
INTRODUCTION
We describe the case of a child who presented with right eye swelling who was subsequently found to have a large soft tissue mass filling the sphenoid sinus, nasopharynx, and posterior right nasal fossa.
HISTORY
A 9-year-old boy presented with right eye swelling. He had also experienced 1 recent episode of epistaxis. Four years previously, he had been diagnosed with Langerhans cell histiocytosis (LCH) that was resected from the right frontal bone without local recurrence. Given the patient's history of LCH, a repeat head computed tomography (CT) scan was ordered. The neuroradiologist identified a lesion in the sphenoid sinus extending below the skull base, so the CT scan was extended through the mandible to cover the lesion. The patient was referred to otolaryngology, and he received magnetic resonance imaging (MRI) followed by cerebral angiogram with embolization prior to surgical resection.
RADIOGRAPHIC APPEARANCE AND TREATMENT
CT and MRI demonstrated a large soft tissue mass filling the sphenoid sinus, nasopharynx, and posterior right nasal fossa. The mass displaced the posterior wall of the right maxillary sinus anteriorly as it extended through the sphenopalatine foramen, widening the pterygopalatine fossa, and then entered the soft tissues of the inferotemporal fossa (Figures 1 and 2). MRI clearly demonstrated superior extension through the orbital apex and inferior orbital fissure to the right cavernous sinus (Figure 3). The mass eroded the right pterygoid bone and posterior wall of the right maxillary sinus. The location of the mass and pattern of spread were highly characteristic of a juvenile nasopharyngeal angiofibroma (JNA). Because the patient had a history of LCH, this diagnosis was also considered as a differential possibility.
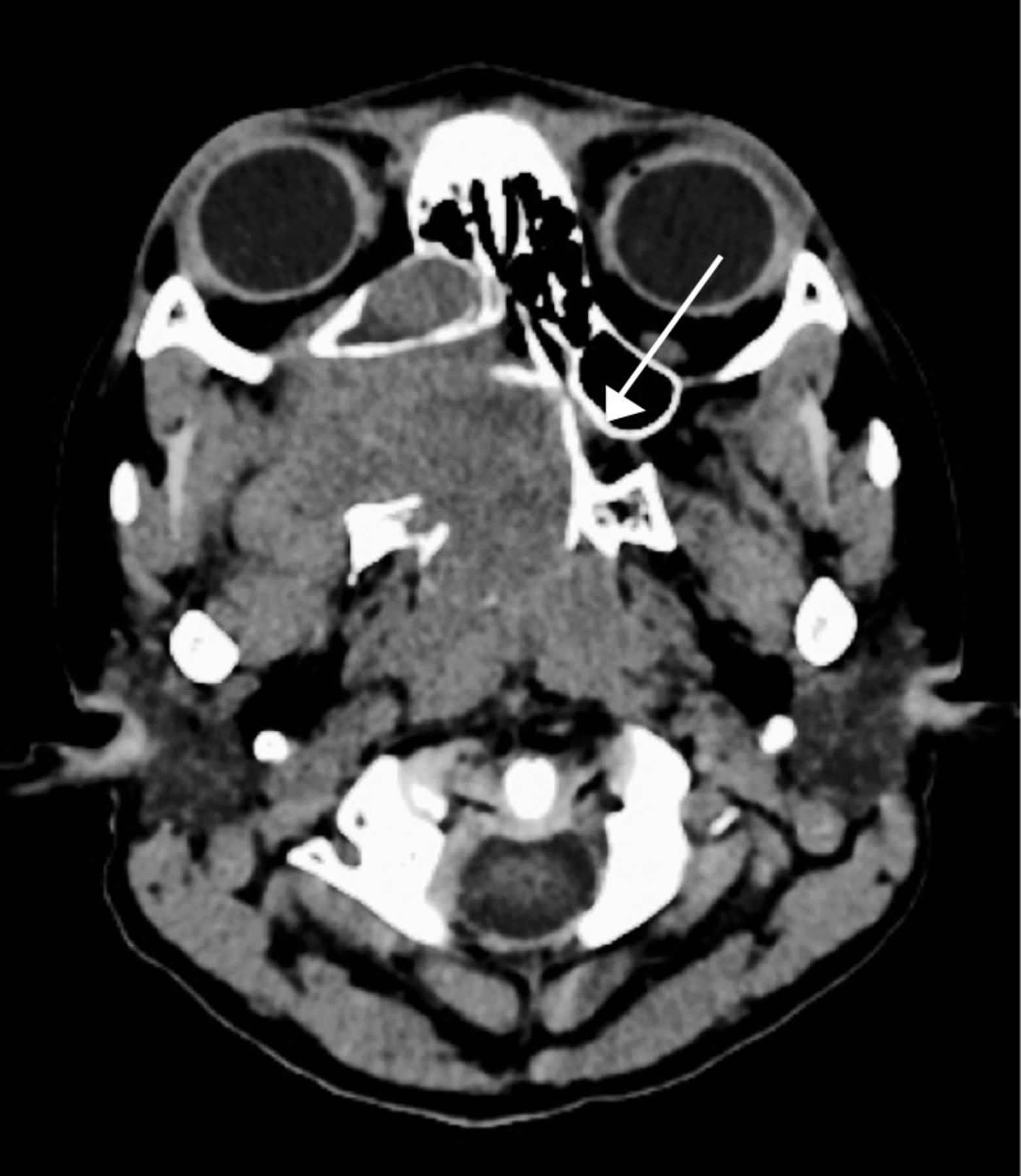
Computed tomography shows the mass extending from the right nasopharynx through the markedly widened sphenopalatine foramen and pterygopalatine fossa on the right. The right maxillary sinus is displaced anteriorly and filled with secretions. The normal left sphenopalatine foramen is shown for comparison (white arrow).

T1 contrast-enhanced magnetic resonance imaging shows enhancing tumor in the right nasopharynx (white arrow) and posterior nasal fossa (black arrow). The tumor extends laterally through the pterygopalatine fossa to the inferotemporal fossa where it displaces the temporalis, masseter, and lateral pterygoid muscles.

T1 contrast-enhanced magnetic resonance imaging shows the juvenile nasopharyngeal angiofibroma as it extends through the orbital apex via the inferior orbital fissure to the right cavernous sinus (white arrow) lateral to the expanded, tumor-filled sphenoid sinus.
The otolaryngologic surgeon described the initial biopsy of the nasal fossa component as highly vascular, but the specimen was nondiagnostic. The neurointerventional service was consulted for arterial embolization prior to surgical removal. The mass was arterially supplied via distal branches of the right maxillary artery and the right middle meningeal artery, as well as small cavernous segment branches of the internal carotid artery. Approximately 90% of the vascular supply to the tumor was successfully embolized using polyvinyl alcohol particles (Figure 4). The patient subsequently underwent surgical removal of the tumor. JNA was the final diagnosis.

Angiography via a microcatheter within the distal right maxillary artery shows the hypervascular tumor stain. Embolization was performed with 150-250 micron polyvinyl alcohol particles at this location as well as from the middle meningeal artery (not shown).
DISCUSSION
JNA is a relatively uncommon neoplasm of the nasopharynx, accounting for 0.05% of all head and neck neoplasms, yet it is considered to be the most common benign neoplasm to arise in this location and occurs almost exclusively in adolescent boys.1 JNA cases are characteristically extremely aggressive, locally invasive, and highly vascular. Severe epistaxis may be the initial presentation. The main treatment modality for these tumors is surgical removal. Preoperative embolization of the tumor vasculature is often performed secondary to the vascular nature of the tumor.2
Although detection and early intervention are improving, JNA demonstrates early and high rates of recurrence, with a mean recurrence rate of 32% and an even higher recurrence rate of 40%-50% if the initial lesion involved the skull base.3 Recurrence is actually the growth of residual disease; complete resection is difficult once the tumor begins to invade the skull base and extends intracranially.
In a single institution study of 32 patients,4 no patients with stage 4 disease, demonstrating intracranial extension, obtained complete resection. Of patients with stage 3 disease, characterized by the tumor extending into the antrum, ethmoid sinus, orbit, pterygomaxillary fossa, and/or the infratemporal fossa, 51% were determined to have received complete resection of the original lesion. All patients with stage 1 (confined to the nasopharynx) and stage 2 (involving the nasal cavity/sphenoid) lesions received complete resection of their tumors in this series. This review used the Sessions staging system.4
LCH, formerly referred to as histiocytosis X, is an overall poorly understood process, with an estimated incidence of 2-10 cases per million children.5 This lesion, characterized by the abnormal proliferation of histiocytes and granuloma formation, is considered a disorder of immunologic regulation, although LCH may involve any aspect of the reticuloendothelial system.6 The manifest lesions can commonly mimic an infectious process as well as other benign and malignant tumors.4 LCH often presents as a lytic lesion in the skull, as was the case for this patient,7 but it can also present as a soft tissue mass.6
Footnotes
The authors have no financial or proprietary interest in the subject matter of this article.
- © Academic Division of Ochsner Clinic Foundation








{kind=link}
{kind=link}
{kind=link}
{kind=link}