
Abstract
Background Diffuse large B-cell lymphoma is the most common lymphoid neoplasm, accounting for approximately 25% of all non-Hodgkin lymphomas. Patients typically present with nodal enlargement, fever, weight loss, or night sweats. Extranodal extramedullary disease occurs in up to 40% of cases with the most common site of extranodal involvement being the gastrointestinal tract. However, diffuse large B-cell lymphoma can present in virtually any area, including the testes, bones, thyroid, salivary glands, tonsils, skin, liver, breasts, adrenals, kidneys, nasal cavity, paranasal sinuses, cervix, and central nervous system.
Case Report We present a unique case of atrial fibrillation and respiratory failure as an initial presentation of diffuse large B-cell lymphoma with cardiac and cavitary pulmonary involvement.
Conclusion The recent advances in chemotherapeutic options allow for and reinforce the importance of tailoring the chemotherapy regimen to the individual patient's unique presentation. In our patient, presentation included extensive intracardiac involvement resulting in arrhythmias, cavitary pulmonary nodules, and acute hypoxemic respiratory failure requiring ventilator support.
- Atrial fibrillation
- drug therapy–combination
- lymphoma–large B-cell–diffuse
- lymphoma–non-Hodgkin
- neoplasm
- respiratory insufficiency
INTRODUCTION
Diffuse large B-cell lymphoma is the most common lymphoid neoplasm, accounting for approximately 25% of all non-Hodgkin lymphomas.1 Patients typically present with nodal enlargement, fever, weight loss, or night sweats.2 Extranodal extramedullary disease occurs in up to 40% of cases, most commonly involving the gastrointestinal tract.3 However, diffuse large B-cell lymphoma can present in virtually any area, including the testes, bones, thyroid, salivary glands, tonsils, skin, liver, breasts, adrenals, kidneys, nasal cavity, paranasal sinuses, cervix, and central nervous system.4
Cardiac involvement by lymphoma is a relatively unusual presentation but has been seen in approximately 16% of patients with Hodgkin disease and 18% of patients with non-Hodgkin lymphoma (NHL) at autopsy.5 Lymphoma is the third most common malignant tumor of the heart at autopsy and usually occurs a median of 20 months after initial diagnosis; it is rarely seen on initial presentation.4 Prognosis with cardiac involvement is extremely poor. We present a unique case of atrial fibrillation and respiratory failure as an initial presentation of diffuse large B-cell lymphoma with cardiac and cavitary pulmonary involvement.
CASE REPORT
A 47-year-old Caucasian male with hypertension and a history of seizure disorder presented with a 1-day history of acute onset of shortness of breath, palpitations, and chest pain. Electrocardiogram revealed atrial fibrillation with rapid ventricular response. The patient was treated with diltiazem and amiodarone drips with improved heart rate control. A computed tomography (CT) scan of the chest revealed no evidence of pulmonary thrombus but showed a 7 × 6 × 4 cm mass in the inferior right hilar area that extended into the mediastinum and compressed the cavoatrial junction and the left atrium at its junction with the pulmonary veins (Figure 1). The tumor appeared to invade the bronchus intermedius with an associated postobstructive infiltrate. Multiple 2- to 4-cm cavitary masses were distributed throughout both lungs. An echocardiogram with color-flow Doppler revealed a normal left ventricular ejection fraction and a large right atrial mass with a small pericardial effusion.

Computed tomography scan revealing large right hilar/infrahilar mass extending to the mediastinum and posterior right aspect of the heart contiguous with soft tissue density involving the right atrium and ventricle, cavoatrial junction, and distal superior vena cava region. This mass caused marked narrowing of the right atrium and cavoatrial junction.
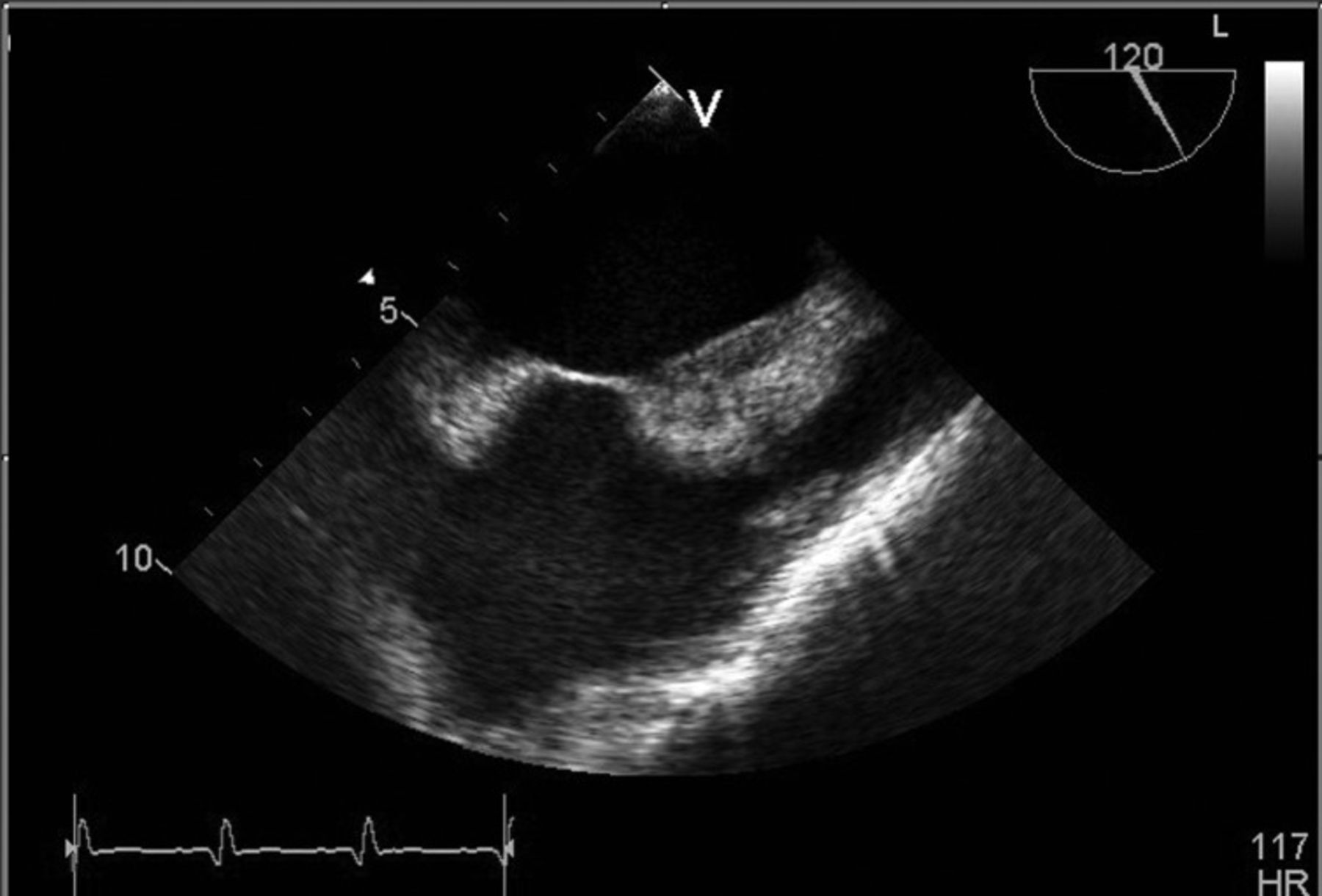
The patient underwent a diagnostic fiber-optic bronchoscopy with bronchoalveolar lavage and endobronchial biopsy. The bronchoscopy revealed an endobronchial mass occluding the right middle and lower lobe. The biopsy was negative for malignancy. Three days later, the patient again developed palpitations. His heart rate was 160-220 bpm, and he became hypotensive. He was emergently cardioverted, after which his heart rate was approximately 50 bpm with a junctional rhythm. The patient was intubated at that time. A repeat CT scan of the chest showed no pulmonary embolism but revealed enlarging soft tissue mass and an increase in the cavitary pulmonary nodules compared to the scan 1 week prior. Flexible and rigid bronchoscopies with biopsy were performed by cardiothoracic surgery. The patient was briefly extubated but required reintubation secondary to acute hypoxemic respiratory failure and atrial fibrillation. Histopathology revealed findings consistent with diffuse large B-cell lymphoma. The large atypical lymphocytes were positive for CD20, BCL-2, BCL-6, MUM-1, and Ki-67 of 99%. A transesophageal echocardiogram showed multiple infiltrative masses consistent with lymphoma. The right atrium revealed multiple echo-dense masses predominantly infiltrating the entire right atrial wall and atrial septum, as well as masses lining the epicardium that could be seen within the pericardial space. No evidence of a thrombus was found, and the patient had a normal left ventricular ejection fraction (Figure 2).
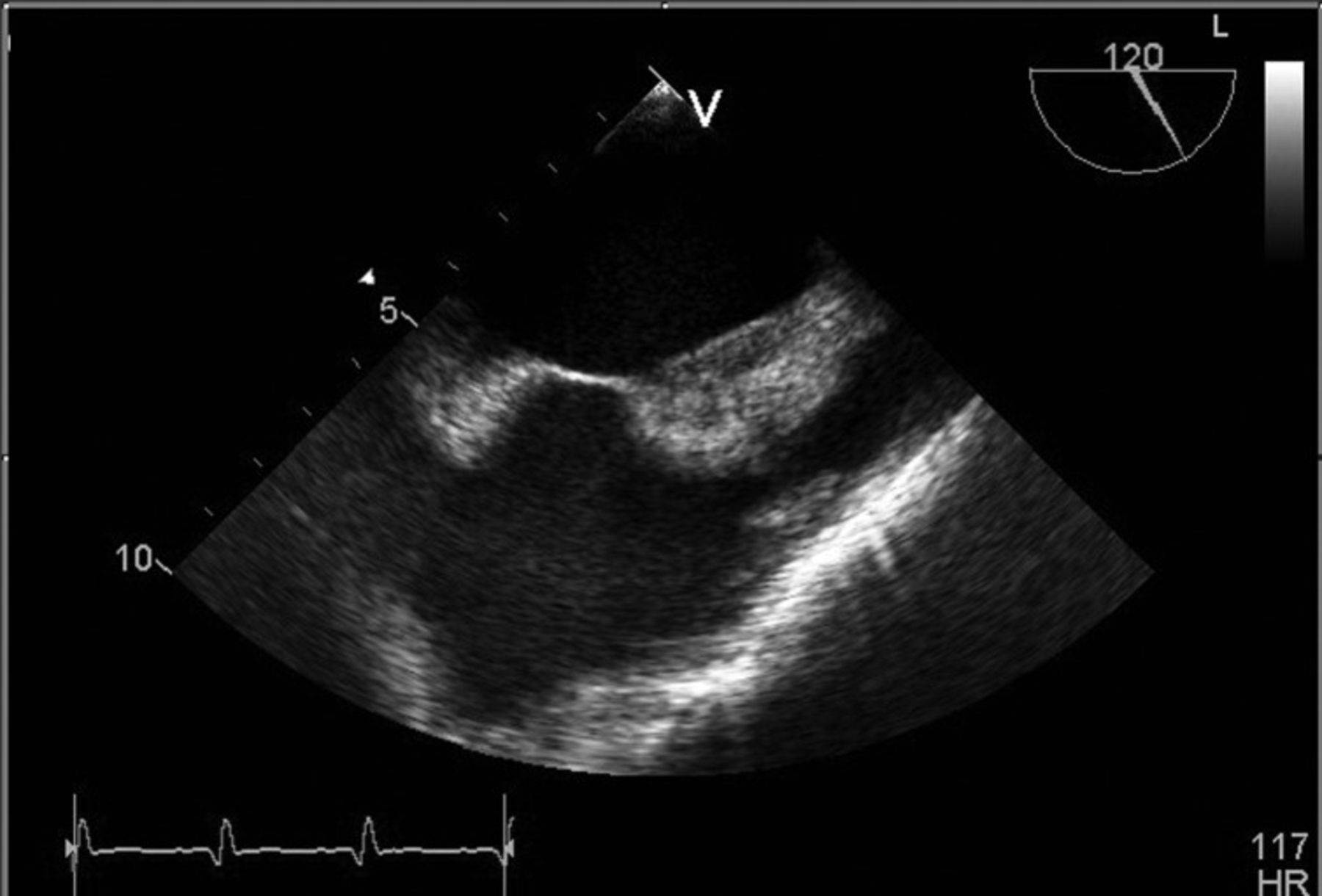
Transesophageal echocardiogram reveals right atrium with multiple echo-dense masses predominantly infiltrating the entire right atrial wall and atrial septum.
While on the ventilator in the intensive care unit, the patient underwent 1 cycle of chemotherapy, including methylprednisolone 100 mg administered daily by intravenous infusion on days 1-5, cyclophosphamide 650 mg/m2 on day 1, etoposide 70 mg/m2 daily on days 1-3, vincristine 1 mg on day 1, and rituximab 375 mg/m2 on day 1. Doxorubicin was not used because of cardiac involvement and concern for cardiac toxicity. The patient tolerated chemotherapy well without evidence of tumor lysis. He was started on granulocyte colony-stimulating factor on day 4 and Pneumocystis carinii pneumonia prophylaxis with pentamidine, as he was allergic to sulfonamide. The patient was extubated on day 7 without further complications, and he was discharged from the hospital on day 15 in stable condition without oxygen with cardiology and oncology follow-up. He has currently completed 6 cycles of rituximab, cyclophosphamide, vincristine, etoposide, and prednisone. A positron emission tomography scan at the end of 4 cycles of chemotherapy revealed a complete response with no abnormal hypermetabolic focal activity identified.
DISCUSSION
Intracardiac lymphoma was previously thought to be rare but is now being reported with increased frequency.6 Thirty-five cases of primary cardiac non-Hodgkin lymphoma had been reported as of 2008, with 22 of these cases being diffuse large B-cell lymphoma.7 According to the current literature, secondary involvement of the heart by lymphoma varies widely from 8.7% to 20%.8 The majority of tumors occur on the right side of the heart. Pulmonary cavitation has also been reported infrequently and is more commonly seen in Hodgkin lymphoma. In 1 series of 27 cases of non-Hodgkin lymphoma, 2 of 14 patients with nodular disease developed cavitary lesions.9 With cavitary lesions, tuberculosis, fungal infections, or other infectious etiology must be ruled out prior to the administration of cytotoxic chemotherapy. Extranodal lymphomas are being seen more frequently with acquired immunodeficiencies, such as human immunodeficiency virus, or after bone marrow and solid organ transplantation.6
Multiple single case reports have discussed management of patients with intracardiac lymphoma, but because of a lack of data, no definitive guidelines exist. Based on a review of the literature, systemic chemotherapy appears to be the only therapy that has been shown to be effective.10 Cases of ventricular wall rupture or perforation have occurred in response to chemotherapy, but only 1 case of prophylactic pericardial patching has been reported where significant transmural involvement was evident.11 Unless the tumor progresses despite chemotherapy, radiation has not generally been considered a therapeutic option because of the risk of pericarditis, cardiomyopathy, conduction defects, and coronary artery disease. Surgical options have also not been recommended.
CONCLUSION
The recent advances in chemotherapeutic options allow for and reinforce the importance of tailoring the chemotherapy regimen to the individual patient's presentation. In our patient, presentation included extensive intracardiac involvement resulting in arrhythmias, cavitary pulmonary nodules, and acute hypoxemic respiratory failure requiring ventilator support. With the cardiac comorbidities, we felt it necessary to avoid anthracyclines. Alternative chemotherapy regimens have been studied for older patients or those with significant comorbidities. For example, for patients older than 60 with newly diagnosed diffuse large B-cell lymphoma, the German lymphoma study group routinely administers low-dose prephase chemotherapy consisting of vincristine and prednisone for 1 week prior to standard multiagent cytotoxic chemotherapy.12 This therapeutic option could be considered in clinically stable patients with high-risk cardiac involvement to possibly prevent cardiac rupture, as has been seen in previous case reports. However, given our patient's respiratory failure, an expedient response was needed, so the regimen used was felt to be the most effective combination with less chance of cardiac toxicity.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care and Medical Knowledge.
Footnotes
The author has no financial or proprietary interest in the subject matter of this article
- © Academic Division of Ochsner Clinic Foundation








{kind=link}
{kind=link}