
Abstract
Background Facet joint arthrosis may play a significant role in low back pain generation. The placement of facet dowels is a percutaneous treatment that aims to fuse the facets and increase joint stiffness. In this cadaveric study, we evaluated spine stiffness after facet dowel insertion in combination with several surgical procedures and determined which motions promote dowel migration.
Methods Six fresh frozen lumbar spines were tested in flexion-extension, lateral bending, and axial rotation. Spine stiffness was determined for the intact specimens, after L4 laminectomy, and after bilateral L4-L5 facet dowel placement, respectively. One specimen underwent a unilateral transforaminal lumbar interbody fusion (TLIF) construct and another underwent extreme lateral interbody fusion (XLIF) graft (22 mm) placement, followed by placement of facet dowels. Afterwards, the specimens were subjected to 10,000 cycles of fatigue testing in flexion-extension or axial rotation.
Results The overall decrease in stiffness after laminectomy was 4.6%. Facet dowel placement increased overall stiffness by 7.2%. The greatest increase was seen with axial rotation (13%), compared to flexion, extension, and lateral bending (9.5%, 2.3%, and 5.6%, respectively). The TLIF and XLIF plus dowel construct increased specimen stiffness to 266% and 163% of baseline, respectively. After fatigue testing, dowel migration was detected by computed tomography in the 2 uninstrumented specimens undergoing axial rotation cycling.
Conclusion Facet dowels increase the stiffness of the motion segment to which they are applied and can be used in conjunction with laminectomy procedures to increase the stiffness of the joint. However, dowel migration can occur after axial rotation movements. Hybrid TLIF or XLIF plus facet dowel constructs have significantly higher stiffness than noninstrumented ones and may prevent dowel migration.
- Biomechanics
- foreign-body migration
- instrumentation
- laminectomy
- low back pain
- lumbar vertebrae
- surgical procedures–minimally invasive
INTRODUCTION
Low back pain is a major health problem in the United States—reported to occur in more than 80% of the population at some point in life—where it ranks as the third leading cause of disability.1 The most common etiology of low back pain involves chronic degeneration within the lumbar intervertebral discs and facet joints.2,3 Historically, this process has been thought to start within the disc space.4-7 However, because facet joint arthrosis has such a high radiographic occurrence, some believe the facets may play a more substantial role in pain generation.8-14
Traditional operative strategies to treat low back pain have aimed to fuse the motion segment that is believed to be the pain generator.15 The perioperative morbidities associated with open instrumented spinal fusion—such as blood loss, nerve injury, muscular atrophy, and pain—have led to the development of minimally invasive surgical techniques.16,17
The placement of facet dowels is a minimally invasive percutaneous treatment approach that aims not only to fuse the facet but also to increase the stiffness of the joint. Recently, dowels have been used with increasing frequency to provide spinal stabilization after decompressive procedures, such as lumbar laminectomies. In this study, we evaluated the stiffness of a lumbar motion segment after laminectomy before and after the insertion of bilateral facet dowels. We also evaluated the segmental lumbar stiffness after facet dowel insertion in combination with an extreme lateral interbody fusion (XLIF) construct and a transforaminal lumbar interbody fusion (TLIF) construct, respectively. Finally, we sought to determine which motions increase the likelihood of dowel migration.
METHODS
Specimen Preparation
Six cadaveric specimens underwent biomechanical evaluation to determine baseline, postlaminectomy, and post–facet dowel placement stiffness. The fresh frozen lumbar spines (L3-S1) were harvested from cadaveric specimens and used for testing. All specimens were screened using computed tomography (CT) to assess for major anatomical abnormalities and were prepared in accordance with the “recommendations for the standardization of in vitro stability testing of spinal implants” previously described.18 Specimens were kept frozen until the date of the experiment, at which time they were thawed slowly at room temperature. The specimens were cleaned of surrounding musculature, while the ligaments and facet capsules were left intact. Manual flexion-extension, lateral bending, and axial rotation movements were applied to each specimen to assess for any gross abnormality in motion. All specimens were screened to confirm that they had no major anatomical abnormalities and displayed neither gross instability nor limited movement due to autofusion. The specimens were potted using Bondo Body Filler (3M) to expose and allow motion only at the L4-L5 segment (ie, a functional spinal unit). Screws were then inserted into the potted vertebral bodies to strengthen the hold between the specimen and the plastic casing in which it was set (Figure 1).

Functional spinal unit biomechanical construct. The L4 and L5 vertebrae were stabilized in the upper and lower gimbal, respectively. The motions of the various spine parts were recorded.
Biomechanical Testing
Tests were performed for no more than 20 hours at temperatures between 20°C and 30°C. Specimens were wrapped in saline-moistened gauze to preserve tissue hydration. Biomechanical testing was performed using the MTS 858 Mini Bionix spine simulator (MTS). Before any data were collected, each specimen underwent preconditioning, consisting of 3 cycles of pure moment. Preconditioning was followed by 17 cycles of pure moment during which data collection occurred. The spines were tested in pure moments of flexion-extension, lateral bending, and axial rotation. Testing parameters are presented in the Table. Spine stiffness was determined for the intact specimens, after L4 laminectomy, and after bilateral L4-L5 facet dowel placement, respectively; hence, each specimen served as its own control. One specimen underwent a TLIF with polyetheretherketone cage and unilateral L4-L5 pedicle screw and rod instrumentation; the facet dowel was placed unilaterally on the opposite side. Another specimen underwent placement of an XLIF graft followed by bilateral facet dowel placement. Afterwards, the specimens were subjected to 10,000 cycles of fatigue testing. Two uninstrumented specimens were subjected to flexion-extension moments, while the remaining 2 uninstrumented and the 2 instrumented specimens were subjected to axial rotation fatigue cycling.
Biomechanical Lumbar Spine Testing Parameters
Facet Dowel Placement
Under oblique fluoroscopic visualization, a Steinmann pin was inserted into the center of the facet joint at an angle that was parallel to the articulating surface and perpendicular to the cranial-caudal axis. Lateral views were used to confirm placement at the level of the underlying superior endplate. After standard preparation of the facet with a reamer, the 5-mm TruFUSE tapered dowel (minSURG Corporation) was loaded into the inserter instrument and impacted into the facet joint to a depth of 13 mm bilaterally. All specimens received bilateral facet dowel placement with the exception of the 1 specimen in which the unilateral TLIF construct was used.
XLIF Construct
Under direct visualization, a standard L4-L5 discectomy was performed from a left lateral approach. A 22-mm graft was sized and subsequently inserted into the disc space. Bilateral facet dowels were then placed using the technique described previously.
TLIF Construct
Under direct visualization, a left-sided L4-L5 facetectomy, discectomy, and cage insertion were performed, followed by unilateral pedicle screws and rod insertion. The entry point was chosen at the junction between the transverse process and lateral facet, mimicking the placement of percutaneous pedicle screws. A unilateral facet dowel was then placed on the right side.
Imaging
After the dowel insertion, thin-cut (1 mm) CT images were obtained to identify the location of the dowels within the facet for each specimen. Repeat imaging was performed after fatigue cycling to assess dowel migration.
Statistical Analysis
A linear regression analysis was performed on data points placed on a load vs displacement curve. The slope of the curve was defined as the stiffness of each specimen during that point of testing.
RESULTS
The overall decrease in stiffness after laminectomy among the specimens was 4.6% when all pure moments were averaged. After placement of the facet dowels, an overall increase in stiffness of 7.2% was noted. The greatest increase in stiffness (13%) was seen with axial rotation moments (Figure 2), compared to flexion, extension, and lateral bending moments (9.5%, 2.3%, and 5.6%, respectively). The unilateral pedicle screw instrumentation with an interbody graft (TLIF) and contralateral facet dowel insertion increased the stiffness of the specimen to 266% of baseline. The XLIF graft in conjunction with bilateral facet dowels increased spine stiffness to 163% of baseline.
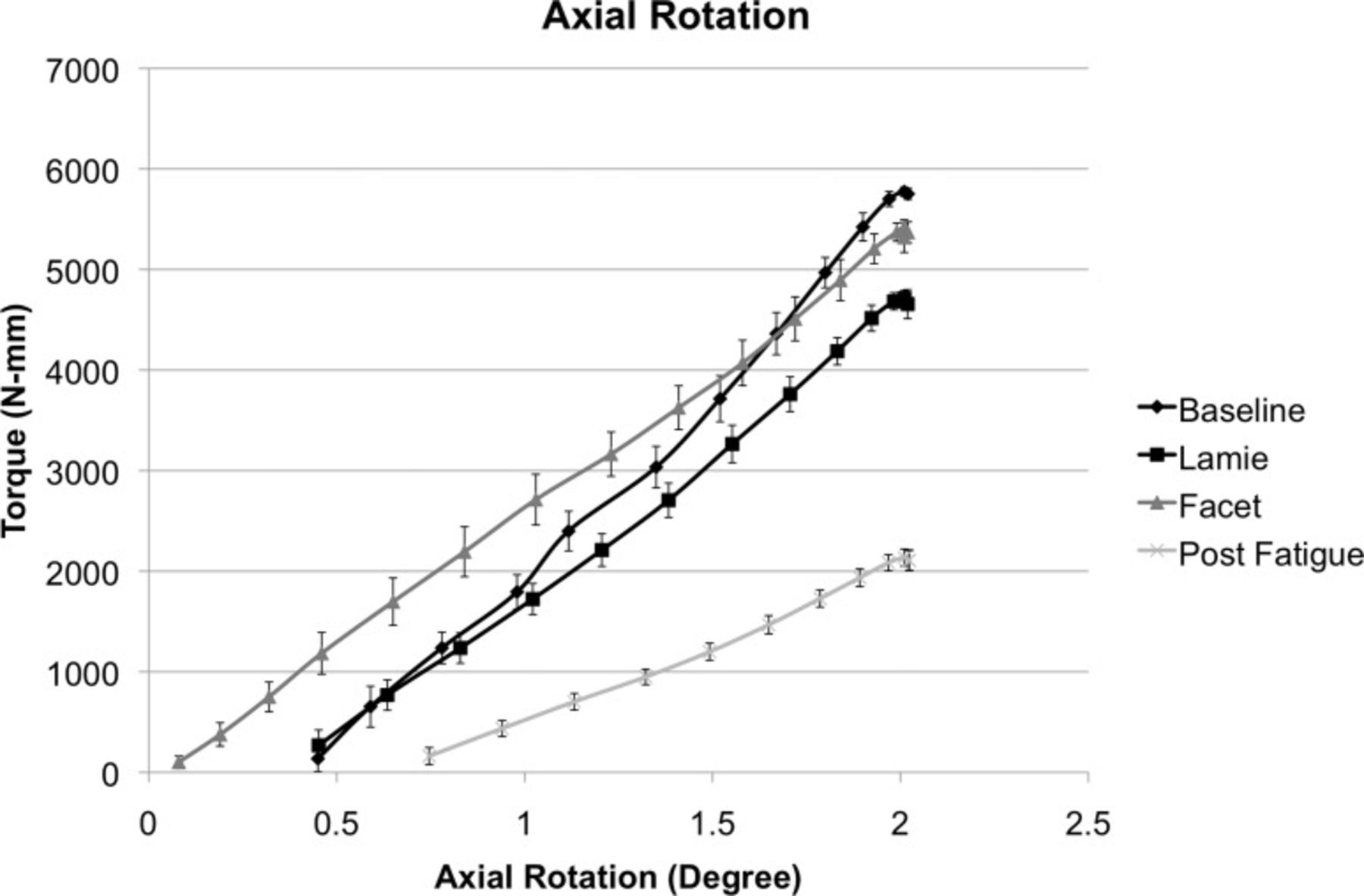
Spine testing in axial rotation. The spine stiffness decreased after the laminectomy (Lamie), but increased above baseline after bilateral facet dowel insertion (Facet). After 10,000 cycles in rotation, the spine was tested again, and the stiffness was significantly decreased.
Fatigue testing was performed on all 6 specimens. Of the 4 uninstrumented specimens that underwent fatigue cycling, dowel migration was noted in both specimens undergoing axial rotation cycling (Figure 3). In 1 of these axial rotation specimens, 1 facet dowel was extruded after approximately 7,000 cycles (Figure 4). Dowel migration was not seen on postfatigue imaging in either of the 2 instrumented specimens.

Axial computed tomography imaging before and after fatigue testing. The right facet dowel was expelled, whereas the left dowel only migrated in the facet joint by a few millimeters.

Bar graph showing the spine stiffness during fatigue testing of the noninstrumented specimen undergoing axial rotation that experienced a dowel expulsion. The stiffness decreased between 7,000 and 9,600 seconds, likely correlating with the right facet dowel expulsion.
DISCUSSION
Lumbar laminectomy procedures decompress the underlying neural structures at the expense of removing stabilizing ligamentous tissue. Previous biomechanical analysis of intact lumbar spines has shown that the posterior ligaments resist up to 60% of flexion forces, with the supraspinous and interspinous ligaments bearing the highest tensile forces.19 Conversely, rotational forces are resisted primarily by capsular ligaments with minimal effect from the midline posterior ligaments.20 Furthermore, the lumbar facet joint as a whole sustains a considerable amount of load in both rotational and extension movements.21-26 Disruption of these tissues via laminectomy and bilateral partial facetectomy decreases segmental stiffness and predisposes patients to spondylolisthesis.27,28
The data from our study confirm the destabilizing effects of laminectomy. In our study, the overall specimen stiffness decreased 4.6% after the laminectomy and increased 7.2% after facet dowel insertion. The greatest increase in stiffness was seen with axial rotation moments compared to flexion, extension, and lateral bending. This finding is expected because the facets' articular surfaces have a sagittal orientation that allows flexion-extension motion but resists axial rotation. When a tapered bone dowel is inserted into the facet, the articulating interface widens within the confined area created by the capsular ligaments. With this joint expansion comes an increase in stiffness of the facet joint that results in an increase in stiffness of the entire motion segment, as evidenced by our data.
In addition to increasing the stiffness of a motion segment, facet bone dowel placement also aims to create facet arthrodesis. Instrumented facet fixation has been described previously in techniques involving lumbar facet interface screws and translaminar facet screws.29,30 Although these technologies offer instrumented fixation, they do not provide a surface area to promote fusion. Facet bone dowels aim not only to immobilize the joint by increasing the stiffness but also to create arthrodesis via incorporation of allograft. However, with the lack of instrumented fixation, the likelihood of nonunion and/or bone dowel expulsion may be increased.
We subjected the lumbar specimens to a fatigue cycling of 10,000 cycles to assess the potential for dowel migration. To delineate whether specific pure moments may influence dowel migration, we submitted 2 specimens to flexion-extension, whereas 4 specimens underwent axial rotation cycling. These moments were chosen to mimic common physiologic movements. None of the specimens subjected to flexion-extension cycling exhibited dowel displacement on postfatigue CT scans. Conversely, both uninstrumented specimens undergoing axial rotation cycling showed evidence of dowel migration on postfatigue imaging. These findings might suggest that patients undergoing standalone facet dowel placement (with or without laminectomy) may need to limit rotational motions until the graft incorporation is confirmed (eg, by CT imaging). Moreover, once bone formation starts to occur between the dowel and the surrounding facets, the dowel is less likely to migrate out of the joint.
Two instrumentation constructs commonly used in clinical practice were chosen for further biomechanical evaluation. The TLIF plus unilateral facet dowel specimen showed a 266% increase in stiffness and no dowel migration on postfatigue imaging. Similarly, the XLIF with bilateral dowels specimen showed a 163% increase in stiffness and no postfatigue dowel migration. These findings suggest that the rigid fixation provided by the TLIF and XLIF constructs may create an optimal environment for the incorporation of the lumbar facet dowels (ie, facet fusion). Moreover, facet dowels are less expensive than a pedicle screw and rod construct and thus may prove beneficial by providing both an additional surface for fusion and cost savings.
Multiple variables must be considered when assessing possible etiologies for dowel kick-out. Our experimental design employed facet joint stresses considered physiologic for both the pure moment testing and fatigue cycling. Normal physiologic strain within the facet joint during axial rotation under 15 Nm moments has been shown to average a 19.25% strain on the capsular ligaments.31 The torque measured during axial rotation cycling in our study ranged from 6 to 8 Nm. Despite the application of lower-than-physiologic torque, dowel migration still occurred.
Other technical variables, such as depth of insertion, angle of insertion, and dowel design may influence dowel migration rates but were held constant within our experimental model. All dowels placed in our study were inserted to a depth of 13 mm, which is the deepest setting allowed by the TruFUSE kit. Shorter depths of 10, 11, and 12 mm are possible but were not evaluated. Regarding the angle of insertion, all dowels were placed at the superior endplate of the L5 vertebral body along the direction of the joint. With respect to dowel design, we used a 5 mm TruFUSE tapered facet bone dowel. TruFUSE also offers a larger 7.5 mm dowel. Other manufacturers offer dowels with shapes such as a threaded design that may influence migration in a positive or negative fashion.
This study has several limitations. First, in a cadaveric study of an isolated motion segment (L4-L5), as with all cadaveric studies, the exact biomechanical environment of an in vivo test cannot be achieved because of the inability to replicate the effects of the torso musculature in the lab setting. Another flaw inherent to cadaveric testing lies in the variability among specimens. Despite the methods used in our study design to detect gross biomechanical abnormality, subtle differences among all spines cannot be accounted for and can alter stiffness outcomes within a small sample size of specimens. Second, our test only evaluated the biomechanical effects during pure moments. In vivo lumbar spines are subjected to motions in all planes and with varying amounts of load. Lastly, the fatigue testing to which the specimens were subjected, although within the standards of biomechanical testing, may not represent true physiologic movement: eg, people do not flex or rotate their lumbar spines 10,000 times in a day.
CONCLUSION
Facet dowels increase the stiffness of the motion segment to which they are applied and can be used in conjunction with laminectomy procedures to increase the stiffness of the joint. Dowel migration can occur after axial rotation movements, even under physiologic conditions. Hybrid TLIF or XLIF plus facet dowel constructs appear to result in significantly higher stiffness than noninstrumented constructs and may not result in dowel migration.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care and Medical Knowledge.
Footnotes
The authors have no financial or proprietary interest in the subject matter of this article.
- © Academic Division of Ochsner Clinic Foundation
REFERENCES
In this issue








{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.