
Abstract
Background Intracranial subdural empyema (ISDE) is a pyogenic infection located in the space between the dura and arachnoid mater. Early diagnosis, prompt initiation of antimicrobial therapy, and surgical drainage are essential to reduce morbidity and mortality. This case series analyzes the presentation and management of ISDE in Queensland, Australia, over a 10-year period.
Methods Thirty-six patients with ISDE were treated at Gold Coast University Hospital, Princess Alexandra Hospital, Townsville Hospital, and Royal Brisbane Hospital. The patients' medical records were analyzed to ascertain patient demographics, etiology, presentation, and management.
Results A slight male preponderance occurred in the cohort of 36 patients with ISDE. The most common source of infection was a neurosurgical procedure, followed by sinusitis and otogenic sources. Headache, fever, and altered sensorium were the most common clinical triad of symptoms, present in 19 (53%) patients. Craniotomy was performed as the initial surgical procedure in 28 (88%) of the 32 patients who required surgery. Seizure prophylaxis was given to 25 (69%) patients, with 8 (32%) of those patients having seizures during their hospitalizations despite this therapy. Five (14%) patients required readmission and a second craniotomy because of failed resolution of the ISDE.
Conclusion Altered sensorium, fever, vomiting, and headache should alert the clinician to the possibility of ISDE. A history of neurosurgery, sinusitis, otitis media, or skull trauma increases the likelihood of this differential. Management includes sensitive antibiotic therapy and surgical drainage. Compared with burr hole, craniotomy is associated with less recurrence of ISDE.
INTRODUCTION
Intracranial subdural empyema (ISDE) is a pyogenic infection localized within the space between the dura and arachnoid mater. It is a rare condition, accounting for 15%-20% of localized intracranial infections.1,2 Although its incidence is decreasing, ISDE can be difficult to diagnose because of its nonspecific presentation.3-6 The most common triad of symptoms is fever, headache, and vomiting.5,6 Improving patient outcomes is critically dependent on rapid diagnosis, prompt initiation of appropriate antimicrobial therapy, and early surgical drainage.5-8 ISDE is an important area of practice that constitutes a neurosurgical emergency and can be associated with significant morbidity and mortality caused by focal neurology and seizures.5,6,9 This study provides clinicians with useful information on the presentation and management of ISDE in Queensland, Australia.
METHODS
We performed a retrospective analysis of patients who were diagnosed with ISDE at all public neurosurgical departments in Queensland, Australia (Gold Coast University Hospital, Princess Alexandra Hospital, Townsville Hospital, and Royal Brisbane Hospital), between June 2001 and June 2011. At Gold Coast University Hospital, the Emergency Department Information System and surgical list databases were searched for patients diagnosed with ISDE. At Princess Alexandra Hospital, Townsville Hospital, and Royal Brisbane Hospital, the Hospital Based Clinical Information System database was searched for patients diagnosed with ISDE. The keywords subdural empyema, subdural abscess, and intracranial empyema were used in the searches. Of 315 potential patients, 36 were suitable for this study based on the diagnosis of ISDE after medical record review. The remaining 279 patients were excluded because they had another exclusive diagnosis such as intracranial abscess, extradural empyema, or subdural empyema in the spinal cord.
The Human Research and Ethics Committee approved this study as low risk. Data were deidentified and collated using a standardized, password-protected Microsoft Excel spreadsheet. Collected data included patient demographics, etiology, presentation, management, and outcome. All clinical features were regarded as present if they occurred before presentation to the hospital or during the hospital stay prior to the diagnosis of ISDE.
Data were analyzed in Microsoft Excel using univariate analysis. Descriptive statistics used were mean and percentage. Incidence was calculated by dividing the number of patients with ISDE from 2001-2011 by the person-years. Person-years were calculated by multiplying the average population in Queensland by the duration of the inclusion period (ie, 10 years).
RESULTS
Demographics
In Queensland, the incidence of ISDE over a 10-year period was 0.1 in 100,000 persons. In the patient cohort analyzed for this study, 20 (56%) were male and 16 (44%) were female. The mean and median ages of the patient sample were 46.1 years and 49.5 years, respectively (range 9-89 years).
Etiology
The most common source of infection was a neurosurgical procedure, occurring in 16 (44%) patients. Evacuation of a subdural hemorrhage was the most common procedure preceding ISDE, performed in 10 (28%) patients. Sinusitis was the second most common source of infection (28%). Otogenic sources were the third most common (14%) and included chronic otitis media and mastoiditis (Table 1). Other known sources were skull trauma and meningitis (Figure 1).
Source of Infection in Patients with Intracranial Subdural Empyema

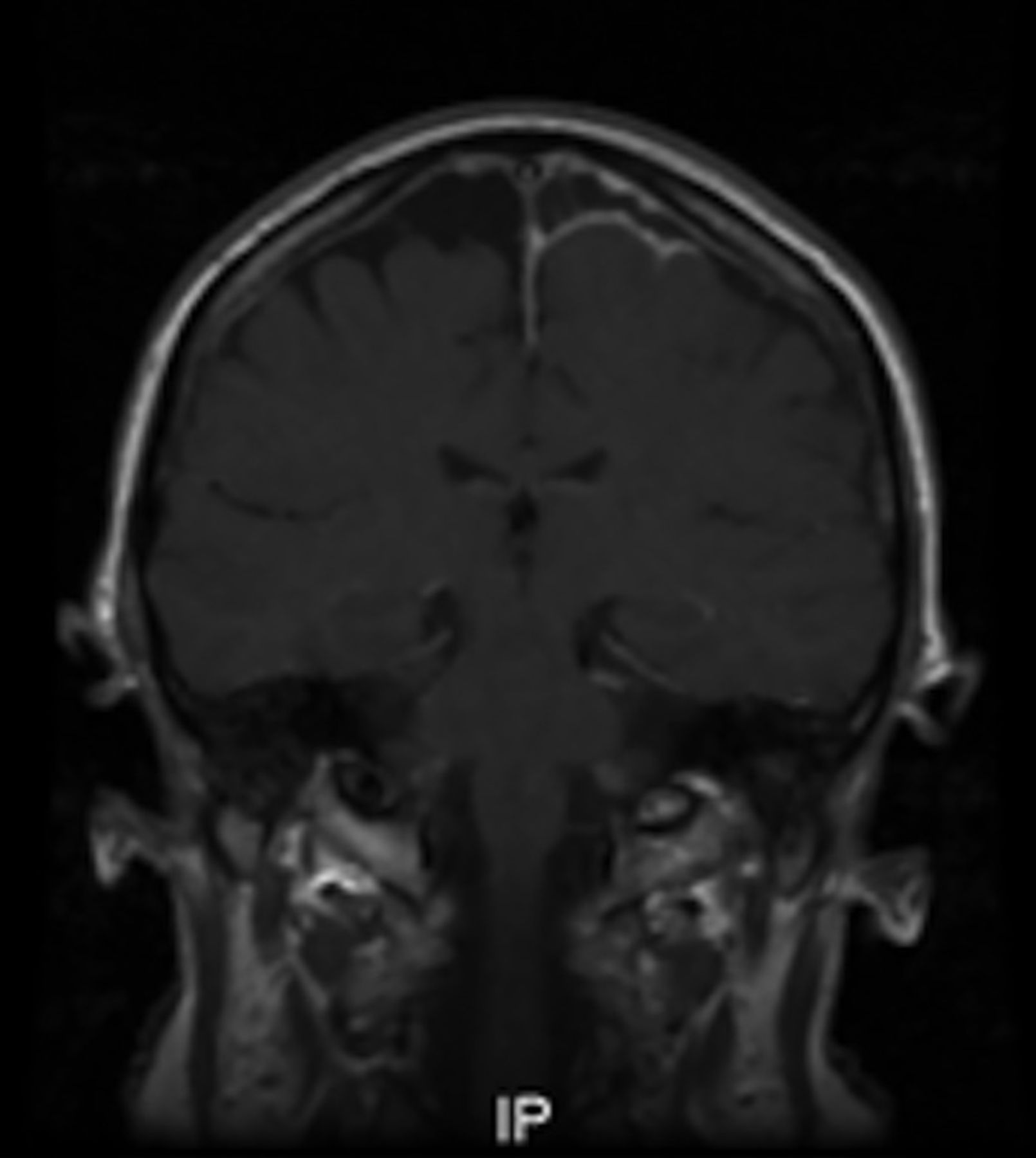
Coronal magnetic resonance imaging head scan with gadolinium shows a left parasagittal subdural empyema in a patient after meningitis.
Clinical Features
The most common clinical feature of ISDE was headache, followed by fever and altered sensorium (Table 2). This triad of headache, fever, and altered sensorium was present in 19 (53%) patients. The classic triad of headache, fever, and vomiting was present in 13 (36%) patients. Altered sensorium was seen in 24 (67%) patients. Of the patients with altered sensorium, 54% had Modified Glasgow Coma Scale (GCS) scores between 13-14, 25% had GCS scores between 9-12, and 21% had GCS scores ≤8 (on a 15-point scale in which 15 indicates full consciousness). A normal level of consciousness was seen in 12 (33%) patients (Table 3). Eight patients (22%) presented with seizures. Focal motor signs were found in 18 (50%) patients. The most common focal motor sign was contralateral limb weakness.
Clinical Features in Patients with Intracranial Subdural Empyema
Modified Glasgow Coma Scale Scores in Patients with Altered Sensorium
Organisms
Organisms were cultured from blood samples (n=28) or intraoperative swabs (n=32). Only 1 patient had a negative intraoperative swab. Multiple organisms were cultured in 7 patients. Of the patients who had blood cultures taken, only 2 had a positive result. The organisms differed based on the source of infection (Table 4).
Cultured Organisms from Patients with Intracranial Subdural Empyema
Diagnosis
Computed tomography (CT) scan of the head with contrast was utilized to diagnose ISDE in 27 (75%) patients. Ten patients underwent magnetic resonance imaging (MRI) with gadolinium to facilitate surgical planning or for follow-up. MRI was used to diagnose ISDE in 9 (25%) patients. The median time to diagnosis was 2 days.
The most common locations for ISDE were along the frontal and frontoparietal convexity (Table 5). Five patients had ISDE in multiple locations. Two patients had bifrontal convexity ISDEs, and 1 patient had 2 right frontoparietal convexity ISDEs (Figure 2). Four patients had an associated extradural abscess, and 1 patient had an associated intraparenchymal abscess.
Location of Empyema

Axial computed tomography head scan with contrast shows 2 subdural empyemas over the right frontoparietal convexity in a patient after microvascular decompression for trigeminal neuralgia.
Antibiotics
In our cohort, 32 (89%) patients received antibiotics along with surgical drainage. Four patients were managed conservatively with antibiotics alone. All patients were given a combination of antibiotics for broad coverage. Common combinations included ceftriaxone, gentamicin, and metronidazole, or benzylpenicillin, gentamicin, and metronidazole. For 14 (39%) patients, antibiotic regimes were altered once sensitivities were obtained. Antibiotic regimes were commonly changed to flucloxacillin, meropenem, or vancomycin because of patient sensitivities.
Prophylactic Anticonvulsants
Seizure prophylaxis was given to 25 (69%) patients with ISDE, but 8 (32%) of those patients had seizures during their hospitalizations despite the use of oral prophylactic anticonvulsants. Eleven (31%) patients did not receive prophylactic anticonvulsants; 2 (18%) of the patients who did not receive prophylactic anticonvulsants were started on anticonvulsants after the onset of seizures.
Surgery
Of the 32 patients who received an operation, the median time to surgery was 24 hours postdiagnosis. Craniotomy was the initial operation to drain the empyema in 28 (88%) patients who required surgery. Two (7%) of these patients had to undergo a second craniotomy during the same hospital admission because the empyema failed to resolve. Of the 4 patients who received burr hole washouts as the initial operation, 1 (25%) experienced clinical resolution and a good outcome; however, the infection failed to resolve in 3 (75%) patients, and they required a subsequent craniotomy. Two patients required external ventricular drains (EVDs) for hydrocephalus after drainage of their ISDEs, and 3 patients had an EVD prior to the ISDE for hydrocephalus during the previous surgery for tumor resection or skull trauma. One patient had a ventriculoperitoneal shunt from skull trauma prior to the hospital admission for ISDE.
Outcome
No mortalities were recorded in this case series during management or follow-up. Residual neurological deficits or seizures were seen in 21 (58%) patients. Eleven (31%) patients had motor deficits, and 3 (8%) patients had dysphasia at discharge from hospital. Nine (25%) patients reported seizures at follow-up appointments. Of these patients, 1 had both dysphasia and seizures, and 1 had both motor deficits and seizures.
Five (14%) patients required readmission and a second craniotomy because the ISDE failed to resolve. One patient was readmitted for intravenous antibiotics, 1 required cranioplasty, 1 required readmission for evacuation of a subdural hemorrhage at a later date, and 1 required readmission for evacuation of extradural empyema at a later date.
DISCUSSION
This study is the largest case series on ISDE in Australia, and it gives insight into the presentation and management of this disease compared to other geographical locations. This study is valuable for clinicians as patient outcomes are dependant on early diagnosis and prompt initiation of treatment.6,10 The demographics for ISDE in Queensland, Australia, are consistent with previous literature in that occurrence is rare and ISDE most often affects middle-aged patients with a slight male preponderance.2,3,5,6,11,12
Neurosurgical procedure was the most common source of infection (44%), followed by sinusitis (28%) and otogenic sources (14%). This finding differs from other studies, in which sinusitis and otogenic sources account for higher proportions of infection sources.12-17 The cause of our finding is likely multifactorial. First, the intracranial complications of sinusitis and otogenic infections have decreased in recent years with the use of broad-spectrum antibiotics.18,19 Additionally, neurosurgery is performed with increasing frequency, and the hospitals included in this study are all major neurosurgical referral centers.20 The most common neurosurgical procedure associated with ISDE in this study was drainage of a subdural hemorrhage, which has been reported in previous studies.21-24
The clinical features associated with ISDE are often nonspecific, making diagnosis difficult for clinicians.4-6 The signs and symptoms found in this case series are similar to those described in other studies.2-5,7,8,25,26 The most common triad of symptoms in this study was headache, fever, and altered sensorium, which differs from the classical triad of headache, fever, and vomiting more commonly reported in the literature.3,7,25 Our findings highlight the need for clinicians to have a high index of suspicion for ISDE in patients who present with any of the 4 most common symptoms in this study—headache, fever, altered sensorium, and vomiting—especially in those patients who have had a neurosurgical procedure, sinusitis, mastoiditis, or chronic otitis media.
In this patient series and in previous studies, operative swabs were vital to determine the causative organism and to target antibiotic therapy. Blood cultures rarely identify an organism because of the capsulated nature of the infection.3 The organisms associated with ISDE are variable and are dependent on the source of infection, with multiple organisms often present.3,27-29 Common organisms associated with neurosurgical operations are Staphylococcus aureus and Propionibacterium acnes.12,20,27 Streptococcus milleri and Fusobacterium necrophorum are common in patients with sinusitis, and Bacteroides fragilis and Staphylococcus aureus are common otogenic sources.3,6,30,31 Our findings are consistent with what has been reported in the literature.
CT head scans with contrast are commonly used as the initial investigation in patients with suspected ISDE because CT scans are readily available and results can be obtained rapidly.3,25,32 However, if CT is inconclusive, MRI with gadolinium should be performed.4,5,8,27
Management of ISDE includes empirical treatment with broad-spectrum antibiotics. A combination of penicillin or cephalosporin, metronidazole, and an aminoglycoside was commonly used in our case series, and this regime is supported by the literature.3-5,27 Antibiotic regimes were altered once sensitivities were obtained, in keeping with previous recommendations that advocate for sensitivity-guided medical therapy in patients with ISDE.11,27
Seizures are common in patients with ISDE, so most centers advocate for the use of prophylactic anticonvulsants.5,6,10,32-34 The majority of patients (69%) in this study were put on anticonvulsants following the diagnosis of ISDE, but 8 (32%) patients had seizures in the hospital, and 9 (25%) patients had seizures after discharge from hospital. Seizures remain a significant cause of morbidity.5,10,35 The seizure rate indicates the need for further studies on anticonvulsant therapy in patients with ISDE to reduce the incidence of this complication.
The surgical options available for patients with ISDE are craniotomy or burr hole, with craniotomy considered superior.2,3,8,11,25,36,37 In this case series, craniotomy had a lower ISDE recurrence rate than burr hole and was the definitive surgical treatment in the majority (86%) of cases. Benefits of craniotomy include partial excision of the wall of the abscess and the ability to leave the area of suppuration completely open.25 This study suggests that in patients with ISDE, craniotomy, rather than burr hole, should be the initial method of surgical drainage.
Limitations
The limitations of this study include the retrospective design and data collection being dependent on documentation in the medical records. Specific limitations associated with medical record review include chart ambiguity, omissions, illegibility, and data entry error. These limitations were minimized by using a simple, exact, nonambiguous data collection tool.
This study does not include the cases of ISDE managed in smaller hospitals and not referred to the neurosurgical units in this state, which we assume to be few. The incidence calculation is limited because it does not account for the population not in residence, patients who travel interstate for treatment, or the population abroad.
CONCLUSION
Subdural empyema is rarely seen in Queensland, Australia. Altered sensorium, fever, vomiting, and headache should alert clinicians to include ISDE in their differential diagnosis. A history of neurosurgery, paranasal sinus infection, otitis media, or skull trauma should guide clinicians to the source of the patient's infection. In suspected ISDE cases, empirical antibiotic therapy should be started and altered once sensitivities are obtained, ultimately proceeding to craniotomy as definitive therapy. Seizure prophylaxis is commonly used, although seizures can still occur, and further research into optimal seizure prophylaxis is required.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care, Medical Knowledge, and Practice-Based Learning and Improvement.
Footnotes
The authors have no financial or proprietary interest in the subject matter of this article.
- © Academic Division of Ochsner Clinic Foundation








{kind=link}
{kind=link}