
Abstract
Background Supraventricular tachycardia (SVT) is a general term describing a group of arrhythmias whose mechanism involves or is above the atrioventricular node. The mechanisms of most forms of SVT have been elucidated, and pharmacologic and invasive therapies have evolved simultaneously.
Methods We provide a brief overview of the mechanisms, classifications, and electrocardiographic characteristics of different SVTs and describe current trends in noninvasive and invasive therapies.
Results The term SVT encompasses a heterogeneous group of arrhythmias with different electrophysiologic characteristics. Knowledge of the mechanism of each SVT is important in determining management at the bedside and in the electrophysiology laboratory.
Conclusion In the acute setting, vagal maneuvers and pharmacologic therapy can be effective in arrhythmia termination. Catheter-based radiofrequency ablation has revolutionized therapy for many SVTs, and newer techniques have significantly improved ablation efficacy and reduced periprocedural complications and procedure times. Cryoablation is currently being investigated as an alternative form of energy delivery, although the long-term effectiveness of this procedure currently limits its use for many SVTs.
- Ablation–catheter
- ablation techniques
- arrhythmias–cardiac
- electric countershock
- tachycardia–supraventricular
INTRODUCTION
Supraventricular tachycardia (SVT) is a general term describing a group of arrhythmias whose mechanism involves or is above the atrioventricular node. The mechanisms of most forms of SVT have been elucidated, and pharmacologic and invasive therapies have evolved simultaneously. This review provides a brief overview of the mechanisms, classifications, and electrocardiographic characteristics of different SVTs and describes current trends in noninvasive and invasive therapies. While this review focuses on all forms of SVT, a thorough review of atrial fibrillation is beyond its scope.
EPIDEMIOLOGY OF SVT
SVT is a common entity in clinical practice and a relatively common occurrence in the emergency department. The incidence of SVT is approximately 35 cases per 100,000 patients with a prevalence of 2.25 cases per 1,000 in the general population.1 Atrial fibrillation and atrial flutter are the most common subtypes of SVT, affecting approximately 2 million patients in the United States. Of the remaining subtypes of SVT, atrioventricular nodal reentrant tachycardia (AVNRT) is the most common, accounting for approximately 60% of cases. The subtypes atrioventricular reentrant tachycardia (AVRT) and atrial tachycardia account for approximately 30% and 10% of SVT cases, respectively. AVNRT is more common in women and has a bimodal age distribution with one peak in the third decade and another that begins in the sixth decade and extends to very old age. AVRT is more common in men and has a mean onset age of 23 years. The incidence of atrial tachycardia increases with age and is more common in patients with structural heart disease.2
MECHANISMS OF SVT
SVT is caused by 1 of 3 mechanisms: reentry, increased automaticity, or triggered activity.3-5
Reentry involves repetitive impulse propagation around 2 pathways or limbs, separated by a zone of nonexcitability.3-6 For reentry to occur, the 2 limbs should have differing electrophysiologic properties (conduction velocity and refractory period). Atrial or ventricular premature beats or runs of tachycardia (automatic or triggered in origin) result in a unidirectional block in one limb with circular repetitive reentry in the opposite direction (Figure 1). Reentry is the mechanism of all cases of AVNRT and AVRT and of some cases of atrial tachycardia.

Subtypes of supraventricular tachycardia. The figures demonstrate the mechanisms of arrhythmia. Atrioventricular nodal reentrant tachycardia (far left) and atrioventricular reciprocating tachycardia (middle) are exclusively reentrant in mechanism. Atrial arrhythmias include atrial tachycardia, atrial flutter, and fibrillation and may be because of reentry, automaticity (star), or triggered activity (T) (far right). Enhanced automaticity and triggered activity may cause the initiation of reentry.
The term automaticity refers to the phenomenon of spontaneous tachycardia arising from a group, or focus, of cells and can result in atrial and ventricular arrhythmias. These foci of myocardial tissue exhibit pathologic changes in resting membrane potential and can develop the capacity to depolarize rapidly and become the dominant rhythm. Automaticity can occur in the setting of electrolyte abnormalities, changes in autonomic tone, and other local factors, many of which are not understood. Automatic foci are the mechanisms of more than 70% of cases of focal atrial tachycardia.4
Automatic arrhythmias and arrhythmias caused by triggered activity are relevant because in addition to being the mechanisms of sustained arrhythmias, short bursts of these arrhythmias are triggers for reentrant SVTs.
Arrhythmias due to triggered activity are caused by extra depolarizations immediately following cellular repolarization (called delayed afterdepolarizations) that may result in extrasystoles and sustained tachyarrhythmias. Triggered activity can occur in response to augmentation of intracellular calcium (eg, with cardiac glycosides) and is the mechanism of approximately 30% of focal atrial tachycardias. Triggered activity is also implicated in the initiation of atrial fibrillation.3,4
CLASSIFICATIONS OF SVT
Atrioventricular Nodal Reentrant Tachycardia
AVNRT is the most commonly encountered paroxysmal SVT. Patients with AVNRT demonstrate dual atrioventricular nodal inputs with differing electrophysiologic properties, the fast and slow pathways that act as the 2 limbs of the reentrant circuit. An estimated 32%-40% of the normal population have dual atrioventricular nodal physiology, although only a minority of these develop AVNRT.7 The fast pathway inputs into the apex of the triangle of Koch near the compact atrioventricular node. The slow pathway inputs near the os of the coronary sinus at the base of the triangle. In the typical form (slow-fast AVNRT), conduction occurs antegrade via the slow pathway and retrograde via the fast pathway. Atypical forms of AVNRT such as fast-slow and slow-slow are also encountered and are one of the causes of long RP tachycardia.8,9
Atrioventricular Reentrant Tachycardia
Accessory pathways are anomalous, extranodal conduction pathways between atrium and ventricle. The accessory pathway and the atrioventricular node can act as the 2 limbs of the AVRT reentrant circuit. Accessory pathways are classified based on their location along the mitral or tricuspid annuli, conduction characteristics, and directionality of conduction (antegrade, retrograde, or both). Accessory pathways capable of antegrade conduction will demonstrate a delta wave known as the Wolff-Parkinson-White (WPW) pattern on the surface electrocardiogram (ECG) (Figure 2). Accessory pathways capable only of retrograde conduction do not exhibit a delta wave on the surface ECG (concealed pathways) but can still form a reentrant loop with the atrioventricular node and result in AVRT.10,11 AVRT is classified as orthodromic if antegrade conduction occurs via the atrioventricular node and antidromic if antegrade conduction occurs via the accessory pathway.
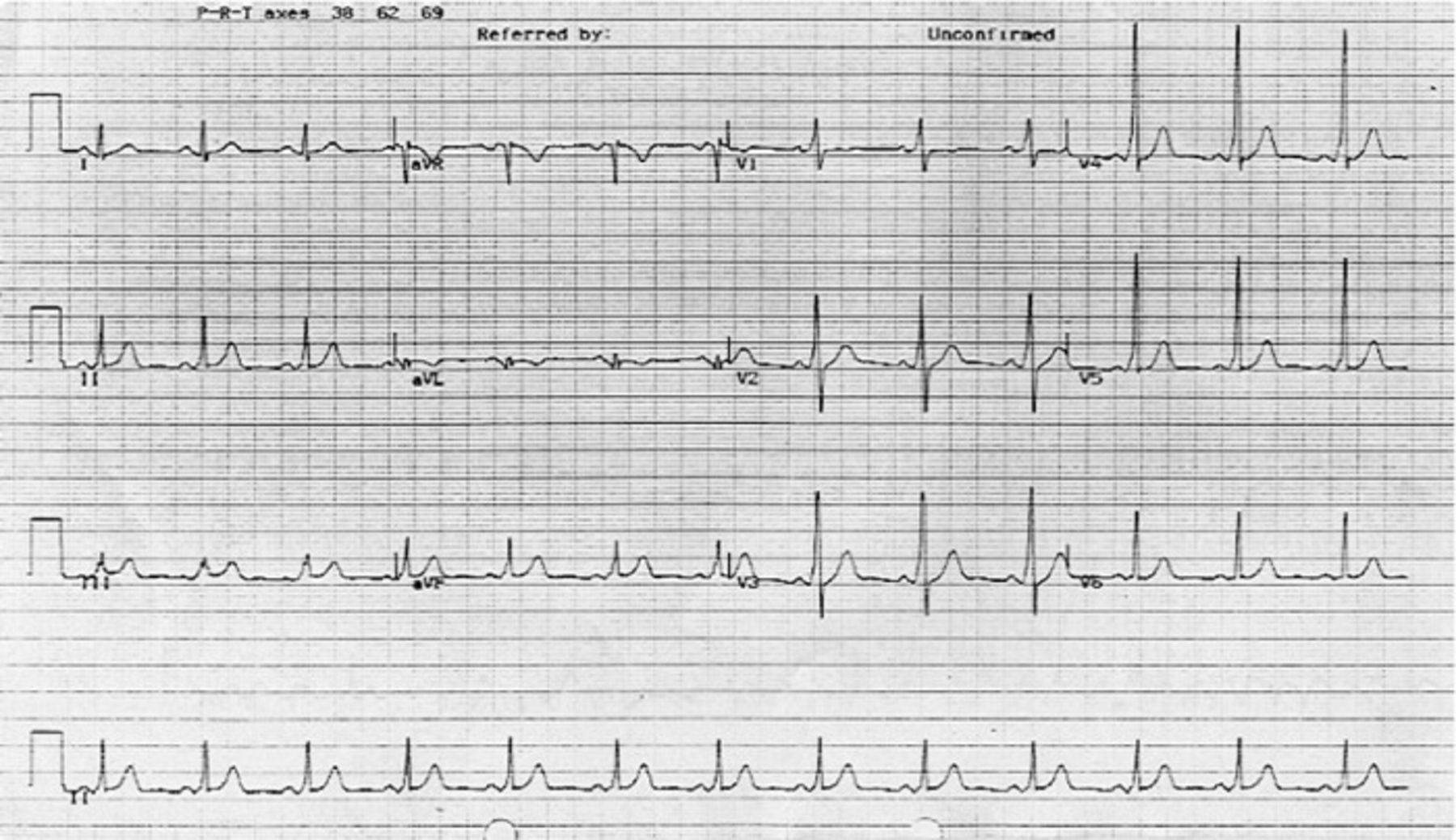
A 12-lead electrocardiogram (ECG) showing a short PR interval and slurred R wave upstroke (delta wave) characteristic of the Wolff-Parkinson-White pattern. The pattern of preexcitation on this particular ECG is suggestive of a left lateral accessory pathway.
Atrial Tachycardia
The term atrial tachycardia describes a group of atrial arrhythmias whose mechanisms may be focal or macroreentrant. Focal atrial tachycardia results in a centrifugal wavefront spread throughout the atria from a focus of (1) enhanced automaticity, (2) triggered activity, or (3) a small area of reentry (microreentry). Macroreentrant atrial tachycardia results from a large intraatrial reentrant loop >2 cm in length. Note that the term macroreentrant atrial tachycardia is synonymous with the term atrial flutter. Both focal and macroreentrant atrial tachycardia may result from prior structural heart disease or surgery for congenital heart disease, may follow surgical or catheter ablation of atrial fibrillation, or may be due to idiopathic phenomena. Right atrial tachycardia often arises from the crista terminalis but can also arise from the tricuspid annulus, compact atrioventricular node, and coronary sinus ostium.12,13 Left atrial tachycardias often arise from the pulmonary veins, as well as the mitral annulus and left atrial appendage.14
Atrial Flutter
Typical atrial flutter is a form of macroreentrant atrial tachycardia that deserves special mention because it is common, may result in stroke and cardiomyopathy, and is highly amenable to catheter ablation. In typical atrial flutter, the depolarizing wavefront courses in either a clockwise or counterclockwise direction around the tricuspid annulus and involves the cavotricuspid isthmus as a critical part of the reentrant circuit. The counterclockwise form of typical atrial flutter is the most common and results in the negative sawtooth wave pattern in the inferior leads with a positive wave in V1. Clockwise typical (cavotricuspid isthmus-dependent) atrial flutter can have a more variable appearance on ECG and can be indistinguishable from atypical atrial flutter.15,16 Atypical atrial flutter encompasses a group of macroreentrant atrial tachycardias that do not utilize the cavotricuspid isthmus for arrhythmia propagation and may involve the crista terminalis, superior vena cava, prior atrial scar in patients with a history of congenital heart disease surgery, or other right atrial structures. The era of extensive left atrial ablation for atrial fibrillation has resulted in the increasingly common occurrence of atypical atrial flutter arising from the left atrium.17 Atypical flutters can be challenging to ablate.
ECG FEATURES OF SVT
SVT usually exhibits a narrow QRS complex tachycardia, although wide complex tachycardia may occur in the case of SVT with preexisting or rate-related bundle branch block. Rarely, wide complex tachycardia may occur in the setting of preexcited SVT because of antidromic AVRT or in cases of preexcited atrial fibrillation, atrial tachycardia, or AVNRT where the accessory pathway is not part of the reentrant circuit (ie, bystander accessory pathway participation). Irregularity during SVT occurs in cases of rapid atrial fibrillation, rapid atrial flutter with variable atrioventricular block, and multifocal atrial tachycardia. Note that atrial fibrillation in the setting of complete heart block with an escape rhythm may appear regular.
SVTs may be classified in terms of the length of the RP interval that may give important clues that lead to the diagnosis of tachycardia.6 A long RP tachycardia (RP interval > PR interval) is a useful finding on the surface ECG because it is caused by atypical (ie, fast-slow) AVNRT, orthodromic AVRT utilizing a slowly conducting accessory pathway, or certain forms of atrial tachycardia (Figure 3).6

A 12-lead electrocardiogram showing a long RP tachycardia. The RP interval (A) is longer than the PR interval, with inverted P waves in the inferior leads. The differential diagnosis for this rhythm includes atypical (fast-slow) atrioventricular nodal reentrant tachycardia, atrioventricular reentrant tachycardia with a slowly conducting accessory pathway, and certain forms of atrial tachycardia.
The surface ECG can provide other clues regarding SVT etiology. A pseudo R′ in lead V1 and a pseudo S in lead II are classically associated with AVNRT (Figure 4). The finding of QRS alternans during SVT is highly suggestive of orthodromic AVRT, though this can occur in AVNRT, particularly at very rapid rates. Broad sawtooth waves in the inferior leads with positive P waves in lead V1 are suggestive of typical atrial flutter. SVT because of atrial tachycardia may appear as either a short or long RP tachycardia on the surface ECG, and the ECG may be helpful in distinguishing right from left atrial tachycardia when the P wave can be adequately visualized.6,12-14

A 12-lead electrocardiogram of atrioventricular nodal reentrant tachycardia (AVNRT). The presence of the pseudo S wave in lead II (A) is highly suggestive of AVNRT as the mechanism of supraventricular tachycardia, particularly if the rhythm terminates with adenosine.
ACUTE MANAGEMENT OF SVT
Vagal Maneuvers
Vagal maneuvers are an appropriate first treatment option in patients with hemodynamically stable SVT. Studies report an approximately 25% success rate, although reported rates vary widely in the literature (6%-54%).18-22 The most commonly performed maneuvers are the Valsalva maneuver and carotid sinus massage. The increase in intrathoracic pressure resulting from the Valsalva maneuver stimulates aortic and carotid baroreceptors, causing an increase in vagal input into the atrioventricular node. Most recent studies advocate placing the patient in a supine position and attempting the maneuver for 15-20 seconds.18,19,21 The Valsalva maneuver has generally been shown to be most effective in adults, having a superior effect on SVT termination compared to carotid sinus massage. Caution is advised when considering whether to attempt carotid sinus massage in older patients, as there is a risk of carotid atheroembolism and stroke even in the absence of an audible bruit. No guidelines currently exist regarding the appropriate number of attempts prior to initiating other therapies, although most providers will try a maximum of 2 attempts. Several studies have suggested that vagal maneuvers are more effective in the termination of AVRT compared to AVNRT.18-22
Pharmacologic Treatment
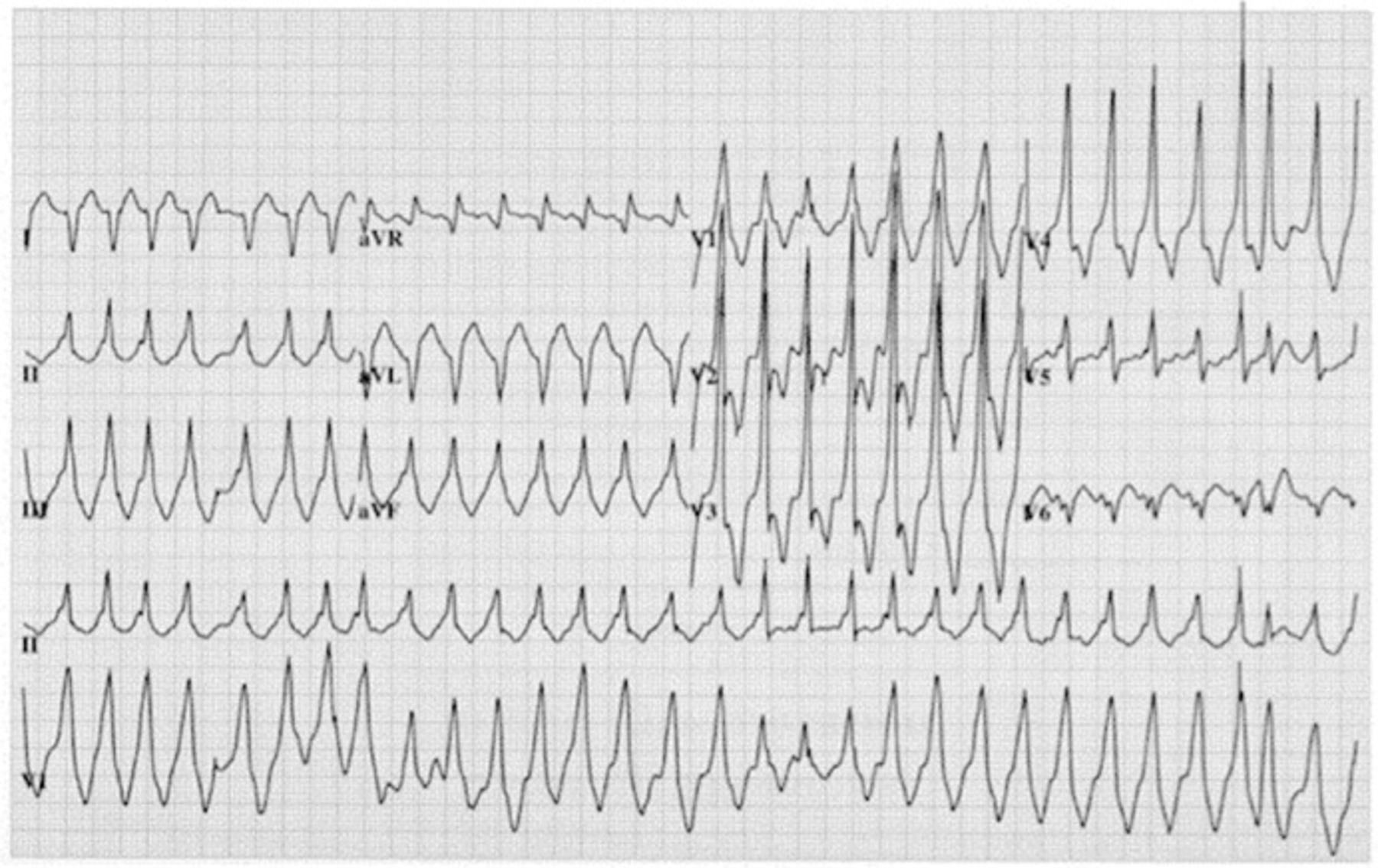
Pharmacologic therapy for acute termination of SVT is appropriate in patients when vagal maneuvers fail. The preferred initial agents are intravenous (IV) adenosine or a nondihydropyridine calcium channel blocker. Adenosine's effects are mediated by membrane hyperpolarization that typically occurs within 15-30 seconds after administration. Adenosine has a powerful effect on the atrioventricular node and is highly effective in causing temporary, complete atrioventricular nodal block. Transient sinus bradycardia or sinus arrests often occur but are short lived. The ECG should be continuously recorded during adenosine administration to document the effect of the drug on SVT and to monitor for the rare occurrence of proarrhythmia. Patients should be warned that they might experience short-lived sensations of claustrophobia, dyspnea, and chest discomfort. The initial dose of adenosine is 6 mg IV bolus (flushed), using a large vein. Subsequent doses of 12 mg or even 18 mg boluses may be required. SVT resolution following adenosine administration establishes AVNRT or AVRT as the likely SVT mechanism, although occasionally some focal atrial tachycardias will terminate with adenosine as well. In macroreentrant and most focal atrial tachycardias, adenosine administration results in transient slowing of the ventricular rate, revealing the underlying atrial activity. Adenosine is contraindicated in patients with WPW and atrial fibrillation because it shortens the refractory period of the pathway that can result in more rapid conduction of atrial fibrillation, increasing the chances of dangerous ventricular arrhythmias (Figure 5).23,24

A 12-lead electrocardiogram (ECG) showing preexcited atrial fibrillation. The ECG shows an irregular, wide complex tachycardia with QRS complexes that are similar but with varying morphologies.
Because propagation of the action potential through the atrioventricular node is calcium-channel dependent, the nondihydropyridine calcium channel blockers verapamil and diltiazem are highly effective in the termination of AVNRT and AVRT.25 Verapamil is infused at a dose of 5 mg during 2 minutes, followed by another 7.5 mg after 5-10 minutes if necessary. Diltiazem is given at a dose of 20 mg IV, with another 25-35 mg given if SVT persists. As with adenosine, transient arrhythmias may be seen, although hypotension occurs more commonly in patients receiving calcium channel blockers, especially if SVT persists after administration. Prior studies have demonstrated similar efficacy between adenosine and calcium channel blockers,23 although adenosine is generally preferred given its lower incidence of hypotension and its extremely short half-life. Beta blockers such as IV metoprolol or esmolol infusion are often used in acute SVT, but data regarding this practice are limited. A small randomized study comparing IV diltiazem to esmolol for acute SVT was terminated early because of the marked superiority of diltiazem.26
Direct-Current Cardioversion
The use of direct-current cardioversion is generally limited to cases of hemodynamically unstable SVT, a rare phenomenon. When utilized, low energies (eg, 25-50 J) will suffice. Most research focuses on direct-current cardioversion in the setting of atrial fibrillation that is more commonly treated using this modality.21
LONG-TERM MANAGEMENT OF SVT
Expectant Management
The American College of Cardiology/American Heart Association/European Society of Cardiology (ACC/AHA/ESC) guidelines recommend expectant management for patients with infrequent episodes of hemodynamically stable SVT, normal left ventricular function, and a normal resting ECG.27Referral to an arrhythmia specialist is indicated for patients with poorly tolerated arrhythmias. In reality, patients with AVNRT or AVRT are often referred early for ablation before extended trials of drug therapy. While management of patients with an asymptomatic WPW pattern on ECG is controversial, guidelines recommend referral of these patients to an arrhythmia specialist for further evaluation.27
Pharmacologic Treatment
Chronic prophylactic drug therapy is an option for patients with SVT who cannot self-terminate the arrhythmia. Frequency of SVT, patient age, and symptom burden should all be taken into account before considering daily prophylactic drug therapy for a sometimes infrequent condition. Pharmacotherapy is associated with side effects and often does not result in complete freedom from arrhythmia.
Both long-acting calcium channel blockers and beta blockers improve symptoms in 60%-80% of patients with SVT.23,28 Flecainide and propafenone are class Ic antiarrhythmic drugs that slow conduction and suppress automaticity and can thus result in marked reduction in frequency and duration of SVT episodes in some patients. These agents are contraindicated in patients with known structural heart disease because of an increased risk of ventricular arrhythmias.28,29 Flecainide may result in headaches, visual disturbances, mild abdominal pain, and nausea. These side effects may necessitate its discontinuation. Propafenone may be somewhat more universally tolerated but may be associated with a metallic taste. These antiarrhythmic drugs should be initiated and followed up by an electrophysiologist experienced in their use. For example, both drugs can result in facilitation of 1:1 conduction of atrial flutter and therefore must be coprescribed with an atrioventricular nodal blocker in the setting of certain atrial arrhythmias, including atrial fibrillation.
Alternative antiarrhythmic drugs include sotalol or dofetilide, both class III agents. Like the class Ic agents, these drugs have been used effectively in patients with AVRT, AVNRT, and atrial tachycardia. Class III antiarrhythmic drugs exert their effect in this setting through prolongation of refractory period, prevention of reentry propagation, and suppression of automaticity.30 Class III antiarrhythmic drugs carry the risk of long QT and torsades de pointes and must be managed by an electrophysiologist.
Given the high success rates and favorable safety profiles of diagnostic electrophysiology study followed by an attempt at catheter ablation, many patients choose this option early in their course. However, pharmacologic therapy is an important treatment option and can be well tolerated and effective in some patients.
Catheter Ablation
The first catheter ablations for SVT occurred in the early to mid-1980s and employed sequential intracardiac delivery of 2-10 direct current shocks to disrupt and ablate myocardial tissue, with shock energy deliveries as high as 300-400 J per delivery.31,32 Soon afterward, catheter-based radiofrequency ablation was found to have a superior efficacy and safety profile compared to direct current ablation32 and since the late 1980s has been extensively employed as a well-tolerated, often curative therapy for SVT. In general, guidelines recommend ablation for patients with recurrent SVT despite treatment or poorly tolerated SVT, although recommendations vary based on the category of SVT and known success rates (Table).27,33 Most SVT ablation is performed under conscious sedation. Between 2-5 multipolar electrodes are positioned in the heart via the femoral (and sometimes jugular) veins under fluoroscopic guidance. The catheter electrodes have sensing and pacing functions that are used for induction and localization of the reentrant circuit or ectopic focus. The mechanism of tissue destruction during radiofrequency ablation is thermal injury that occurs at tissue temperatures >50°C, and tissue temperatures of 60°C-70°C are often targeted. At electrode temperatures >100°C, plasma proteins may denature to form a coagulum on the catheter tip, decreasing the density of the current delivered and increasing impedance, both of which can limit lesion growth.10 Further, when temperatures approach 100°C, a steam pop may occur and, if epicardial, may result in cardiac tamponade.
Success and Recurrence Rates After Radiofrequency Ablation of Supraventricular Tachycardia
Complications of ablation for SVT are generally low, although they vary significantly depending on the arrhythmia being treated. One large multicenter study examining patients undergoing AVNRT, AVRT, and atrioventricular node ablation found low risks of death, stroke, myocardial infarction, tamponade, and arterial perforation. Procedures involving ablation near the septal aspect of the tricuspid valve (fast pathway input to the atrioventricular node) are more likely to be complicated by atrioventricular block. Other possible complications include pericardial and pleural effusions, pneumothorax, and damage to the coronary vasculature and valves, although these complications are rare.34
AVNRT Ablation
The standard technique for RF ablation of AVNRT initially targeted the fast pathway. Although effective (success rates >95%), fast pathway ablation for AVNRT carried a risk of complete heart block as high as 15% and was abandoned in favor of an approach targeted at modifying the slow pathway.4,34-37 In most patients, the slow pathway inputs to the atrioventricular node are located along the posterior tricuspid annulus near the coronary sinus ostium, several centimeters away from the fast pathway and the compact atrioventricular node. Ablation is performed by targeting specific electrograms and an area in the posteroseptal right atrium, often close to the roof of the coronary sinus ostium. Slow pathway modification results in an impressive success rate of 99% for permanent cure of AVNRT. However, the incidence of complete heart block remains 1%-1.5%, even in experienced hands.26,38,39 AVNRT ablation can be complex. In some patients, the location of the slow pathway is challenging. In other patients, the fast and slow pathways lie close to each other, resulting in an increased risk of atrioventricular block. In such cases, assessing the size of the triangle of Koch (either by three-dimensional [3-D] mapping, fluoroscopy, or measuring conduction time between coronary sinus and His-bundle catheters) can be helpful.40-42 Radiofrequency energy application at relatively low power and immediate termination of radiofrequency energy delivery if any evidence of atrioventricular block is observed reduce the incidence of long-term atrioventricular block.41
Recently, studies have focused on the use of cryoablation as an alternative to radiofrequency in AVNRT ablation.42-46 The tip of a cryoablation catheter freezes to −75°C, resulting in ice formation within the cell, rupture of the cell membrane, and permanent myocardial cell death. The cryoablation platform allows for freeze mapping, the creation of test lesions at approximately −4°C with reversible electrophysiologic effects. Freeze mapping allows the operator to test an ablation site for the effect on pathway conduction and also to monitor for atrioventricular block that is usually reversible at these temperatures. This effect is not completely reliable, however, and tissue function does not always recover after freeze mapping. The other advantage of cryoablation is that an ice ball forms on the tip of the catheter and adheres to the cardiac tissue, resulting in a high degree of catheter stability. An early study suggested similar efficacy of cryoablation compared with radiofrequency ablation for AVNRT, with a reduced risk of complete heart block.42 A larger study in 2004, however, found a significantly higher rate of recurrence compared to radiofrequency ablation because of the reversibility of cryoablative lesions.43 This study was not powered to detect differences in rates of complete heart block. In 2010, the CYRANO (Cryoablation Versus Radiofrequency Energy for the Ablation of Atrioventricular Nodal Reentrant Tachycardia) study demonstrated similar acute efficacy between radiofrequency and cryoablation (98.4% and 96.8%), although recurrence rates were much higher in the cryoablation group (9.4% vs 4.4% at 6 months). No difference was seen in the incidence of complete heart block.44 Notably, the “frosty” trial demonstrated significantly less recurrence in patients with AVNRT (94% of patients had no recurrence at 6 months).47 The current ICY-AVNRT (Intracardiac CrYoablation for AtrioVentricular Nodal Reentrant Tachycardia) trial is prospectively examining the efficacy of cryoablation for AVNRT.
Accessory Pathway Ablation
Success rates for accessory pathway ablation range from 95%-98%, with recurrence rates of AVRT as low as 2%, although location of the accessory pathway can have a significant effect on success rates (posteroseptal and right-sided pathways are more challenging).45-47 Accurate localization of the accessory pathway is key for successful ablation. The morphology of the delta wave and QRS complex is helpful in the preliminary localization of pathways with manifest preexcitation. Ablation of pathways located near the atrioventricular node (most commonly anteroseptal or midseptal pathways) carries an increased risk of atrioventricular block.46,47 Ablation with cryoablation has thus been attempted in such cases to reduce this risk. The “frosty” trial demonstrated a modest success rate of 69%, although there was no evidence of atrioventricular block. Success rates may be reduced in cases with unusual accessory pathway locations (eg, epicardial, atrial appendage, or atriofascicular) because of difficulties in catheter position or inadequate power delivery.11,47 Posteroseptal pathways are a challenging group of accessory pathways to ablate. Previous research has suggested that these accessory pathways can involve the musculature of the coronary sinus, and ablation within the coronary sinus may be necessary. In addition, diverticula in the proximal coronary sinus have been shown to be a region where some of these pathways can lie (Figure 6).48,49 More recently, 3-D mapping technology has allowed for the creation of computerized representations of the sequence of electrical activation and is sometimes used in the ablation of accessory pathways.45

Three-dimensional electroanatomical map (ESI system, St. Jude Medical) demonstrating a diverticulum of the coronary sinus containing a posteroseptal accessory pathway. A: ablation catheter electrograms. B: coronary sinus electrograms. The electrograms show 2 leads of the surface electrocardiogram with disappearance of the delta wave on the third beat and corresponding intracardiac electrograms below.
Accessory pathway ablation in patients with symptomatic preexcitation (ie, WPW pattern) or with preexcited rapid atrial fibrillation carries a class I level B recommendation in the ACC/AHA/ESC guidelines.27 Ablation in patients with asymptomatic preexcitation seen on the surface ECG is controversial. Population-based studies suggest that the incidence of sudden death in these patients is low. One study of 162 patients reported ventricular fibrillation as the presenting arrhythmia in 1.85%, although rates vary widely in the literature.50 Certain electrophysiologic characteristics (eg, accessory pathways with a short refractory period at electrophysiology study or the presence of multiple accessory pathways) carry a greater risk of developing atrial fibrillation with a critically fast ventricular response, so electrophysiology testing is often performed in patients with these characteristics, particularly younger patients. Electrophysiology testing may not be necessary in older asymptomatic patients because if SVT has not occurred by age 40, it is extremely unlikely that the first manifestation of a WPW pattern will be preexcited atrial fibrillation, although this assertion has been questioned.51
Atrial Flutter Ablation
Compared to relatively ineffective antiarrhythmic drug therapy, atrial flutter ablation is more successful in maintaining normal sinus rhythm.52 Typical atrial flutter ablation involves the creation of a complete bidirectional conduction block across the cavotricuspid isthmus. RF energy is applied in a point-by-point fashion or as a linear drag lesion from the tricuspid annulus to the inferior vena cava to create the line of conduction block. Pacing from the lateral right atrial and the coronary sinus is then performed to confirm isthmus block (Figure 7). Atrial flutter ablation is successful in more than 99% of cases, and recurrence rates are low.15,52,53 Atrial fibrillation and atrial flutter commonly coexist, and atrial fibrillation often occurs after ablation for atrial flutter, even in patients without documented preprocedure atrial fibrillation.54

Fluoroscopic catheter positions during typical atrial flutter ablation. A: around the tricuspid annulus (Halo catheter). B: in the coronary sinus. C: tip of the ablation catheter positioned on the cavotricuspid isthmus. Catheters A and B measure isthmus block. Ablation is performed with the catheter looping back on itself as in this example or with the catheter flat against the isthmus.
The maximum voltage-guided ablation approach has been proposed as an alternative method of atrial flutter ablation. Maximum voltage-guided ablation targets only anatomically important muscle bundles (identified as high-voltage electrograms) along the cavotricuspid isthmus instead of creating a single continuous ablation line. A post hoc analysis of the AURUM 8 study found that voltage-guided ablation significantly reduced ablation time, number of lesions, fluoroscopy time, and procedure duration.55
As indicated, atrial flutter may be atypical, arising from the right atrium or the left atrium. Atypical right atrial flutter may be caused by a right atrial scar or by a phenomenon known as upper-loop reentry in which the circuit is localized in the upper right atrium, utilizing a critical gap in the upper crista terminalis.56 The left atrial flutter circuit most commonly involves the mitral annulus, the insertion of the pulmonary veins into the posterior left atrium, an area of left atrial fibrosis, or a combination of these areas. The ablation procedure for atypical atrial flutter varies based on the location and complexity of the reentry circuit. In general, ablation is performed by transecting a critical area in the reentry circuit by a continuous line of RF ablation. Studies have reported an approximate 70% success rate with left atrial flutter ablation.57-59 As mentioned above, atrial fibrillation is often seen after atrial flutter ablation, and left-sided atrial flutter is commonly seen in this clinical situation.
Atrial Tachycardia Ablation
Atrial tachycardia ablation is indicated in patients with recurrent, symptomatic arrhythmia. In focal atrial tachycardia, accurate localization of the focus is required. The advent of 3-D mapping technology has significantly improved the efficacy of atrial tachycardia ablation. Maps demonstrate earliest local atrial activation and can be useful in mapping the chamber and identifying the atrial tachycardia circuit. Difficulty inducing atrial tachycardia at the time of electrophysiology study remains a significant challenge in as many as 12% of patients, and success rates of atrial tachycardia ablation reported in the literature range from 69%-100%.60 Recurrence rates may be as low as 8%.
Even with aggressive pacing maneuvers, sometimes only a few beats of atrial tachycardia may be induced during electrophysiology study. A technique known as noncontact balloon mapping has been used with some success in this situation, enabling the operator to create a complete atrial activation map utilizing just a single beat of atrial tachycardia. Electrodes on the surface of a balloon-tipped catheter are introduced into the atrium to sample thousands of anatomically distinct electrical signals during each cardiac cycle that are then extrapolated using the calculated geometry of the atrium to infer a sequence of activation. The accuracy of noncontact vs contact balloon mapping in ventricular arrhythmias is comparable,57 and the technique is currently being evaluated for atrial arrhythmias.61,62 Noncontact mapping of this type is only performed in the right atrium.
CONCLUSION
The term SVT encompasses a heterogeneous group of arrhythmias with different electrophysiologic characteristics. Knowledge of the mechanism of each SVT is important in determining management at the bedside and in the electrophysiology laboratory. In the acute setting, both vagal maneuvers and pharmacologic therapy can be effective in arrhythmia termination. RF ablation has revolutionized therapy for many SVTs, and newer techniques have significantly improved ablation efficacy and reduced periprocedural complications and procedure times. Cryoablation is currently being investigated as an alternative form of energy delivery, although the long-term effectiveness of this procedure currently limits its use for many SVTs.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care and Medical Knowledge.
Footnotes
Disclaimer: Owen A. Obel, MD, is a consultant for Medtronic and is on the speaker bureau for Medtronic and Biotronik. Otherwise the authors have no financial or proprietary interest in the subject matter of this article.
- © Academic Division of Ochsner Clinic Foundation








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}