse when the meal tray has arrived and of waiting to have blood glucose levels checked and insulin administered before eating. Possible solutions could vary from signs or posters in the patient's room to a process integrated into the electronic health record that alerts the nurse to a patient's request for a meal. Education of frontline staff alone was not an adequate intervention for our quality improvement initiative to succeed.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care and Practice-Based Learning and Improvement.
Monthly Patient Satisfaction Scores Before and After the Intervention
Footnotes
The authors have no financial or proprietary interest in the subject matter of this article.
- © Academic Division of Ochsner Clinic Foundation








{kind=link}
{kind=link}
{kind=link}
{kind=link}