
Abstract
Background Renal medullary carcinoma (RMC) is an aggressive form of non–clear cell kidney cancer that typically affects young adults and is almost exclusively associated with sickle cell trait. Typical RMC patients tend to be young black males (2:1 male to female predominance) with sickle cell trait who present with pain and hematuria and are found to have metastatic disease at diagnosis. Prognosis is extremely poor, with a mean survival of less than a year in most cases.
Case Report We present a case illustrative of many of the classic findings of RMC. A 25-year-old female with a past medical history of sickle cell trait presented to the emergency room with right-sided flank pain. Initially, a computed tomography (CT) scan showed only a benign-appearing cystic lesion 4.5 cm in diameter in the right kidney. Six months later, the patient re-presented with hematuria, lightheadedness, and dizziness. A repeat CT scan showed that the renal cyst had enlarged to 5.6 cm. The patient underwent a decortication and fulguration procedure that revealed malignancy in the wall of the cyst. She was given a series of treatments but experienced progressive disease and passed away 2 years and 8 months after metastatic diagnosis.
Conclusion Neither systemic therapy nor radiation therapy has been found to be particularly efficacious in the treatment of RMC. As the underlying biologic mechanisms of RMC are further elucidated on a basic science level, we expect new translational research opportunities will emerge and novel treatment options will be developed for this rare and dismal disease.
INTRODUCTION
An estimated 65,150 cases of renal cell carcinoma (RCC) were diagnosed in the United States in 2013.1 About 70%-80% of these tumors are classified as clear cell RCC and the remainder are non–clear cell RCC. Over the last 15 years, as the pathophysiology of non–clear cell RCC has been increasingly studied, several distinct subtypes have been recognized. These heterogeneous diseases have varying clinical, pathologic, and molecular characteristics.2
One type of non–clear cell RCC that has been more recently recognized is renal medullary carcinoma (RMC). RMC is an aggressive form of kidney cancer first described by Davis et al in 1995.3 The disease almost always affects young patients with sickle cell trait and has been described as the seventh sickle cell nephropathy (the other sickle cell nephropathies are gross hematuria, papillary necrosis, nephrotic syndrome, renal infarction, inability to concentrate urine, and pyelonephritis).4 We present a case illustrative of many of the classic findings of RMC and provide an up-to-date review.
CASE REPORT
A 25-year-old female with a past medical history of sickle cell trait presented to the emergency room with right-sided flank pain. Initially, computed tomography (CT) scan showed only a benign-appearing cystic lesion 4.5 cm in diameter in the right kidney. Six months later, the patient re-presented with hematuria, lightheadedness, and dizziness. Physical examination was benign. Laboratory tests revealed a hematocrit of 21%. Urinalysis was consistent with hematuria. A repeat CT scan showed that the renal cyst had enlarged to 5.6 cm. The patient underwent a decortication and fulguration procedure that revealed malignancy in the wall of the cyst. Two months later, she underwent a right nephrectomy that revealed a high-grade (Fuhrman grade 3) medullary carcinoma with venous invasion. Positive extension into the renal vein was noted. All surgical margins were clear, and sampled lymph nodes were all negative for malignancy. No lymphovascular invasion was present. The tumor exhibited extensive areas of necrosis and hemorrhage.
The patient had no evidence of further disease and observation was recommended, as no known adjuvant therapy for RCC currently exists. She presented to the University of Texas MD Anderson Cancer Center 2 months later, and baseline imaging revealed a new right retrocaval lymph node measuring 1.9 × 1.6 cm. Also, at the inferior aspect of the right lobe of the liver, a small soft tissue attenuation measuring approximately 1.5 cm in greatest dimension was noted, as well as multiple bilateral metastatic lung nodules, metastatic mediastinal lesions, left hilar lymphadenopathy, and paratracheal masses (See Figures 1-3). She was initially started on protocol with full-dose 50 mg sunitinib by mouth daily for 4 weeks on and 2 weeks off. She required dose reduction to 37.5 mg daily after 5 months because of grade 3 hand-foot syndrome. She remained on sunitinib for 6 months until progressive disease (PD) was noted, with a new nodule in the right adrenal gland, new nephrectomy bed metastases, and an increase in size of mediastinal lymphadenopathy and left hilar lymphadenopathy.

Axial computed tomography scan of the chest showing a large left hilar mass. Images of the patient's primary tumor are not available, as she presented to our institution at recurrence.
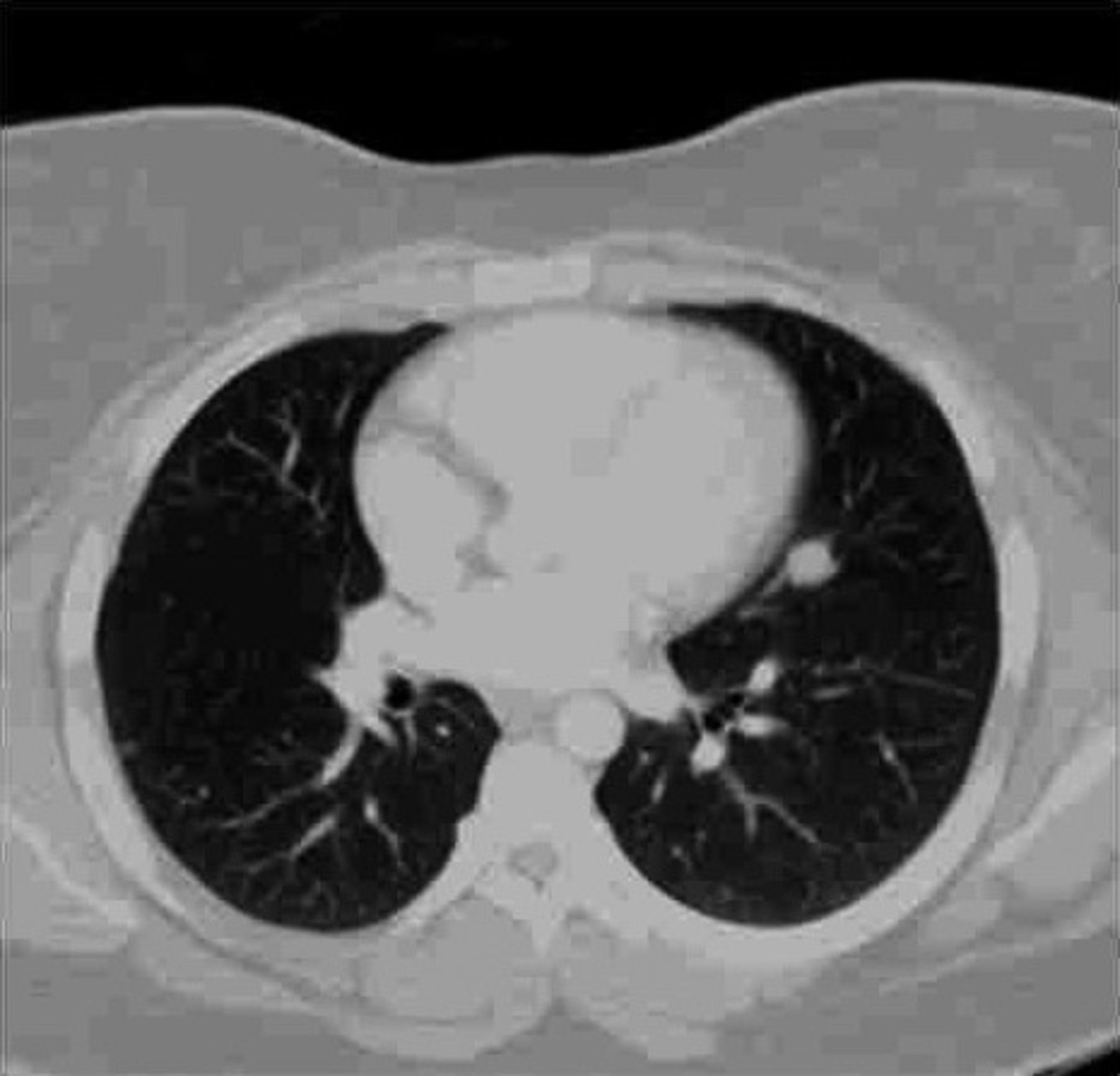
Axial computed tomography scan of the chest showing several central masses in the left lung and numerous smaller peripheral nodules in the right lung.
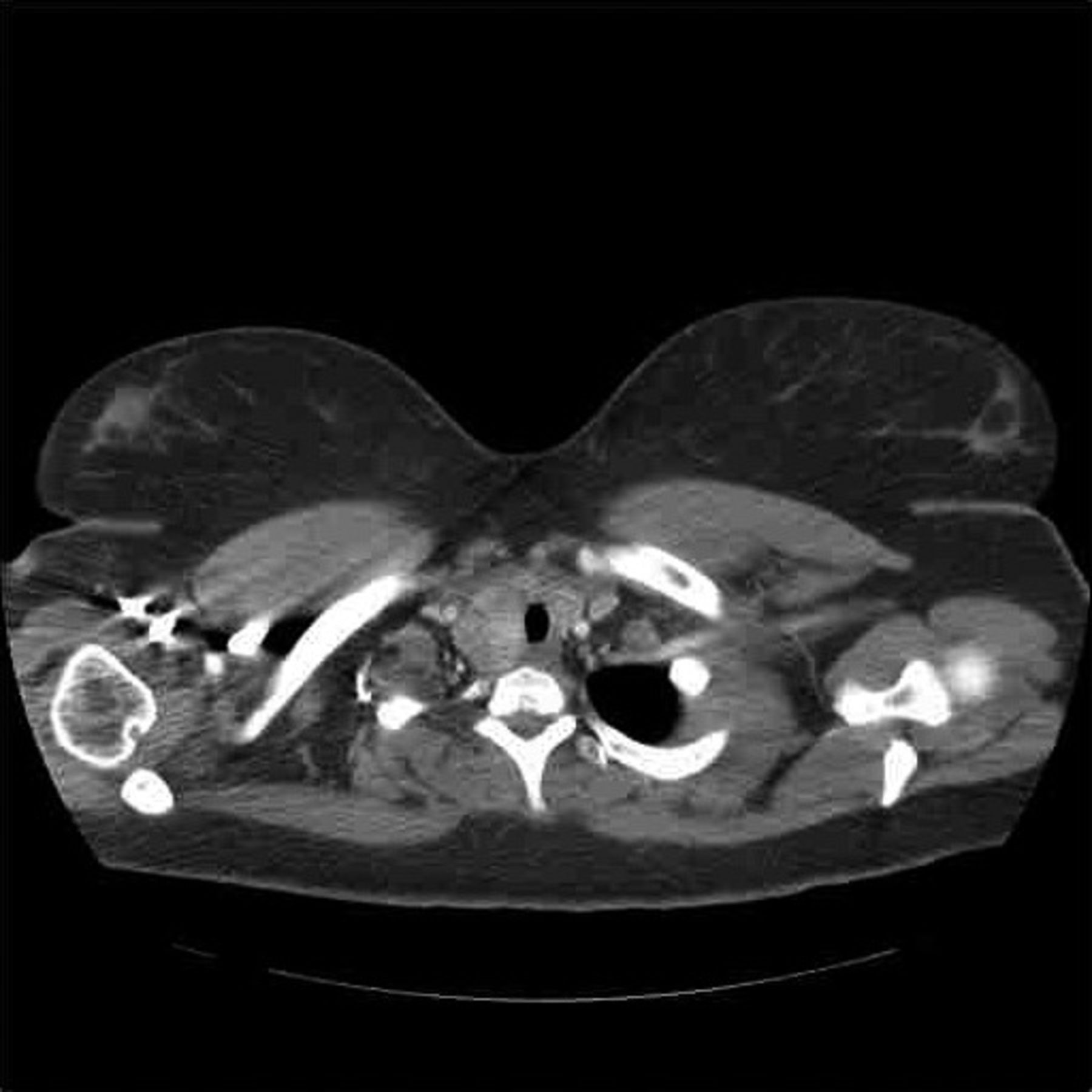
Axial computed tomography scan of the chest showing prominent paratracheal lesions.
She was then given a lead-in course with bevacizumab alone followed by bevacizumab with cisplatin and gemcitabine. She underwent 5 cycles of bevacizumab, cisplatin, and gemcitabine until PD was noted in her liver and bones. At this point, the patient was started on targeted therapy with everolimus, a mammalian target of rapamycin (mTOR) inhibitor. After 3 months, the patient had PD in the lungs and intrathoracic lymph nodes, and her treatment was changed to dose-dense MVAC (methotrexate, vinblastine, doxorubicin, and cisplatin), a regimen typically given for bladder cancer. She was treated with 2 cycles of dose-dense MVAC but developed tinnitus, requiring discontinuation of this regimen. Her therapy was then switched to doxorubicin and gemcitabine. Her disease remained stable for 7 months. She was then switched to bortezomib after receiving a cumulative doxorubicin dose of 660 mg/m2. Bortezomib was discontinued after 3 months due to PD. She was then started on carboplatin and paclitaxel. This treatment was discontinued after 3 months because of progressive thrombocytopenia. She was then started on bevacizumab and capecitabine, but after 2 months, she passed away because of PD. The total time span from the date of her metastatic disease diagnosis to the time of death was 2 years, 8 months, and 19 days.
DISCUSSION
Since Davis et al published the original description of RMC, more than 150 cases have been reported, confirming the clinical and epidemiological associations. Patients with RMC tend to be young with a median age of 19-22 years. Patients are almost always of black race (although RMC has been reported in Hispanics/Brazilians and a few Caucasians).5 Nearly all RMC patients have sickle cell trait or, rarely, sickle cell disease.
In adults, a 2:1 male-to-female ratio has been observed in patients with RMC. In children, the male predominance is even greater. Initial clinical presentation varies, but most patients present with symptoms; pain and hematuria are the most common. The right kidney is the affected kidney in more than 75% of cases.6 Metastasis at presentation is extremely common. The most common sites of metastases are the regional lymph nodes, adrenal glands, lung, liver, inferior vena cava, and peritoneum.7
Pathologically, RMC is a malignant epithelial tumor, arising from the collecting duct epithelium. Grossly, these tumors tend to be solitary grayish-white masses with prominent necrosis and hemorrhage. Microscopically, RMC tumors tend to be infiltrative, encompassing solid sheets of poorly differentiated carcinoma. Poorly formed vacuoles can also be seen, although a variety of microscopic patterns can be seen in individual specimens. Solid, reticular, tubular, trabecular, cribriform, and micropapillary architecture have all been described, as has sarcomatoid morphology. Often inflammatory cells, especially neutrophils and lymphocytes, infiltrate the tumor tissue. RMC tumors usually express cytokeratin AE1/AE3, low molecular weight cytokeratin, vimentin, hypoxia-inducible factors (HIF), and vascular endothelial growth factor (VEGF). Variability in the expression rate of high molecular weight cytokeratin is common.5,8
RMC is a highly aggressive cancer with an extremely poor prognosis. Mean survival time of less than 1 year is seen in most cases. Treatment is difficult. Neither chemotherapy nor radiation therapy has been found to be particularly efficacious. In a review of 20 cases from 4 major institutions over the last decade, Tannir et al found that targeted therapy has low efficacy when used as monotherapy.9 Cytotoxic chemotherapy is a mainstay of treatment, but even this modality provides only modest short-term palliation, with most patients dying within a year of diagnosis.9 A variety of chemotherapies has been tried in the past, including cyclophosphamide, doxorubicin, cisplatin, topotecan, methotrexate, and vinblastine. Currently, however, no regimen has significantly improved outcomes.10
As treatment options are few, several researchers have sought new targets of therapy in RMC. Albadine et al, for example, performed immunoexpression analyses of RMC tissue and found that topoisomerase II alpha was overexpressed in 11 of 13 (85%) RMC cases.11 These authors suggested therefore that topoisomerase II might potentially be an efficacious molecular target for future trials. Likewise, Schaeffer et al showed increases of topoisomerase II in all 4 cases they analyzed by whole-genome expression, and they further reported a case of metastatic RMC in which a complete response was achieved for 9 months using topoisomerase II-inhibitor therapy.12
Some renal medullary carcinomas have been associated with the absence of INI1 expression, a factor in the adenosine triphosphate-dependent chromatin-modifying complex. This genetic condition is also seen in renal rhabdoid tumors. An absent INI1 does not appear to predict rhabdoid histopathology, but in RMC, it is associated with more aggressive tumor behavior.13
Anaplastic lymphoma kinase (ALK) receptor tyrosine kinase rearrangement has been reported in RMC. Mariño-Enríquez et al reported a case of RMC in which they found a t(2;10)(p23;q22) chromosomal translocation associated with a novel ALK oncoprotein that had the cytoskeletal protein vinculin fused to the ALK kinase domain.14 Their report suggests a rationale for studying the treatment of RMC with targeted ALK inhibitors.15
Kondagunta et al conducted a phase 2 trial of bortezomib in metastatic RCC.16 One patient in this trial had metastatic RMC. The patient in this study received intravenous bortezomib at 1.3 mg/m2 on a twice-weekly schedule for 2 weeks followed by 1 week without treatment, continuing for a total of 7 months of bortezomib therapy. The patient achieved a complete remission and remained without evidence of disease after more than 27 months of follow-up.16 Bortezomib, a drug approved for the treatment of multiple myeloma and mantle cell lymphoma, targets the 26S proteasome of the ubiquitin-proteasome degradation system. In normal cells, the proteasome degradation system regulates protein expression and function by degradation of ubiquitinylated proteins. The system also clears abnormal or misfolded proteins from the cell.
Despite the lack of available prospective evidence, we currently use both targeted therapies and cytotoxic chemotherapy in the treatment of RMC. Our patient was treated with trials of both a VEGF-targeted tyrosine kinase inhibitor (sunitinib) and an mTOR inhibitor (everolimus), as well as various cytotoxic chemotherapy regimens. We also treated her with bortezomib based on the Kondagunta data and used the angiogenesis inhibitor bevacizumab both as a single-agent therapy and in combination with cytotoxic chemotherapy.
Our experience in this case mirrors that of other practitioners, sequencing through multiple modalities of systemic therapy in an attempt to achieve efficacy for the individual patient. Hopefully, improved understanding of the underlying biologic mechanisms of this rare disease will provide guidance for future therapies.
CONCLUSION
RMC is a rare and aggressive form of kidney cancer found almost exclusively in patients with sickle cell trait. Treatment options are limited, as most standard therapies have not been found to be efficacious in RMC. Currently no open clinical trials are enrolling only patients with RMC. However, a few trials are enrolling patients with various forms of non–clear cell kidney cancer, which can include patients with RMC. Researchers continue to explore the molecular drivers of this rare disease, but few clinical correlations have been made. As the underlying biologic mechanisms of RMC are further elucidated on a basic science level, we expect new translational research opportunities will emerge and novel treatment options will be developed for this rare and dismal disease.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care and Medical Knowledge.
Footnotes
The authors have no financial or proprietary interest in the subject matter of this article.
- © Academic Division of Ochsner Clinic Foundation








{kind=link}
{kind=link}
{kind=link}