
Abstract
Background Amyloidosis of the breast is an unusual diagnosis. Overall, only 2 major case series have been published in the literature since the time amyloidosis was first reported in 1973, highlighting the rare nature of this disease. Clinically, the patient may present with a breast mass or simply increased breast density and skin thickening. As such, amyloidosis may mimic the appearance of a number of pathologies, both benign and malignant.
Case Report We report a single case of a patient who presented with a breast mass and was ultimately diagnosed with primary amyloidosis of the breast. We also present a review of the literature to date.
Conclusion The main treatment for primary amyloidosis of the breast is surgical removal, most often accomplished with breast conservation via lumpectomy. In performing the lumpectomy, the goal should be to obtain negative surgical margins; however, no strong data exist to suggest that such lesions would recur with a microscopically positive margin.
INTRODUCTION
Amyloidosis of the breast is a rare entity, with only 2 major case series reported in the nearly 40 years since it was first reported in 1973.1 Amyloidosis is the extracellular deposition of insoluble beta-pleated fibrillar proteins.2 It may be localized or systemic, with the isolated involvement of the breast seldom reported. Staining for amyloid protein with Congo red reveals a characteristic apple-green birefringence under polarized light.3 Amyloidosis of the breast can distribute in a periductal, perivascular, or intralobar pattern; can create a foreign body–like reaction with infiltration of multinucleated giant cells; and can have an affinity for calcium.2 Clinically, the patient may present with a breast mass or simply with increased breast density and skin thickening.4 Radiographic imaging reveals a wide variety of mammographic and ultrasound findings, including similar patterns of ductal carcinoma in situ and fibrocystic change.4 As such, amyloidosis may mimic the appearance of a number of pathologies, both benign and malignant. However, more commonly, amyloidosis of the breast is a manifestation of an overall systemic disorder coexisting in the presence of systemic amyloidosis or a hematologic malignancy, mandating a thorough evaluation of the patient for these disorders.5,6
CASE REPORT
A 52-year-old African American female undergoing her regularly scheduled screening mammogram was found to have a new questionable area of focal asymmetry within the left breast. The mammogram was given an overall Breast Imaging-Reporting and Data System (BI-RADS) category 3 assessment (on a scale of 0-6), with a 6-month follow-up of this area recommended. The follow-up mammogram revealed an evolving mass in the same area, measuring 2.0 × 3.0 × 1.5 cm by both mammogram and ultrasound and considered a BI-RADS category 4 abnormality with biopsy recommended (Figure 1). The patient underwent an ultrasound-guided core biopsy, with the final pathology revealing amyloidosis with a lymphoplasmacytic infiltrate surrounding the breast ducts and some blood vessels.

A: Mammogram with craniocaudal view of the breast with needle guidewire in place just prior to operative procedure. The previously placed core biopsy clip is visible within the mass. B: Medial-lateral view of the breast with the needle guidewire placed. C: Imaged lumpectomy specimen performed intraoperatively, showing complete gross removal of the mass, core biopsy clip, and guidewire.
Initial staining for amyloid protein was performed with Congo red dye and revealed a characteristic apple-green birefringence that represents a positive finding for amyloid within the specimen (Figure 2). No evidence was found of breast cancer or other breast pathology; the associated immunohistochemical analysis revealed both kappa and lambda staining (10:1 kappa to lambda ratio). The patient was evaluated first by a medical oncologist, and a series of studies did not reveal any significant findings of amyloidosis. Bone marrow biopsy revealed normocellular bone marrow that was negative for plasma cell dyscrasia on flow cytometric analysis and negative for the presence of amyloid. Serum protein electrophoresis revealed a polyclonal increase in the gamma region. With no clinical symptoms reported and no evidence of systemic amyloidosis, the patient was seen by a surgical oncologist for further evaluation and possible removal of this breast mass. The patient subsequently underwent a needle-localized lumpectomy of this mass (Figure 3), and the final pathology revealed an amyloidoma with surrounding margins of breast parenchyma containing interstitial fibrosis, fibrocystic change, and periductal chronic inflammation (Figure 4). No evidence of malignancy was found and all of the surgical margins were negative.

The amyloid material is positive for staining with Congo red dye, revealing the characteristic apple-green color and birefringence under polarization microscopy (100× magnification); arrows indicate some of the larger areas of apple-green color.

Gross pathologic cross-section of the lumpectomy specimen revealing a slightly yellow, somewhat rubbery mass with some surrounding breast tissue.

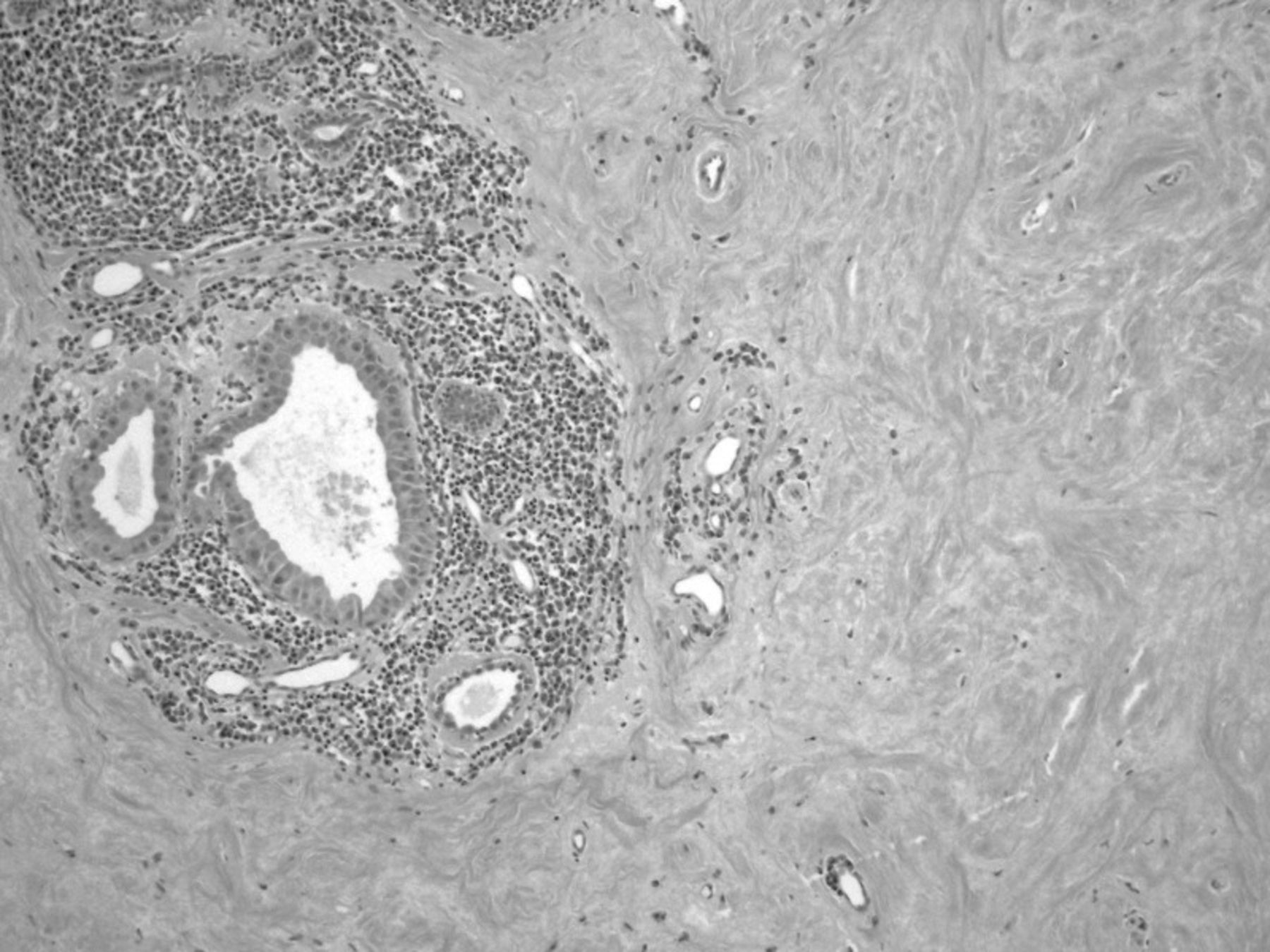
Standard hematoxylin and eosin histologic section of the lesion showing under low power the amyloid material in the breast, apocrine metaplasia, and periductal lymphoplasmacytic infiltration.
DISCUSSION
The deposition of insoluble protein characterized by systemic amyloidosis can interfere with physiological function. The clinical manifestations of amyloidosis are determined by the location of deposition.7 Systemic amyloidosis occurs when a monoclonal population of plasma cells generates excess amyloidogenic immunoglobulin light chains. In 75% of cases, the fibrillar deposits of systemic amyloidosis are composed of monoclonal lambda light chain proteins.7,8 In the remaining cases, protein deposits are products of kappa-restricted plasma cell clones. Kappa light chains have been described more frequently than lambda light chains with respect to amyloidosis of the breast.2 The incidence of systemic amyloidosis is 4.5 per 100,000, or approximately one-tenth the incidence of multiple myeloma.7
Primary breast amyloidosis is rare; however, it will typically present in women between the ages of 43 to 86 years old. Recent case reports have described instances of amyloidosis coexisting with breast cancer.2,4,9,10 Patients with breast amyloidosis are typically without clinical symptoms, with the first findings often noted on mammography or ultrasound. A minority of patients may present with a painless palpable mass or possibly a localized area of skin thickening, edema, or erythema.2 Primary amyloidosis of the breast is most often unilateral, but bilateral involvement has been reported.2,11-16
Although we describe a case of primary amyloidosis of the breast, the condition is most commonly associated with systemic amyloid involvement, manifesting outside of the breast in other parts of the body.2,11-16 Others have described amyloidosis as distinct lesions or occasionally as intermixed with breast cancer, and several different histologies have been reported, such as tubular carcinoma, invasive ductal carcinoma with extensive intraductal components, and invasive lobular carcinoma.10 Additional reports have included pathologies such as localized breast amyloidosis secondary to underlying extranodal Castleman disease, osseous metaplasia, and giant cell reaction.17,18 Other case reports have described isolated amyloidosis, or amyloidomas, of the lungs, larynx, urinary bladder, and heart.19-22
A recent review of 40 cases of breast amyloidosis over a 16-year period at the Mayo Clinic demonstrated an association with systemic amyloidosis in nearly 50% of all patients.5 Hematologic malignancies were also found in association with breast amyloidosis in a similar percentage of patients.5 As part of the systemic form, breast amyloid is frequently found as a late presentation. A case series by Charlot et al found that localized amyloidosis of the breast represented 0.5% of all the patients referred to the amyloid treatment center.23
CONCLUSION
The main treatment for primary amyloidosis of the breast is surgical removal, most often accomplished with breast conservation via lumpectomy. No role exists for associated examination of the draining nodal basin unless the final pathology reveals a concomitant breast cancer. In performing the lumpectomy, the goal should be to obtain negative surgical margins; however, no strong data exist to suggest that such lesions would recur with a microscopically positive margin. In this case, we were able to achieve negative margins. Adjuvant radiation therapy appears to be unnecessary. Postoperative management consists of periodic physical examination with a unilateral mammogram at 6 months to establish a baseline study. If this mammogram reveals postsurgical change and scar tissue, the patient can safely return to yearly bilateral screening mammograms.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care and Medical Knowledge.
Footnotes
The authors have no financial or proprietary interest in the subject matter of this article.
- © Academic Division of Ochsner Clinic Foundation
REFERENCES
In this issue








{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.