
Abstract
Background Cognitive behavioral therapy (CBT) has proven useful in treating fibromyalgia, depression, and anxiety. Computerized delivery of CBT allows increased access to such therapy. This study assessed the effect of internet-based CBT on Fibromyalgia Impact Questionnaire (FIQ) composite scores and tender point assessments.
Methods This 12-week randomized controlled trial included patients ≥18 years of age with 1990 American College of Rheumatology criteria for fibromyalgia and mild to moderate depression and anxiety. A total of 56 subjects were randomized into either a 6-week internet-based CBT group (MoodGYM) or a control group (standard care). We evaluated patients in both groups at 1-, 6-, and 12-week follow-up. The primary outcome measure was change in FIQ composite score. A secondary outcome measure was change in tender point assessment.
Results The mean age of study participants was 55 years, and 88% were female. Mean FIQ scores were significantly lower in the MoodGYM group compared to the control group (P<0.05 for group differences at 6 and 12 weeks). Mean tender point scores were also significantly lower in the MoodGYM group (P<0.001 at 6 and 12 weeks). We found no significant difference in the FIQ scores across the 3 timepoints in the MoodGYM group, but tender points showed a significant negative trend from baseline to 12-week follow-up.
Conclusion Patients in the internet-based MoodGYM CBT program had lower FIQ and tender point scores at 6- and 12-week follow-up. Internet-based CBT could be beneficial in the treatment of mild to moderate depression and anxiety in patients with fibromyalgia by allowing increased access to CBT.
INTRODUCTION
Fibromyalgia (FM) is a chronic disorder of unknown etiology, characterized by widespread pain, muscle tenderness, decreased pain threshold to pressure, fatigue, stiffness, sleep disturbances, and psychological distress (cognitive mood disturbances, lack of well-being, depression, or memory problems).1 The prevalence of FM in industrialized countries reportedly ranges from 0.5%-4%2,3 and is just as high in rural and nonindustrialized societies.
A combination of pharmacologic and nonpharmacologic interventions may be the most efficacious option to manage patients with FM.4 Several reports have supported the effectiveness of nonpharmacologic treatment in FM.5,6 The 2 best-studied nonpharmacologic therapies are cognitive behavioral therapy (CBT) and exercise. CBT—a type of psychotherapy that focuses on patients' understanding of how their thoughts and feelings may contribute to destructive, negative thoughts and behaviors—has been widely used to treat depression and anxiety. Both CBT and exercise have been shown to be efficacious in the treatment of many medical conditions, including FM.1,7 However, nonpharmacologic interventions are less likely to be used in clinical settings. Limitations are in part caused by inadequate access to qualified therapists, insufficient third-party coverage, a lack of physician awareness, or time constraints in implementing nonpharmacologic approaches. The patient burden associated with traveling to and from therapy may be another barrier.
The internet may help overcome some of these barriers. Many healthcare and mental health providers are using the internet more frequently to provide care.8,9 Several cognitive-behavioral internet interventions have been studied regarding chronic pain and patients with FM, and the interventions have shown promising results in improving pain and functional status.9
In an internet survey of 2,596 people with FM, more than 80% named emotional distress—including anxiety and depression—as an aggravating factor for their FM. Despite the number of people reporting these aggravating factors, only 8% of respondents used CBT to help control their symptoms.10
Computer-delivered CBT (cCBT) has been evaluated extensively. Several studies have shown no differences between CBT delivered by a therapist or via electronic means.7,11,12 Advantages of cCBT include convenience, flexibility, privacy, availability, and accessibility, especially for patients living in remote areas.
The primary purpose of our study was to compare the free cCBT program MoodGYM with standard pharmacologic therapy in patients with FM and mild to moderate depression and anxiety.
METHODS
Participants and Setting
This study was conducted at the Ochsner Medical Center in New Orleans, LA. Participants were patients seen in the outpatient rheumatology clinic. The institutional review board approved the study protocol, information brochure, and informed consent form. All participants gave their informed consent prior to the study.
Study Design
In this prospective, controlled trial, subjects were randomized using a 1:1 ratio into 2 groups: cCBT via MoodGYM or stable pharmacologic therapy.
Procedure and Randomization
Patients randomized to standard treatment maintained their current FM therapy for the duration of the study without any changes. These patients also received online educational information about FM. Patients randomized to the intervention group participated in the MoodGYM program and had 6 weeks to access and complete the program. They also maintained their current FM treatments without change. Patients in both groups visited the clinic at 0, 1, 6, and 12 weeks.
We collected data at 1, 6, and 12 weeks through the use of questionnaires completed during the office visit. Subjects who withdrew or did not complete the program were included in the final data analysis on an intention-to-treat basis.
Visit 1, Week 0
We assessed patients diagnosed with FM using the American College of Rheumatology (ACR) 1990 criteria for symptoms of mild to moderate anxiety and depression by survey and for pain by visual analog scale. We obtained consent from eligible patients and randomized them as explained previously. We instructed patients to maintain their current therapy for FM, depression, and anxiety throughout the study.
Visit 2, Week 1
Patients completed the Fibromyalgia Impact Questionnaire (FIQ) to provide baseline scores. Their treating clinicians assessed the number of tender points. This information was maintained under username and password protection. We taught the experimental patients how to use the MoodGYM program and informed them of the 6-week deadline. Additionally, we gave these patients a stamped, preaddressed postcard to mail to the clinic when they had completed the program.
Visit 3, Week 6
This visit was scheduled after we received the postcards, at week 6 ±1 week after the beginning of the study. At this visit, patients took the FIQ again, and the same clinician reassessed their tender points. We recorded scores and collected completion certificates from patients in the intervention group to document compliance with therapy.
Visit 4, Week 12
At this visit, we administered a final FIQ, and the clinician conducted a final tender point assessment.
The primary outcome measure was change in FIQ score, a composite of 10 items, at 6 and 12 weeks. The first item contains 11 questions related to physical functioning. Each question is rated on a 4-point Likert-type scale. Items 2 and 3 ask patients to mark the number of days they felt well and the number of days they were unable to work (including housework) because of FM symptoms. Items 4 through 10 are horizontal linear scales of 1 to 10. Patients were asked to assign a numeric value to work difficulty, pain, fatigue, morning tiredness, stiffness, anxiety, and depression. The secondary outcome measure was change in tender point assessment performed by a clinician.
Inclusion and Exclusion Criteria
Inclusion criteria consisted of the following:
Men and women ages ≥18 years who met the ACR criteria for FM and had a mean score of 4 or greater on a 0-10 visual analog pain scale prior to randomization
Patients under the medical care of a rheumatologist for at least 3 months
Patients on stable pharmacotherapy for the length of the study
Patients with basic computer literacy
Patients with computer access
Exclusion criteria included the following:
Patients having evidence of an inflammatory rheumatic disease or another disease process that could contribute to chronic pain or having significant, unstable medical or psychologic conditions that would compromise participation in the study or informed consent
Patients with signs or symptoms of severe depression or other severe psychologic disturbances
Patients currently undergoing CBT by any other system
Patient whose pharmacotherapy changed during the length of the study
Program and Evaluation Model: MoodGYM
MoodGYM, a free interactive online program (www.moodgym.anu.edu.au), was developed at the Centre for Mental Health Research at the Australian National University to help patients determine if they are having problems with emotions such as anxiety and depression and learn skills that can help them cope with these emotions (Figure 1). MoodGYM is based on CBT and interpersonal therapy, both of which have been successful in preventing and treating depression and anxiety. The program is confidential, and patients are encouraged to use a pseudonym.

MoodGYM training program web page.
MoodGYM contains 5 modules based on cognitive reconstructing, relaxation, pleasant events, assertiveness training, and problem solving. These models assess symptoms of depression and anxiety, feelings, and emotional encounters through the use of online quizzes, exercises, games, and an interactive workbook. This information is used in further modules to show the patient how his/her thoughts and feelings impact daily life and decisions, and the program provides structured lifestyle changes to improve and assess these thoughts. Once all the modules are completed, the patient receives a certificate of completion.
Statistical Analyses
Analyses of variance (ANOVA) were employed to assess the differences in means (FIQ and tender points) between the control and intervention groups at each point in time (ie, weeks 1, 6, and 12). Post hoc Bonferroni analyses were performed to calculate the differences between each pairwise comparison, adjusting for both intervention and control groups. An effect size was calculated to assess the mean change over time. We subtracted the means between 2 consecutive follow-ups (ie, xt – xt+1, where x is the mean score for FIQ or tender points and t is time). ANOVA were used to determine statistical significance. We also analyzed the number of patients completing the program and the number of patients able to obtain computer access.
Data management and statistical analyses were performed in Stata, v.11 (College Station, TX), and P<0.05 was considered statistically significant.
RESULTS
Sample Selection and Patient Characteristics
Over a 24-month period, we assessed 90 subjects for eligibility (Figure 2). We excluded 34 subjects based on the previously described criteria. The majority of exclusions involved patients who failed to meet the ACR criteria and/or who had a concurrent rheumatologic condition. The original study sample consisted of 56 participants, all of whom continued to receive standard medical care from their rheumatologist. After randomization, 28 were in the intervention (MoodGYM) group and 28 were in the control group.

Study inclusion flow diagram.
Eleven subjects from the intervention group and 1 subject from the control group were lost to follow-up because of noncompliance, medication changes, family illnesses, or other personal reasons. Thus, in the end we had a total study size of 44. The majority of the subjects were Caucasian (not of Hispanic origin) women.
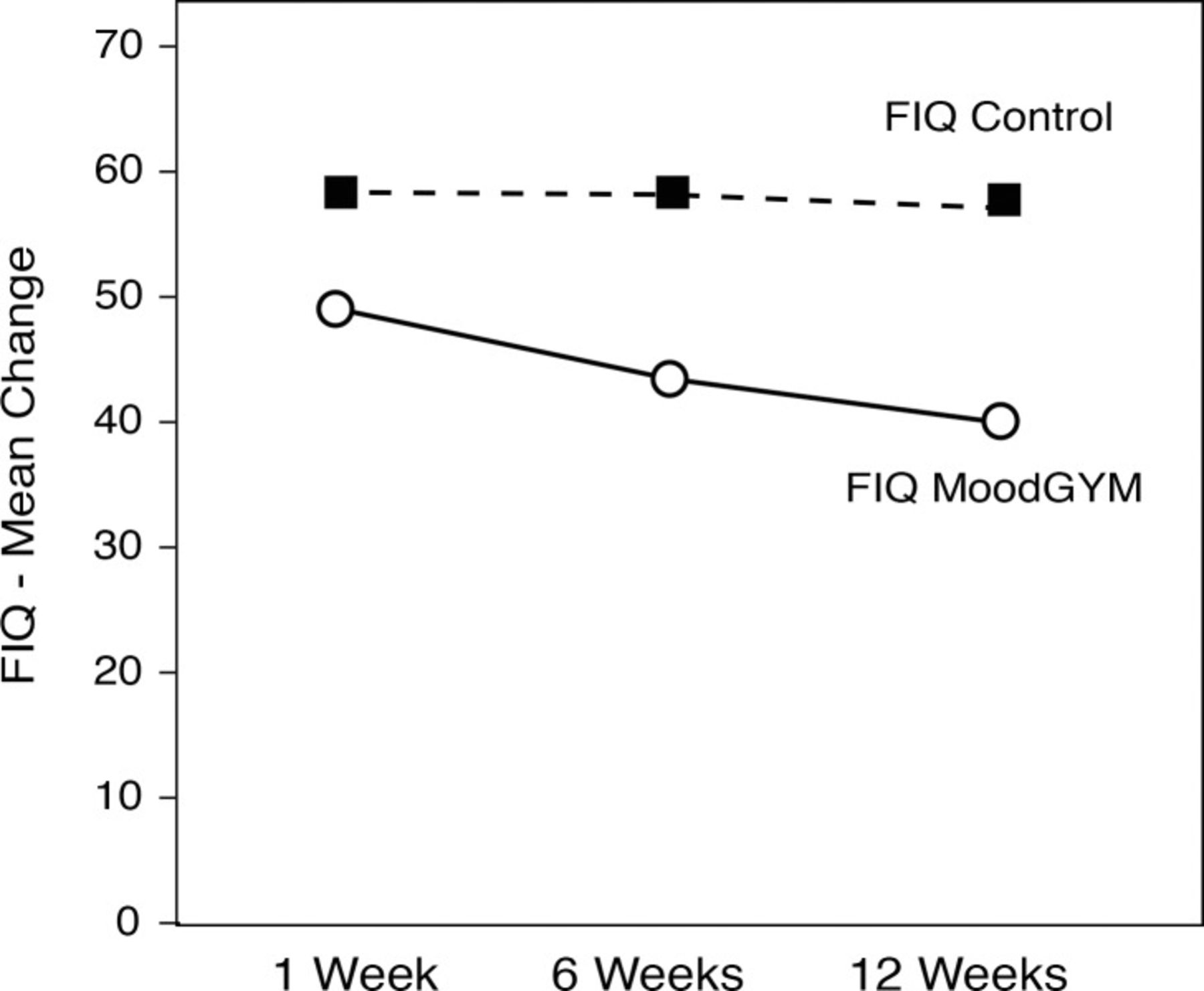
Table 1 compares both FIQ and tender points between the control and intervention groups over the 12-week study period. FIQ was the primary outcome measure, and patients in the control group had higher FIQ scores compared to the intervention group regardless of the time of the visit. At week 1, the FIQ mean scores between the 2 groups did not differ significantly, P=0.121. The intervention group compared to the control group showed a significant difference in mean FIQ score at 6 weeks (43.9 vs 58.6, P=0.005) and at 12 weeks (41.0 vs 57.7, P=0.008).
Comparison of Fibromyalgia Impact Questionnaire Scores and Number of Tender Points
At 12 weeks, the difference in FIQ scores for patients in the MoodGYM group was 8.7 points from baseline (1 week), whereas scores for patients in the control group had a modest decrease in FIQ of 1.1 points. However, the difference in decrease rates was not significant (P=0.185) (data not shown).
Regarding the number of tender points, no statistical difference was found at week 1 between the intervention and control groups (14.7 vs 16.5, P=0.069). At 6 weeks, the MoodGYM group had a significantly lower number of tender points compared to the control group (10.4 vs 16.5, P<0.001). A statistically significant negative trend was also detected at 12 weeks when the intervention and control groups were compared, P<0.001. The number of tender points dropped significantly from 14.7 to 9.5 in the intervention group, a decrease of 5.2 points (P<0.001) (data not shown).
For the MoodGYM group, we compared the overall effect of follow-up time among FIQ and tender points measures, as well as pairwise comparisons of 2 follow-ups at a time (eg, week 1 vs week 6 for FQI scores) to assess statistical significance. In total, 8 comparisons were obtained, as shown in Table 2. For FIQ scores, the overall effect of time was not statistically significant (P=0.367). In addition, none of the pairwise comparisons for FIQ scores was significant at the 5% level.
Longitudinal Effect of Fibromyalgia Impact Questionnaire Scores and Number of Tender Points in the Intervention (MoodGYM) Group
However, tender points showed a significant negative trend from baseline to 12 weeks (P=0.005). The comparison between baseline and 6 weeks also showed a significant reduction in tender points (4.3, P=0.006), and the same significance was found for the comparison of week 1 and week 12 (5.2, P=0.001). The difference in mean tender points between 6 weeks and 12 weeks did not reach statistical significance.
Trends of the mean FIQ scores and tender points are illustrated in Figures 3 and 4.

Mean change in Fibromyalgia Impact Questionnaire (FIQ) score over 12 weeks in the intervention (MoodGYM) and control groups.
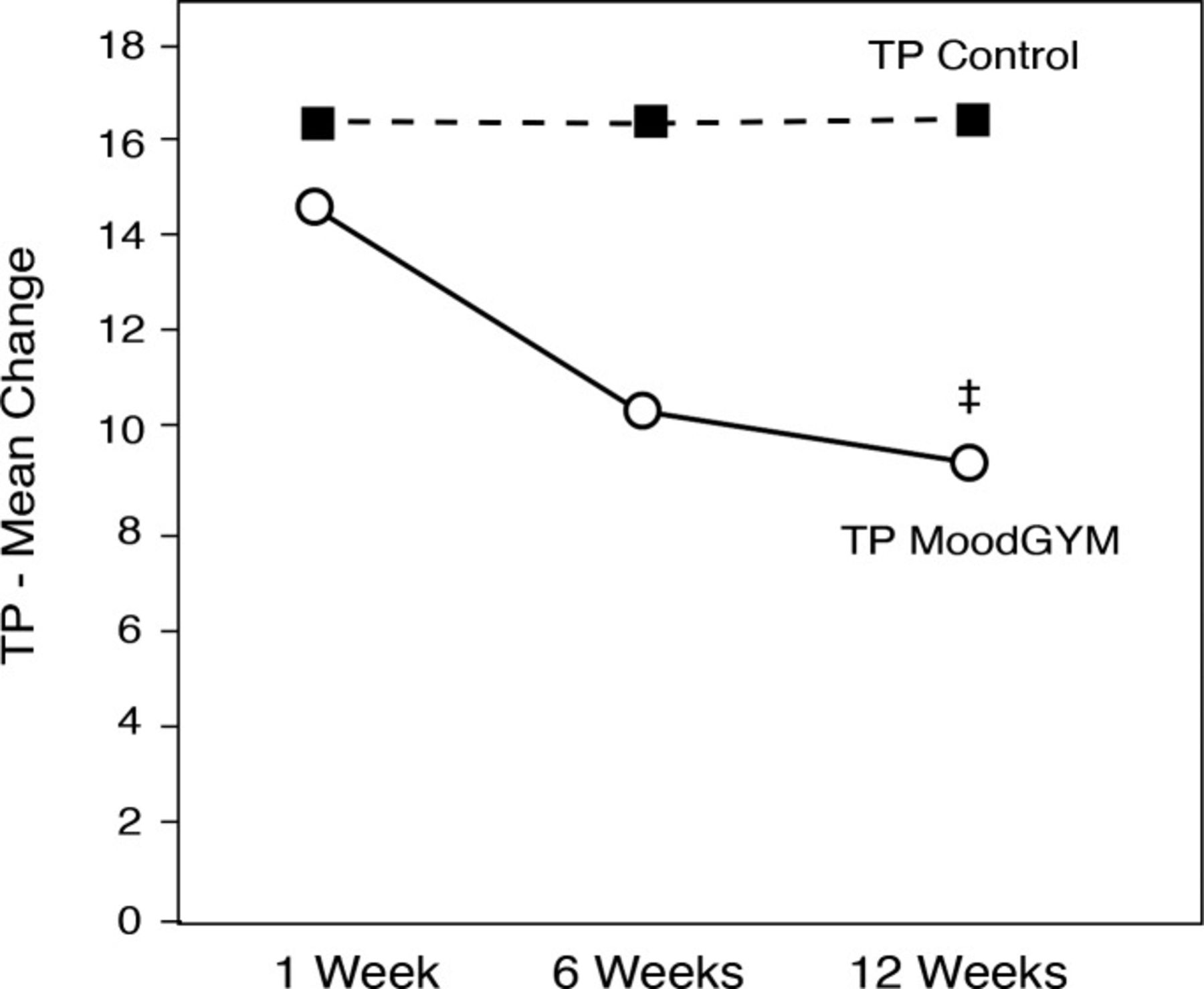
Mean change in the number of tender points (TP) over 12 weeks in the intervention (MoodGYM) and control groups.
‡Denotes statistical significance.
DISCUSSION
FM can be challenging to treat. Most patients are managed in clinic with dual reuptake inhibitors or anticonvulsant medications. Although controlled clinical trials have suggested that pharmacologic treatments provide some relief of symptoms for patients with FM, these benefits are modest at best.9,13 Psychosocial interventions such as exercise programs and CBT have also shown promise, with CBT being the most effective.13 Some reports demonstrate that patients may prefer psychologic treatments.14 Classically, CBT administration is therapist dependent, but this approach may be costly and/or not readily available.
Several reported randomized trials for internet-based therapies for mental health conditions have shown promise.9,15 One pretrial study is looking at the use of mobile applications as a possible self-management tool for patients with chronic pain and for patients with FM. Data support the idea that such an intervention may be feasible.8 Researchers in the Netherlands created an interactive internet-based CBT program called FITNET for adolescents with chronic fatigue syndrome, a condition related to FM with similar features.16 Participants in the FITNET group could email a therapist who would provide weekly online consultations. FITNET offered a parallel program for parents as well. The researchers found that internet-based CBT was much more effective than standard care for chronic fatigue syndrome in teenagers. The results included improved school attendance, reduced fatigue severity, improved physical functioning, and higher self-rated improvement. These improvements in symptoms persisted at 12 months.16
Our 12-week study compared cCBT with standard therapy for patients with FM and mild to moderate depression and anxiety. The intervention resulted in significantly improved FIQ scores and significantly decreased tender points between patients in the MoodGYM group and in the control group at weeks 6 and 12. Additionally, the number of tender points improved in the MoodGYM group across time compared to baseline at a level not seen in the similar analysis of FIQ scores.
Limitations of our study include the small sample size and the higher attrition rate in the intervention group than in the control group. The small sample size likely accounts for the lack of statistical significance in FIQ scores over time in the MoodGYM group. However, sample size did not affect the improvement in FIQ scores in the MoodGYM group compared to the control group; the difference was statistically significant.
Other limitations may include the lack of comparison of cCBT to traditional face-to-face CBT. Additionally, the use of a web-based CBT program requires patients to be familiar with and have access to the internet. Although the majority of the patients we screened had computer access, some patients may not be computer literate or have access to computers, cell phones with internet capabilities, or the internet.
Several studies have supported the use of CBT as a nonpharmacologic therapeutic approach to the treatment and management of FM, depression, and chronic fatigue syndrome.16-21 A recent study found that CBT by telephone was helpful in the management of chronic depression compared to face-to-face CBT in lowering attrition rates and improving depression.17 Other studies have shown a lower rate of side effects and dropouts in patients undergoing CBT compared to those on antidepressants.22
CONCLUSION
The increased availability of cCBT may be beneficial to the management of FM. The effectiveness of cCBT in our study recommends it as an alternative in the treatment of mild to moderate depression and anxiety in patients with FM.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care and Medical Knowledge.
ACKNOWLEDGMENT
We thank Smita Padigala, MD, for her assistance with manuscript preparation.
Footnotes
The authors have no financial or proprietary interest in the subject matter of this article.
- © Academic Division of Ochsner Clinic Foundation








{kind=link}
{kind=link}
{kind=link}
{kind=link}