
Abstract
Background Transforaminal lumbar interbody fusion (TLIF) is the standard surgical treatment for patients with lumbar degenerative spondylolisthesis who do not respond to a 6-week course of conservative therapy. A number of morbidities are associated with the conventional open-TLIF method, so minimally invasive surgery (MIS) techniques for TLIF (MIS-TLIF) have been introduced to reduce the trauma to paraspinal muscles and hasten postoperative recovery. Because providing cost-effective medical treatment is a core initiative of healthcare reforms, a comparison of open-TLIF and MIS-TLIF must include a cost-utility analysis in addition to an analysis of clinical effectiveness.
Methods We compared patient-reported clinical functional outcomes and hospital direct costs in age-matched patients treated surgically with either open-TLIF or MIS-TLIF. Patients were followed for at least 1 year, and patient scores on the Oswestry Disability Index (ODI) and visual analog scale (VAS) were analyzed at 6 weeks, 6 months, and ≥1 year postoperatively in the 2 treatment groups.
Results Compared to their preoperative scores, patients in both the open-TLIF and MIS-TLIF groups had significant improvements in the ODI and VAS scores at each follow-up point, but no significant difference in functional outcome occurred between the open-TLIF and MIS-TLIF groups (P=0.46). However, open-TLIF is significantly more costly compared to MIS-TLIF (P=0.0002).
Conclusion MIS-TLIF is a more cost-effective treatment than open-TLIF for patients with degenerative spondylolisthesis and is equally effective as the conventional open-TLIF procedure, although further financial analysis—including an analysis of indirect costs—is needed to better understand the full benefit of MIS-TLIF.
- Costs and cost analysis
- outcome assessment
- pain measurement
- spinal fusion
- spinal instrumentation
- spondylolisthesis
- surgical procedures–minimally invasive
INTRODUCTION
Lumbar degenerative spondylolisthesis is relatively common in men (2.7%) and women (8.4%).1 Studies have demonstrated the superiority of surgical treatment once patients fail a 6-week trial of standardized nonsurgical treatment that includes physical therapy, medications, and spinal injections.2 Several spinal fusion techniques have been used over the years; they all aim to decompress the neural elements and stabilize the spinal segment through spinal arthrodesis with pedicular instrumentation.
Lumbar interbody arthrodesis techniques via dorsal spine approaches allow for circumferential fusion via a single posterolateral approach and have been performed for many years with good results.3,4 In 1982, Harms and Rolinger first described the open transforaminal lumbar interbody fusion (TLIF) technique,5 a procedure that has proven to be effective.6 However, multiple studies have reported the destructive effects of the extensive muscle dissection and retraction required for the open-TLIF procedure.7,8 The extensive soft tissue dissection is necessary to expose the anatomic landmarks for pedicle screw insertion, to achieve a proper lateral-to-medial screw trajectory, and to resect the facet complex. The significant iatrogenic muscle and soft tissue injury that occurs during the surgical approach can result in increased postoperative pain, lengthened recovery time, and impaired spinal function.
Recently, minimally invasive surgery (MIS) techniques for TLIF (MIS-TLIF) have been introduced with the goals of smaller operative wounds, reduced trauma to paraspinal muscles, and quicker postoperative recovery, all of which may in turn result in minimized estimated blood loss, decreased hospital length of stay (LOS), and decreased rates of surgical site infection9-11 in contrast to the protracted hospital stays and significant costs associated with open-TLIF procedures.12,13
Because providing cost-effective medical treatment is a core initiative of healthcare reforms, a comparison of open-TLIF and MIS-TLIF must include a cost-utility analysis in addition to an analysis of clinical effectiveness. Consequently, the purpose of this study was to perform a comparative analysis of treatment effectiveness and of the direct costs of open-TLIF vs MIS-TLIF in age-matched patients diagnosed with degenerative spondylolisthesis grades 1-2.
METHODS
From 2009 to 2012, the lead author maintained a database in which patient demographics; diagnoses; and surgery data including estimated blood loss, perioperative morbidity and surgical complications, hospital LOS, and direct hospital cost data were collected prospectively. For this study, we retrospectively reviewed the data of patients who underwent either open-TLIF or MIS-TLIF and met the following inclusion criteria: (1) evidence on magnetic resonance imaging of grade 1 or 2 degenerative lumbar spondylolisthesis, (2) mechanical low back pain and radicular leg symptoms, (3) lack of response to at least 6 weeks of conservative therapy, and (4) age 18 to 80. Patients were excluded if they had an active medical or worker's compensation lawsuit or any preexisting spinal pathology. The institutional review board approved this study.
The lead author performed all the open-TLIF and MIS-TLIF procedures. In addition, all patients had nearly identical postoperative treatment paradigms based on a standardized postoperative order set. Patients were also sent for physical therapy at 3-4 weeks postoperatively as needed and returned to work as soon as they felt capable, as early as 4-8 weeks postoperatively.
Surgical Techniques
MIS-TLIF
Patients were positioned prone on the Jackson table for all surgeries, and intraoperative fluoroscopy was used at each critical stage of the surgery starting with identification of spinal operative level. The MIS-TLIF procedure was performed on the side of radicular symptoms or on the more symptomatic side if the patient had bilateral leg pain. Paramedian incisions 1-2 inches long were made on the lateral borders of the facet joints of the spinal level as visualized on fluoroscopy. Sequential soft-tissue dilators were then inserted through the incision down to the facet complex until the desired working diameter was achieved. A laminotomy and facetectomy were then performed with a high-speed drill and Kerrisons of different configurations until the ligamentum flavum was visualized. The flavum was removed piecemeal. In patients with unilateral leg pain, we decompressed both the exiting and traversing nerve roots in a manner similar to the open Gill procedure. In cases of bilateral leg pain, we did a wider laminectomy by angling our tubular retractor medially and drilling across, through the contralateral lamina; removing the flavum; and undercutting the overgrown facet. Hence, the contralateral nerve roots were also visualized and decompressed. We made a wide rectangular annulotomy, used disc space shavers of different sizes to do a complete discectomy, and used a ring curette to remove cartilaginous endplate materials. We placed a mixture of autograft from the facet joint and bone morphogenetic protein (Infuse; Medtronic) anteriorly in the disc space. We packed a polyetheretherketone (PEEK) interbody device with autograft and inserted it in the disc space as well, using fluoroscopy to ensure satisfactory placement. Once the interbody fusion was performed, we removed the tubular retractor and placed 4 pedicle screws percutaneously immediately above and below the interbody segment to be fused. Compression was applied to the construct before final tightening, providing compression of the bone graft within the middle column and maximizing lordosis. All wounds were copiously irrigated, and the wounds were closed in layers.
Open-TLIF
Patients were positioned prone on the Jackson table. A midline skin incision was made. The fascia was incised and the paravertebral muscles dissected from the spine. Fluoroscopy was used to localize the spine level. A wide laminectomy and facetectomy were performed with full decompression and visualization of the exiting and traversing nerve roots (Gill procedure). An annulotomy was made, followed by complete discectomy and endplate preparation. The same mixture of autograft and Infuse as well as PEEK cage used for MIS-TLIF were used for interbody fusion. Bilateral pedicle screws and rods were inserted using standard anatomic landmarks and fluoroscopy as needed. Compression was applied to the construct before final tightening, providing compression of the bone graft within the middle column and maximizing lordosis. All wounds were copiously irrigated, and the wounds were closed in layers.
Hospital Course and Perioperative Quality
Length of surgery, estimated blood loss, perioperative complications, and hospital LOS were recorded. Hospital readmission during the 90-day global period was recorded as was return to the operating room during the 2-year follow-up period. All morbidity and mortality occurring within the first 3 months after surgery were recorded.
Clinical Outcome Measures
Patient-reported functional outcomes were pain, disability, and quality of life that were assessed preoperatively (baseline) and at 6 weeks, 6 months, and ≥1 year. Assessments were principally done during clinic follow-ups, except for the ≥1-year assessment when we alternatively collected the data via phone interviews. Patient-assessed questionnaires included the visual analog scale (VAS) for low back pain and leg pain14,15 and the Oswestry Disability Index (ODI) for disability and quality of life.16,17
Hospital Direct Cost
The hospital accounting and billing office provided us with direct hospital costs for all patients included in this study. The costs included labor, medical supplies including implants, and other costs such as equipment and general/administrative costs that are expensed to all of the hospital cost centers. Cost data did not represent billing or charges but rather cost center–level expenditures incurred by the hospital to deliver care allocated to personnel, resource consumption, and overhead cost, among others.
Statistical Analysis
Parametric data were given as mean ± SD (standard deviation) and paired t tests were used to assess statistical significance between groups at each follow-up. The Wilcoxon rank-sum test was used to compare the VAS scores at each time point and between groups because the VAS is not normally distributed. Student t tests were employed to compare ODI scores at each time point and between groups. A value of P<0.05 was considered statistically significant.
RESULTS
A total of 68 patients (11 open-TLIF and 57 MIS-TLIF) were included in the study (Table). The mean age at time of surgery was 56 years for the open-TLIF cases and 61 years for the MIS-TLIF cases. The majority of the patients were women (64% of the patients who received open-TLIF and 70% of the patients who received MIS-TLIF). All patients presented with back and leg pain, as well as radiographic evidence of grade 1-2 degenerative spondylolisthesis. One patient in the open-TLIF group and 16 patients in the MIS-TLIF group had grade 2 spondylolisthesis; all other patients had grade 1 spondylolisthesis.
Characteristics of Patients Undergoing Open-TLIF and MIS-TLIF
The majority of the patients in the open-TLIF group (82%) had 2-level disease, while most patients in the MIS-TLIF group had 1-level disease (79%).The most common disease level was L4-L5 for the MIS-TLIF group and L5-S1 for the open-TLIF group. Body mass index, preoperative ODI, and VAS scores were not significantly different between the 2 groups.
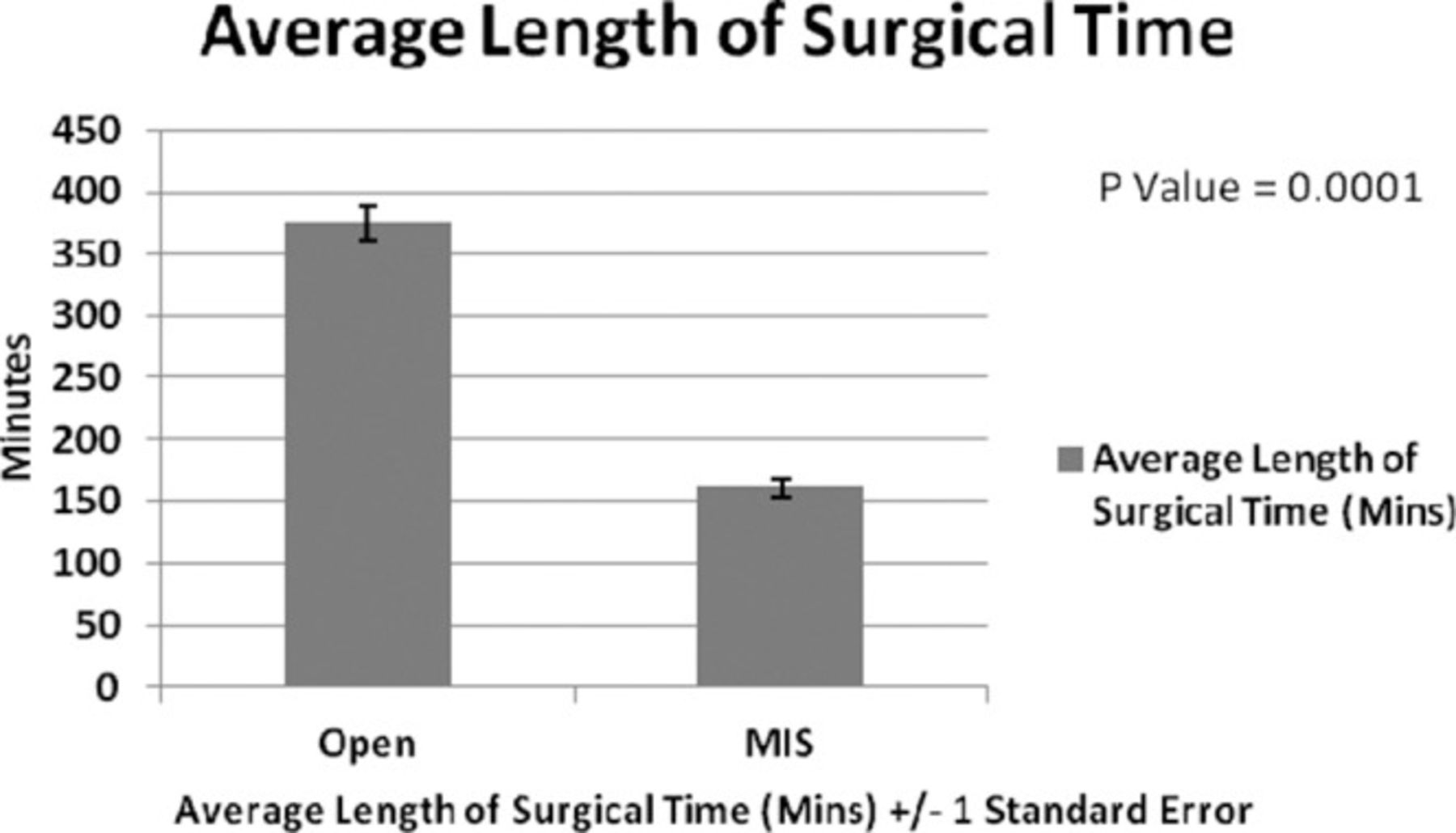
Duration (mean ± SD) of surgery was significantly longer for MIS-TLIF vs open-TLIF procedures: 161 minutes ± 7.6 minutes vs 375 minutes ± 14 minutes, respectively (P<0.0001) (Figure 1). Mean estimated blood loss was significantly less in the patients receiving MIS-TLIF vs open-TLIF: 95 mL ± 20 mL vs 786 mL ± 107 mL, respectively (P<0.0001) (Figure 2). The incidence of complications was higher in the open-TLIF cases; 2 of 11 (18%) patients in that group had complications compared to 4 patients (7%) in the MIS-TLIF group. No permanent neurologic complications occurred in the 2 groups. Three malpositioned screws in the MIS-TLIF group needed revision, and 1 dura tear was repaired during the surgery. One dura tear in the open-TLIF group was repaired during surgery, and 1 major wound infection occurred. The patient with the wound infection was readmitted 3 times for wound irrigation and debridement. No patients in the MIS-TLIF group were readmitted or developed a wound infection. The mean hospital LOS (Figure 3) was similar in both groups (3.2 days ± 0.2 days in the open-TLIF group vs 3.6 days ± 1 day in the MIS-TLIF group) and was not statistically significant (P=0.82).
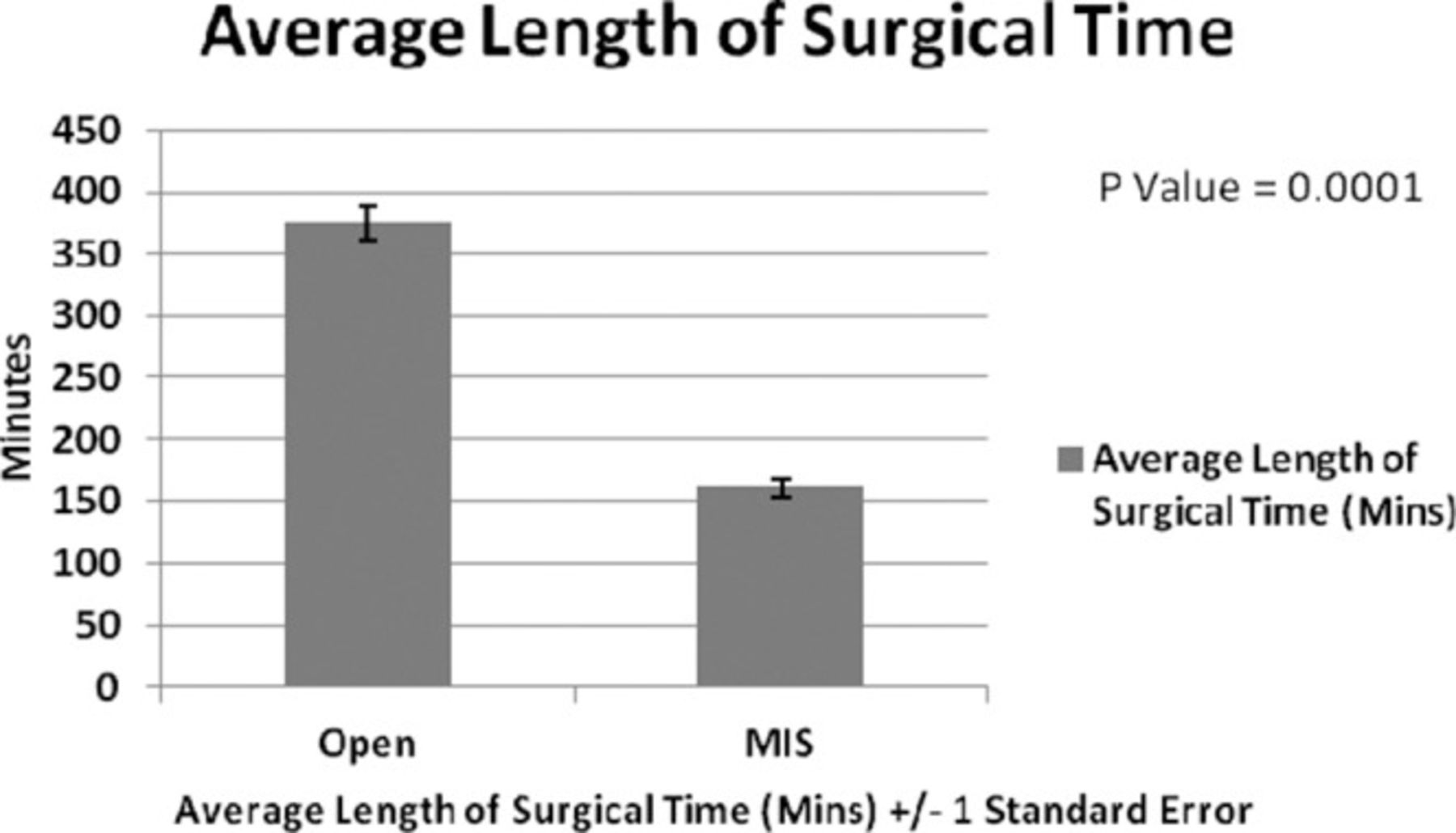
Average length of surgical time comparison between the open transforaminal lumbar interbody fusion group and the minimally invasive surgery (MIS) transforaminal lumbar interbody fusion group.

Average estimated blood loss comparison between the open transforaminal lumbar interbody fusion group and the minimally invasive surgery (MIS) transforaminal lumbar interbody fusion group.

Average hospital length of stay comparison between the open transforaminal lumbar interbody fusion group and the minimally invasive surgery (MIS) transforaminal lumbar interbody fusion group.
Patients in both groups showed significant improvement from preoperative score at the 6-week, 6-month, and ≥1-year time points in both outcome metrics. For the ODI (Figure 4), on a scale of 0% (no disability) to 100% (complete disability), mean scores for patients in the open-TLIF group were 57.8% vs 37.9% vs 41.2% vs 46.1% (P<0.0001) at baseline, 6 weeks, 6 months, and ≥1 year, respectively. For patients in the MIS-TLIF group, ODI mean scores were 53.7% vs 30.8% vs 26.4% vs 26.4% (P<0.0001), at baseline, 6 weeks, 6 months, and ≥1 year, respectively.
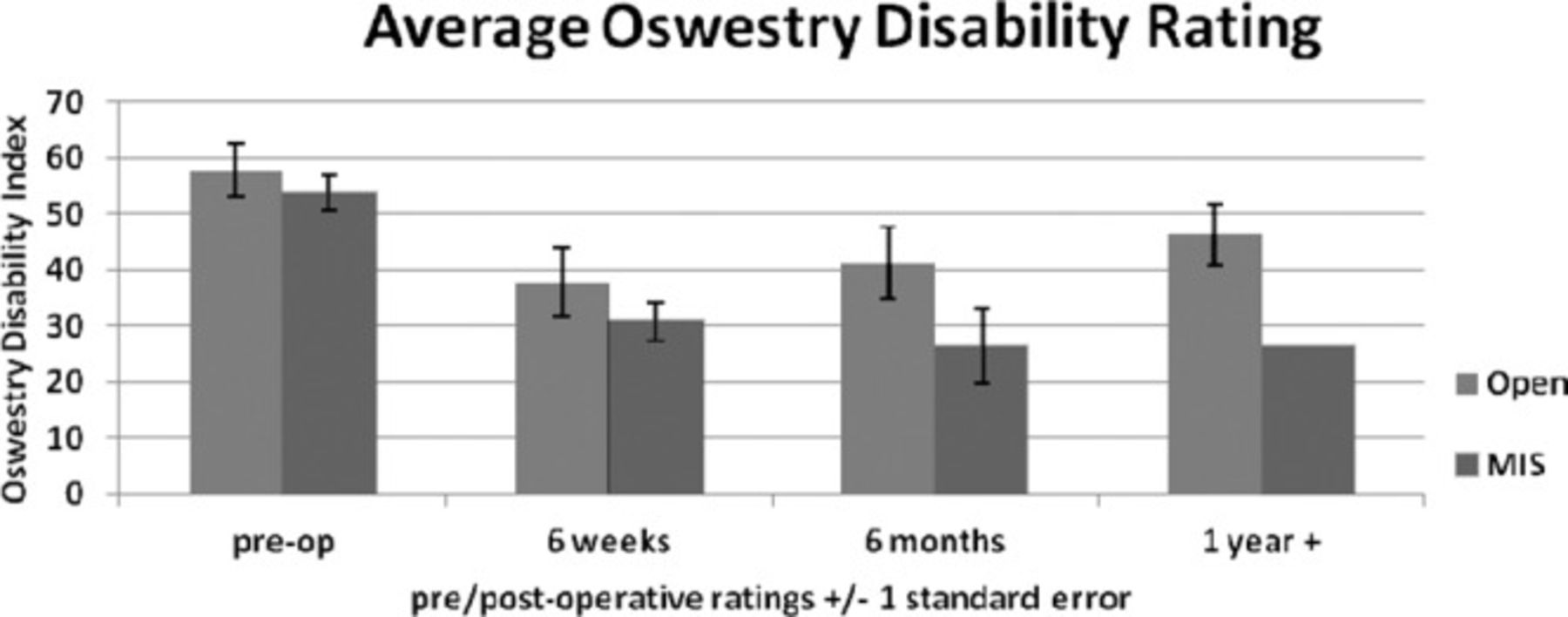
Average Oswestry Disability Index scores at baseline and 3 follow-ups in the open transforaminal lumbar interbody fusion group and the minimally invasive surgery (MIS) transforaminal lumbar interbody fusion group.
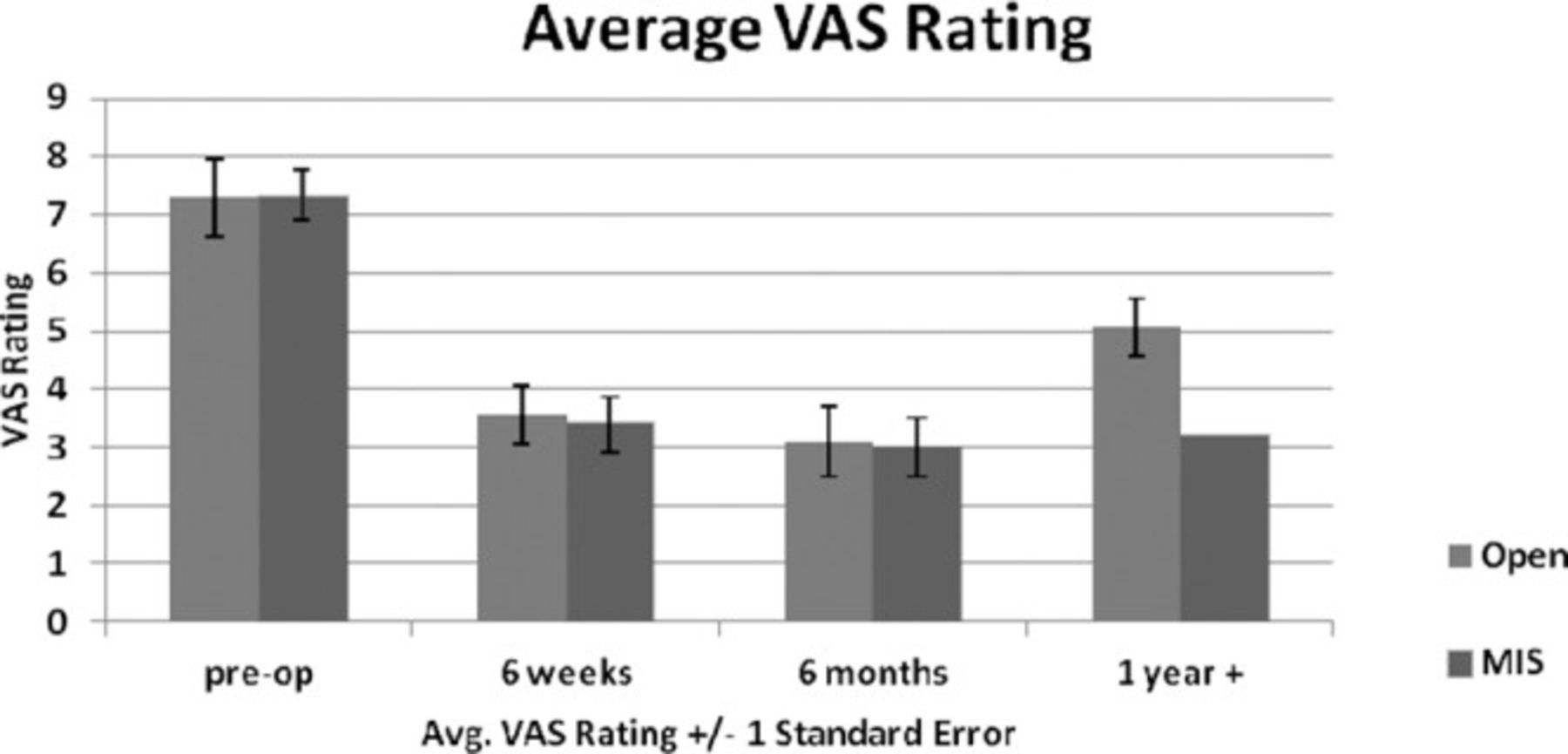
For the VAS (Figure 5), on a scale of 0 for no pain to 10 for the worst pain imaginable, scores for the patients in the open-TLIF group were 7.3 vs 3.6 vs 3.1 vs 5.1 (P<0.0001) and scores for the patients in the MIS-TLIF group were 7.3 vs 3.4 vs 3.0 vs 3.2 (P<0.0001) at baseline, 6 weeks, 6 months, and ≥1 year, respectively. The overall comparison of functional outcomes was not significantly different between the open-TLIF and the MIS-TLIF groups (P=0.46).

Average visual analog scale (VAS) scores at baseline and 3 follow-ups in the open transforaminal lumbar interbody fusion group and the minimally invasive surgery (MIS) transforaminal lumbar interbody fusion group.
We also assessed the direct hospital cost for all patients throughout their hospital stay (Figure 6). The mean hospital direct cost of patients who underwent open-TLIF was $37,681 compared to $19,098 for those who underwent MIS-TLIF, and this difference was significant (P<0.0002).
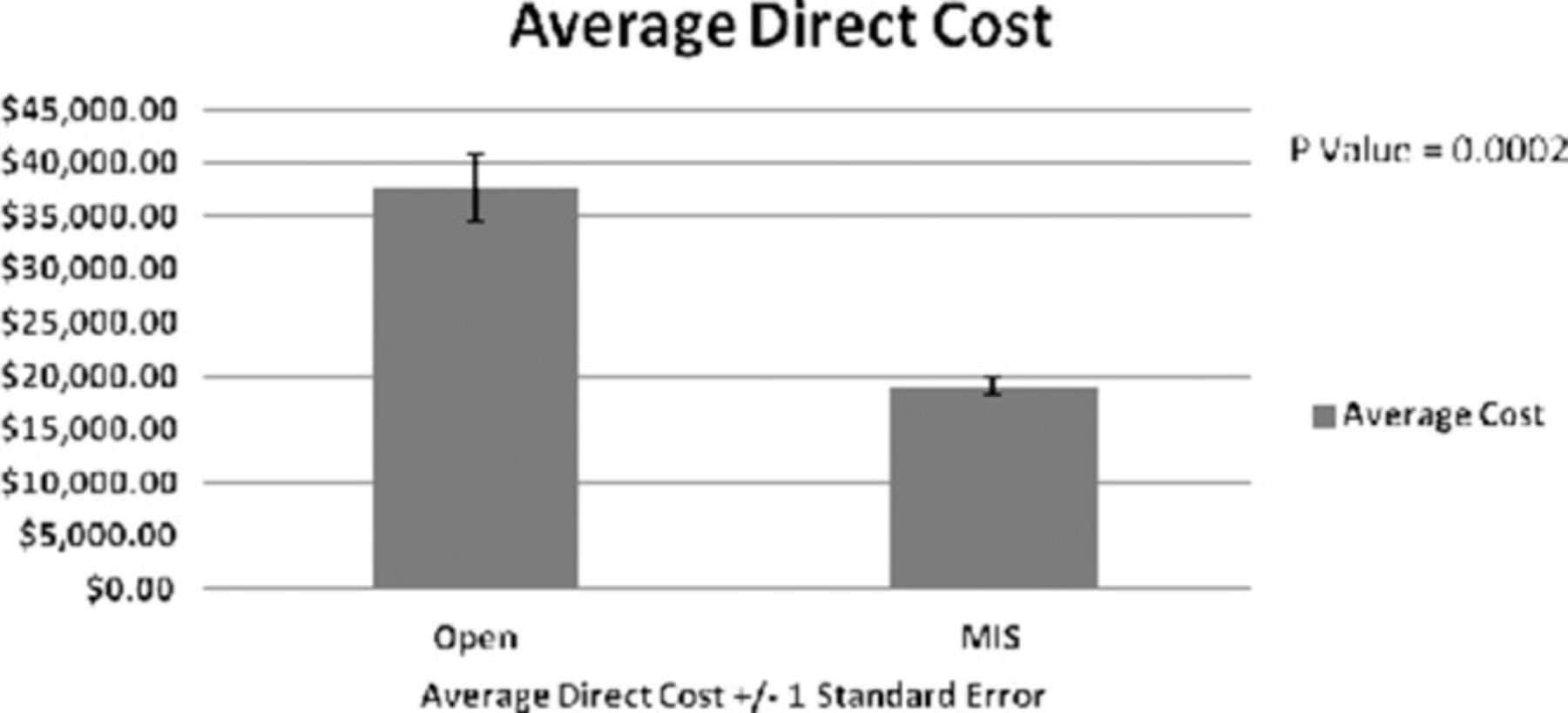
Average direct hospital costs comparison between the open transforaminal lumbar interbody fusion group and the minimally invasive surgery (MIS) transforaminal lumbar interbody fusion group.
DISCUSSION
Patients in both groups showed significant improvement from their preoperative ODI and VAS scores at each time point postoperatively, but no significant difference in functional outcomes occurred between the open-TLIF and MIS-TLIF groups, confirming that both treatment options are equally efficacious in treating patients with degenerative spondylolisthesis. This finding is consistent with previous studies that compared short- and long-term effectiveness between MIS and open approaches. In a prospective comparison study, Peng et al18 demonstrated significant improvement in back pain and lower limb symptoms, low back-specific disability, and quality of life at 6 months and 2 years for patients undergoing MIS-TLIF vs open-TLIF, but no significant difference in the amount of improvement existed between the 2 groups. The comparison studies of Dhall et al19 and Schizas et al11 also demonstrated similar improvement for patients undergoing MIS-TLIF vs open-TLIF.
We did note that patients who underwent MIS-TLIF recovered faster and were able to return to their daily activities earlier than patients who received open-TLIF and this is illustrated in the larger and more sustainable improvement in ODI scores in the patients who received MIS-TLIF compared to the patients who received open-TLIF. Although no significant difference in the ODI and VAS scores occurred between the groups, patients in the MIS-TLIF group had lower scores (better outcomes) than patients in the open-TLIF group.
A comparison of direct hospital costs in the 2 groups showed that open-TLIF is significantly more costly to the hospital than MIS-TLIF. This finding is similar to the finding of Scott et al despite their more extensive cost analysis.20 All studies, including ours, comparing open-TLIF vs MIS-TLIF found less estimated blood loss in patients undergoing MIS-TLIF.9,10,12,20 In our series, we did not find significant difference in the hospital LOS between the 2 groups, contrary to other studies.9,10,12,20 We believe that this difference may be the result of the longer hospital stays for MIS-TLIF patients who required reoperation due to screw malposition. When we calculated the average LOS without these 3 patients, the LOS for patients in the MIS-TLIF group was significantly lower than in the open-TLIF group (data not included). Earlier hospital discharge is important because it encourages earlier and more frequent ambulation, reduces exposure to nosocomial pathogens, and decreases medical resource utilization and hospital costs.9,21-23 We plan to continue our analysis of factors that may contribute to a longer LOS.
Cost-utility analysis and various forms of value analysis are important to healthcare reform initiatives. To improve the efficiency and cost of healthcare delivery, value-based purchasing has emerged that requires each costly medical treatment to demonstrate a health benefit that is greater than its added cost. Care that is more costly than its alternative but fails to provide added health benefits is considered cost ineffective. Care that is more costly than its alternative but provides a health benefit greater than its added cost is considered cost effective. Although the cost-effectiveness threshold is debated, it historically has been defined as less than $50,000 per quality-adjusted life year gained. Care that is less costly than the alternative and equally effective is considered cost saving. Care that is both less costly and more effective is considered cost dominant.20
The societal cost of healthcare comprises direct costs (all healthcare expenditures) and indirect costs (occupational productivity losses of patient and caregivers), both of which are equally important despite the fact that we only evaluated direct costs in our study. Our direct cost analysis demonstrates that MIS-TLIF is a more cost-effective treatment option for the hospital. We plan to perform further analysis of the indirect costs to better understand the cost effectiveness of MIS-TLIF vs open-TLIF.
CONCLUSION
In this retrospective review of treatment and cost effectiveness of MIS-TLIF and open-TLIF, we found that both treatment options are equally effective with regards to patient-reported outcomes, but open-TLIF was less cost effective than MIS-TLIF based on our analysis of hospital direct costs. MIS-TLIF may represent a valuable and cost-saving advancement for hospitals and employers but further cost analysis—including analysis of indirect costs—is required to better understand the cost implications of open-TLIF compared to MIS-TLIF for the treatment of patients with degenerative spondylolisthesis grades 1 and 2.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care, Medical Knowledge, and Practice-Based Learning and Improvement.
Footnotes
The authors have no financial or proprietary interest in the subject matter of this article.
- © Academic Division of Ochsner Clinic Foundation
REFERENCES
In this issue








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Cited By...
- Two-Year Clinical and Radiographic Outcomes for Percutaneous Lumbar Interbody Fusion With an Expandable Titanium Cage Through Kambins Triangle Without Facetectomy
- Biplanar Expandable Cages for Transforaminal Lumbar Interbody Fusion Are Safe and Achieve Good 1-Year Clinical and Radiological Outcomes in an Asian Population
- Biplanar Expandable Cages for Transforaminal Lumbar Interbody Fusion Are Safe and Achieve Good 1-Year Clinical and Radiological Outcomes in an Asian Population
- Methodology of economic evaluations in spine surgery: a systematic review and qualitative assessment
- Systematic Review of Cost-Effectiveness Analyses Comparing Open and Minimally Invasive Lumbar Spinal Surgery
- Comparison of Clinical Outcome and Radiologic Parameters in Open TLIF Versus MIS-TLIF in Single- or Double-Level Lumbar Surgeries
- Two-Year Clinical and Radiographic Outcomes of Expandable Interbody Spacers Following Minimally Invasive Transforaminal Lumbar Interbody Fusion: A Prospective Study
- Enhanced Recovery After Surgery Trends in Adult Spine Surgery: A Systematic Review
- Risk Factors for Medical and Surgical Complications After Single-Level Minimally Invasive Transforaminal Lumbar Interbody Fusion
- Minimally Invasive Transforaminal Lumbar Interbody Fusion: Comparison of Isthmic Versus Degenerative Spondylolisthesis
- Recent Publications by Ochsner Authors: October 2013 - March 2014