
Abstract
Background Male breast cancer is relatively rare, comprising only 0.7% of all breast cancer cases. Male breast cancer usually presents with a palpable, nontender, retroareolar mass and occasional bloody discharge from the nipple. The typical age at presentation is between 60 and 70 years old (mean age of 67), which is significantly later than female presentation. Male breast cancer is generally diagnosed at a more advanced stage than female breast cancer.
Case Report A 74-year-old white male presented to his primary care physician with a palpable, nontender 2.5 cm mass in the subareolar region of his right breast. The patient underwent a right mastectomy with right sentinel lymph node biopsy. The final surgical pathology revealed a 20 mm area of stage 0 intracystic papillary–type ductal carcinoma in situ.
Conclusion Male breast cancer is a relatively rare cause of morbidity and mortality among men. Screening for male breast cancer is not recommended for the general population but is encouraged for individuals known to be high risk. High-risk status is reserved for patients with extensive family history of breast cancer, known BRCA2 mutations, medical disorders causing hyperestrogenism, or radiation exposure.
INTRODUCTION
Male breast cancer is relatively rare, comprising only 0.7% of all breast cancer cases.1 Male breast cancer usually presents with a palpable, nontender, retroareolar mass and occasional bloody discharge from the nipple.2 The typical age at presentation is between 60 and 70 years old (mean age of 67), which is significantly later than female presentation.1,3 Male breast cancer is generally diagnosed at a more advanced stage than female breast cancer. Fifty percent of male patients present with stage 2 or above, compared to 35% of female patients, and more than half of male patients exhibit lymph node metastasis at the time of diagnosis.4 The more advanced stage at presentation is thought to be a function of delayed presentation, possibly because of decreased patient awareness and physician suspicion.2
Similar to female breast cancers, important risk factors for male breast cancer include family history and genetic predisposition caused by mutations in the BRCA2 gene.5 Hyperestrogenism is another known risk factor for male breast cancer. Endocrine disorders such as Klinefelter syndrome and testicular disorders such as cryptorchidism are indicators that men may be at increased risk for male breast cancer.5 Radiation exposure is another risk factor.5
CASE REPORT
A 74-year-old white male with a history of hypertension, type 2 diabetes, Barrett esophagus, multinodular goiter, benign prostatic hyperplasia, and cerebrovascular disease presented to his primary care physician with a palpable, nontender 2.5 cm mass in the subareolar region of his right breast. The mass was mobile with no apparent fixation to the skin or underlying chest wall. The patient had no evidence of nipple retraction or discharge. No lymphadenopathy was detected on examination.
The patient's family history was significant for a maternal grandmother treated for breast cancer with a radical mastectomy at an unknown age. The patient denied any occupational or radiation exposures.
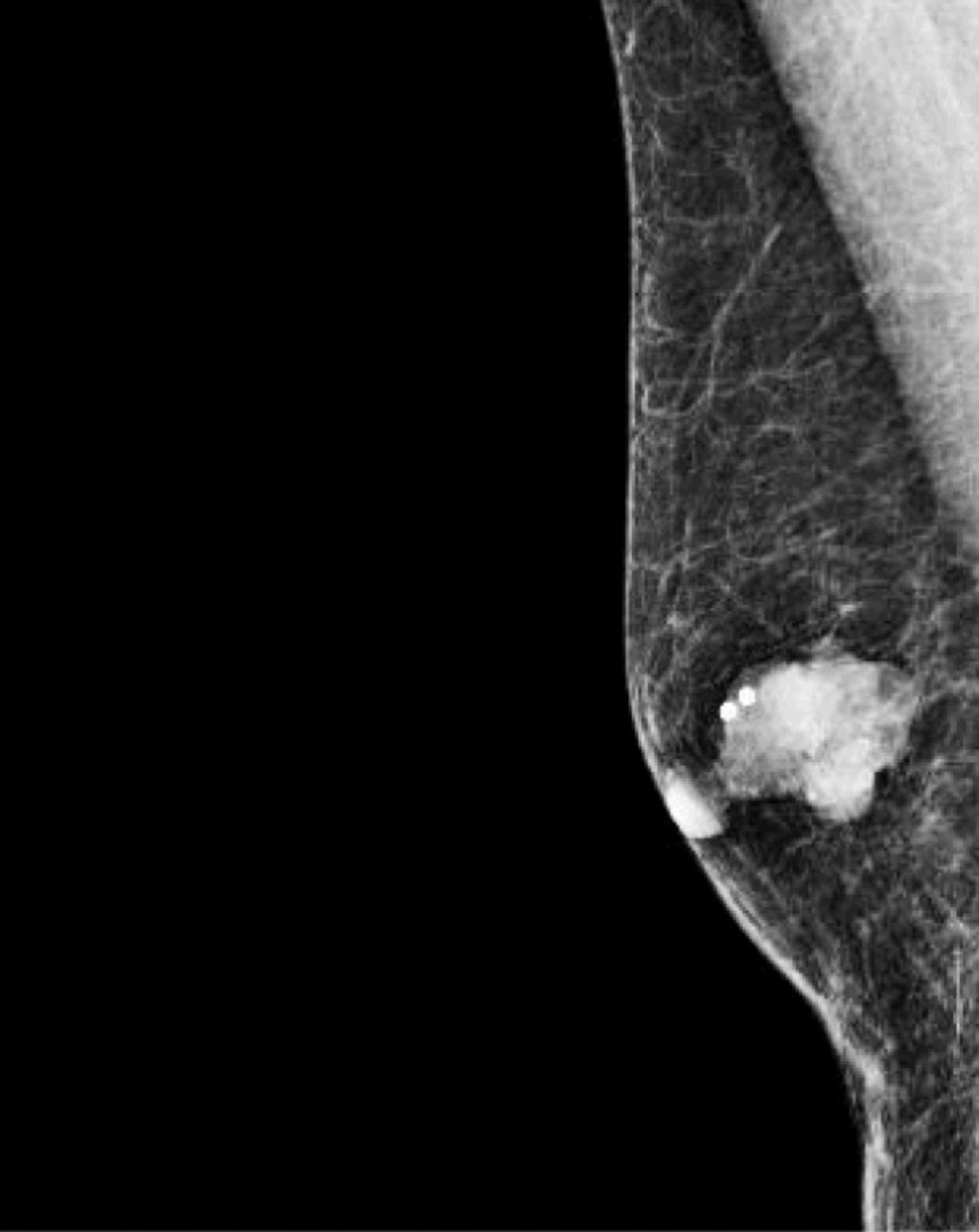
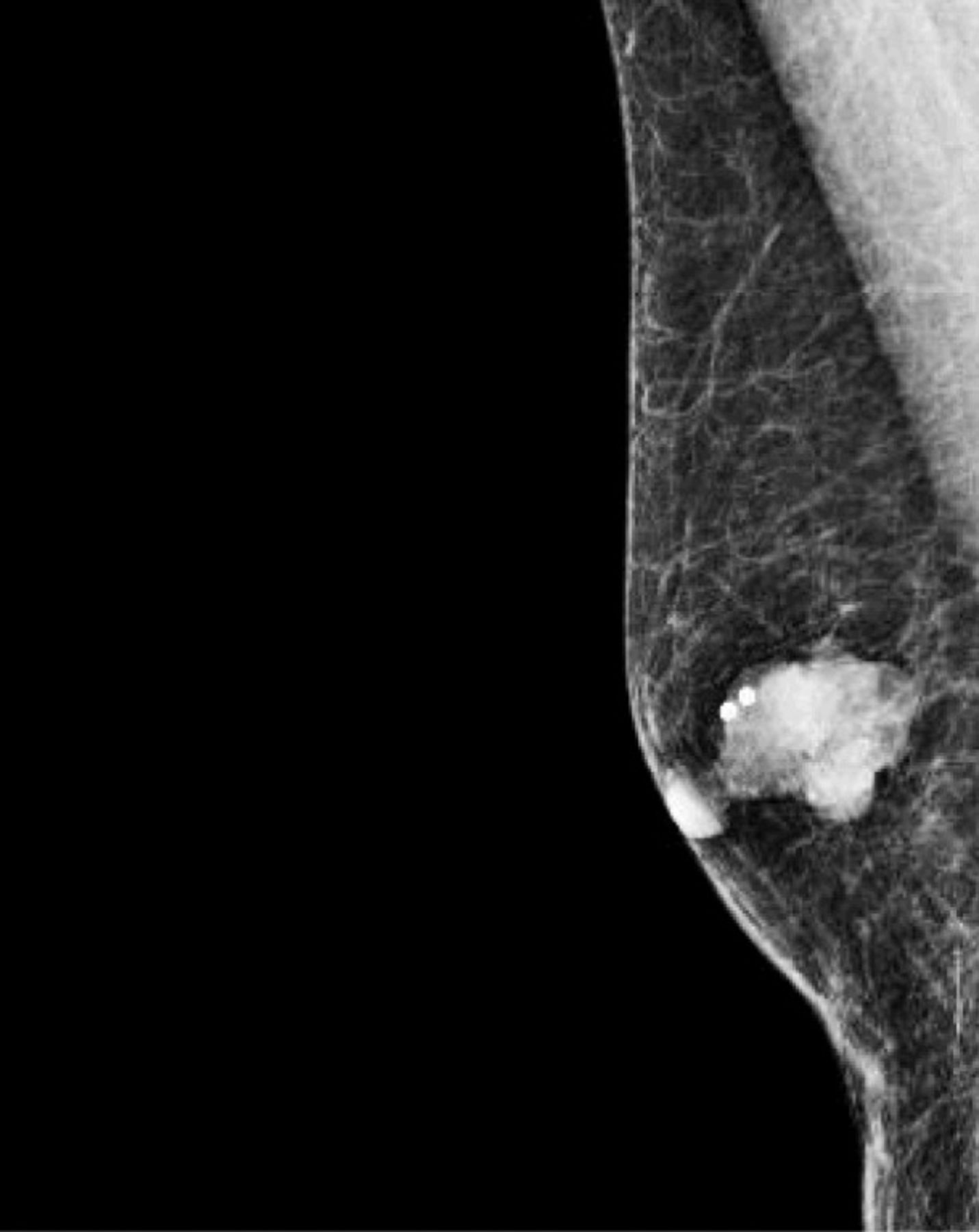
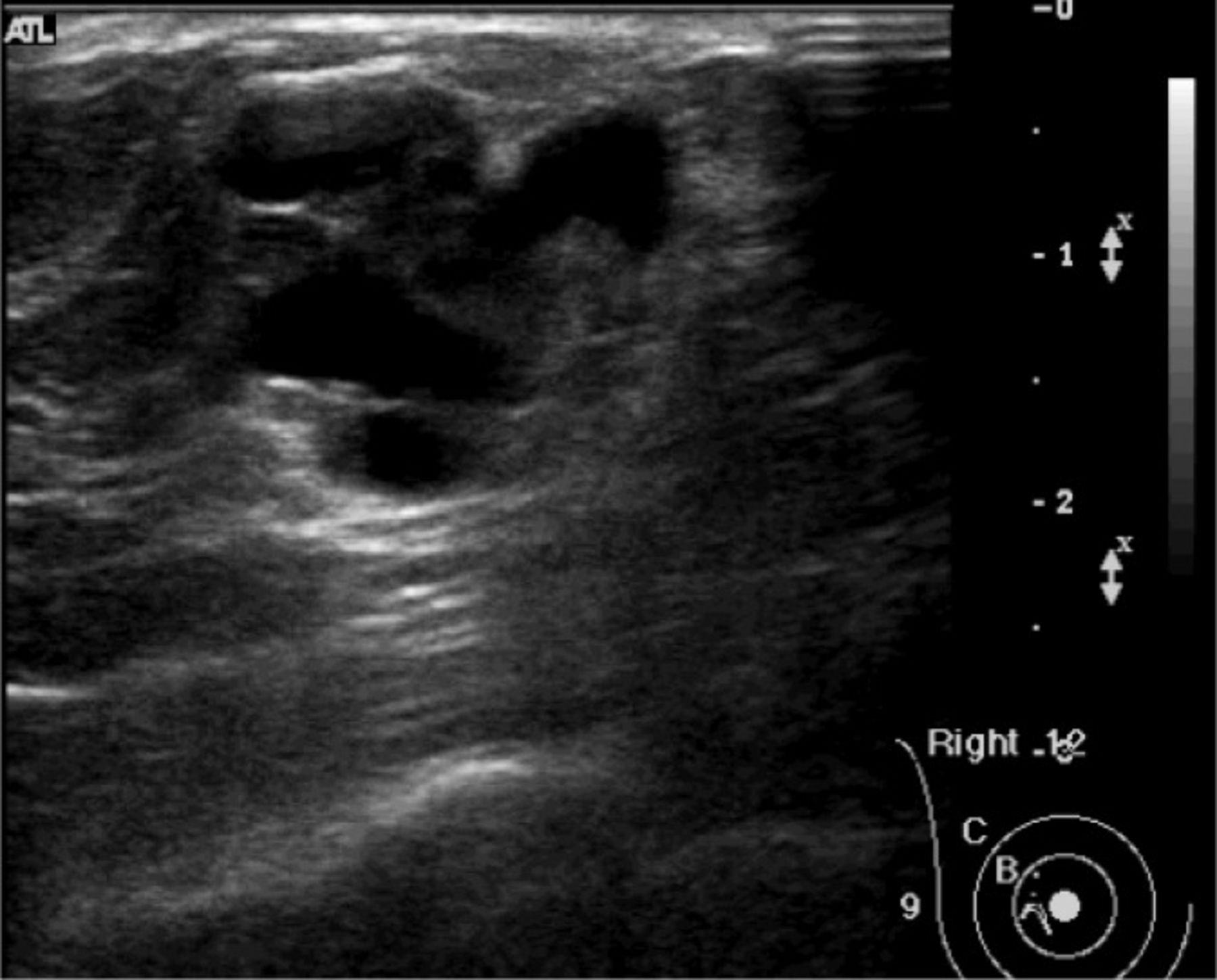
Mammogram revealed a lobular mass measuring 2.5 cm in the subareolar region (Figures 1 and 2). Ultrasound revealed a complex cystic mass with thick septations and solid components (Figure 3). The mass was suspicious for malignancy (Breast Imaging Reporting and Data System category 4); therefore, the patient underwent a vacuum-assisted ultrasound-guided core needle biopsy.

Right cranial/caudal mammogram showing a 2.5 cm lobular mass in the subareolar region.
Right medial/lateral mammogram showing a 2.5 cm mass in the subareolar region.

Ultrasound of the right breast showing a complex cystic mass with thick septations and solid components.
The biopsy revealed intracystic (encapsulated) papillary carcinoma with no invasion identified. Hormone receptor staining showed estrogen receptor positivity above 99% and progesterone receptor positivity less than 1%. HER-2/neu protooncogene overexpression was identified by fluorescence in situ hybridization.
The patient subsequently underwent a right mastectomy with right sentinel lymph node biopsy. The final surgical pathology revealed a 20 mm area of stage 0 intracystic papillary–type ductal carcinoma in situ. The tumor was identified as high grade without signs of necrosis. All margins were negative, with the closest margin 1 cm from deep structures. Three lymph nodes from the right axilla were sampled, and all were negative for metastasis.
The patient did not undergo subsequent radiation or endocrine therapy. He will be closely followed with biannual clinical breast examinations and annual contralateral screening mammograms.
DISCUSSION
This patient was not considered to be at high risk for breast cancer before his diagnosis. The patient's maternal grandmother was treated for breast cancer, but the rest of his family history did not suggest a BRCA2 mutation. The patient had a body mass index of 28.5 at the time of diagnosis. Obesity leading to hyperestrogenism has been linked to male breast cancer but is not considered a major risk factor.5
Male breast tumors are usually low grade and show both estrogen and progesterone receptor positivity in up to 90% of cases.1 HER-2/neu protooncogene overexpression is less likely to be found in cases of male breast cancer compared to female breast cancer.1,4 The hormone receptor status for this patient's tumor (estrogen-receptor positive, progesterone-receptor negative, HER-2/neu positive) is rare. Although estrogen receptor positivity is typical among male breast cancers, progesterone negativity and HER-2/neu positivity is uncommon.1,4 The significance of this hormone expression is unknown.
This case presentation is unusual because the patient presented with a palpable, pure ductal carcinoma in situ rather than the advanced, invasive breast cancer most commonly seen in presentations of male breast cancer. Pure ductal carcinoma in situ accounts for only 10% of male breast cancers, with papillary and cribriform subtypes being the most common.1,4,6
Male breast cancers tend to behave in the same manner as female breast cancers with regard to natural history and response to treatment.2,4 Although 5-year survival rates are the same for men and women with similar cancers, overall survival rates are lower for men.1,4 The increased age at diagnosis and the increased number of comorbidities may influence survival rates.2
CONCLUSION
Male breast cancer is a relatively rare cause of morbidity and mortality among men. Screening for male breast cancer is not recommended for the general population but is encouraged for individuals known to be high risk.4 High-risk status is reserved for patients with extensive family history of breast cancer, known BRCA2 mutations, medical disorders causing hyperestrogenism, or radiation exposure.4,5
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care and Medical Knowledge.
Footnotes
The authors have no financial or proprietary interest in the subject matter of this article.
- © Academic Division of Ochsner Clinic Foundation








{kind=link}
{kind=link}
{kind=link}