
Abstract
Background Chest pain from coronary heart disease (CHD) accounts for more than 8 million emergency department visits every year in the United States, emphasizing the need for cardiovascular (CV) interventions to help reduce this high number. Meditation––a state of contemplation, concentration, and reflection––has the potential to help decrease CV disease.
Methods This article reviews the available data regarding the effects of meditation on various aspects of CV health.
Results During the past few decades, multiple studies have demonstrated the beneficial effects of meditation on various CV risk factors. In addition to decreasing CV mortality, meditation has also been shown to improve conditions such as hypertension, type 2 diabetes mellitus, dyslipidemia, and high cortisol levels. Still unclear is how current medical therapies impact overall CHD in comparison to meditation techniques.
Conclusion Prospective trials are needed to study the effects of meditation on CV risk factors, to provide guidelines for daily meditation practice, and to determine the efficacy of meditation compared to current pharmacologic therapies.
INTRODUCTION
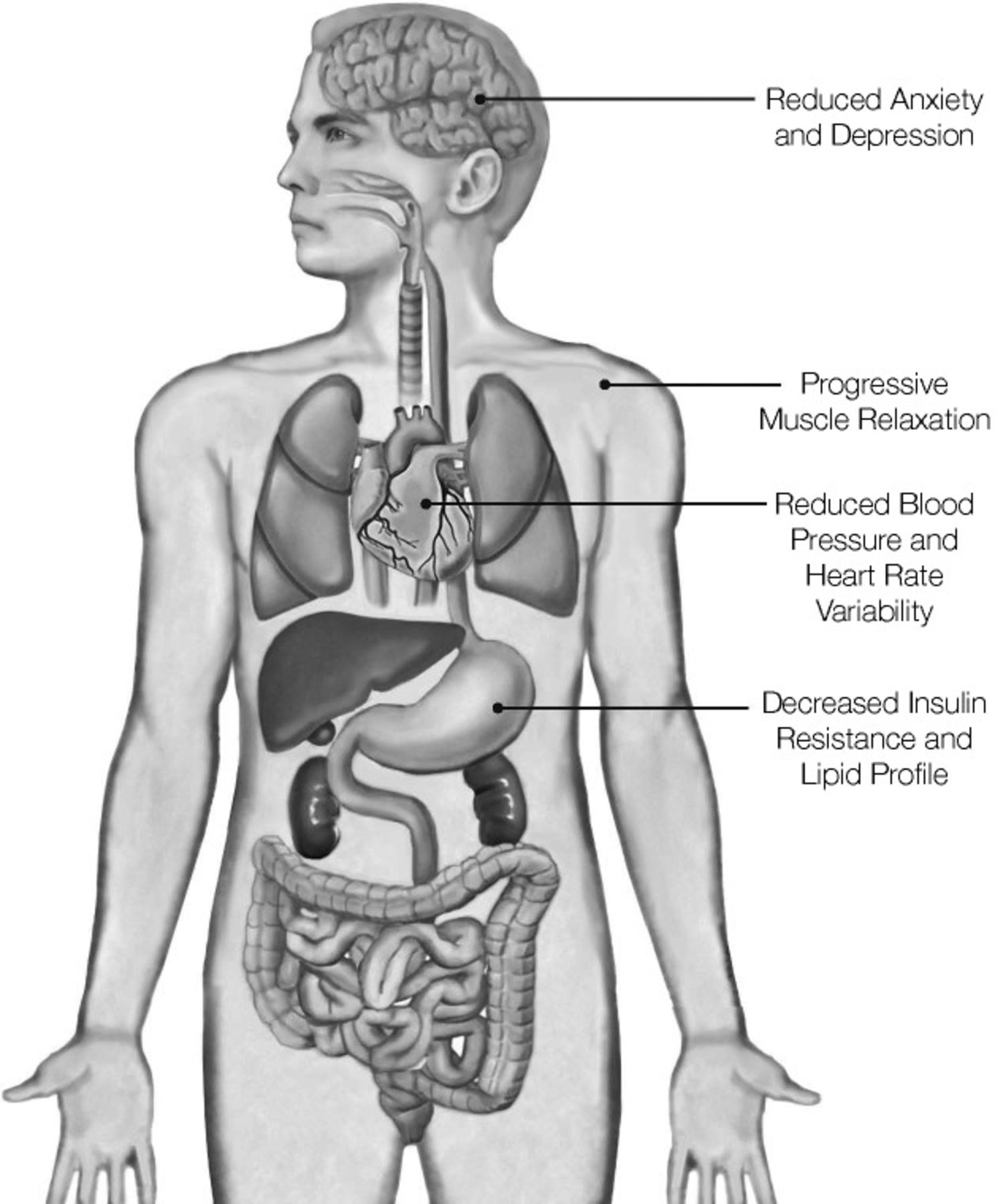
Meditation is a state of contemplation, concentration, and reflection that originated thousands of years ago as a practice that improves spiritual and emotional well-being. This discipline teaches the practitioner to examine thoughts, feelings, and sensations in a nonjudgmental fashion with the goals of achieving a state of inner calmness, physical relaxation, and psychological balance (Figure).

The effects of meditation on the body.
Various types of meditation are used today. Mantra meditation primarily involves the repetition of words that have phonetic significance, whereas mindfulness meditation generally refers to practices that cultivate awareness and requires paying attention to the present moment. Yoga includes a group of techniques incorporating postures, breath control, and meditation that originated in India. Tai chi and qigong are meditation practices related to Chinese martial arts and traditional Chinese medicine.
Chest pain from coronary heart disease (CHD) accounts for more than 8 million emergency room (ER) visits every year in the United States.1 Each year, patients presenting with symptoms suggestive of acute coronary syndrome and myocardial infarction (MI) account for as many as 10% of hospital ER cases and up to 25% of all admissions.2,3 These numbers represent a considerable burden on healthcare resources, as the cost of treating these patients is approximately $286 billion annually, or roughly 17% of healthcare expenditures,4 emphasizing the need for cardiovascular (CV) interventions such as meditation to help alleviate this problem.
During the past few decades, awareness of the application of meditation or other forms of mind-body therapy in the healthcare setting has increased. Multiple studies have demonstrated the beneficial effects of meditation on various aspects of CV health (Table). This article reviews the available data and discusses avenues for future research.
Benefits of Meditation
PSYCHOLOGICAL RISK FACTORS AND CHD
During the past 50 years, many studies have established a correlation between psychological risk factors (anxiety, depression, and hostility) and CHD.5 Roest et al showed that depression is independently associated with CV mortality.6 Substantial evidence suggests that anxiety7 and hostility8 negatively impact CV health.
The mechanism behind these associations, however, is not clear and is likely multifactorial. Psychological stress (PS) has multiple implications in coronary artery disease that can be categorized into behavioral mechanisms and direct pathophysiologic mechanisms.9 Behavioral mechanisms are demonstrated when increased PS increases the frequency of negative practices, such as alcoholism, smoking, poor diet, and patient medical noncompliance.10 Additionally, elevated PS contributes to direct pathophysiologic processes that increase the risk of coronary artery disease. Chronic increases in PS have been implicated in significant impairment of platelet function, including enhanced platelet reactivity and release of platelet products such as platelet factor 4 and β-thromboglobulin.11,12 In animal models, most notably the work done with the Macaca fascicularis monkey, chronic PS has been clearly demonstrated to lead to atherosclerosis exacerbation, endothelial dysfunction, and even necrosis.13 Kaplan et al postulated that this accelerated atherosclerosis phenomenon was secondary to upregulation of the sympathetic nervous system and excess catecholamines.13 Further review reveals that chronic PS is associated with elevated cortisol levels, ovarian dysfunction, and excessive adrenergic activation, all of which herald accelerated atherosclerosis.9
While chronic PS increases the risk for developing coronary artery disease, acute PS can trigger MI, arrhythmogenicity, and coronary vasoconstricton.14 Additionally, acute PS can activate platelet function and promote endothelial dysfunction, both of which can culminate in adverse cardiac events. A 2012 review of the medical literature demonstrated that acute PS can increase sympathetic output, impair endothelial function, and create a hypercoagulable state.15 These changes have the potential to allow plaque rupture and precipitate intraluminal thrombosis, resulting in MI or sudden death.
The literature suggests that PS affects the autonomic nervous system by increasing catecholamines (such as norepinephrine) and suppressing vagal tone. PS may lead to reduced heart rate (HR) variability, increased resting HR, and delayed postexercise HR recovery.16,17 In addition, PS may lead to inflammation, oxidative stress, and abnormal coronary artery tone,18 as well as platelet activation.19 PS can also increase CV work and hemodynamic shear stress.16 All these factors increase the risk of CV events.
Studies have shown that meditation practices have a beneficial effect on psychological risk factors.20-22 A study published in 2010 enrolled 42 volunteers to evaluate the effects of progressive self-focus meditation.23 Participants were divided into 2 groups: 1 that participated in weekly 1-hour training sessions for 5 weeks and 1 waiting-list control group. After 5 weeks, the meditation group had a significant depression score reduction and an increase in attention compared with the control group. Zeidan et al evaluated the benefits of brief mindfulness meditation sessions on mood and CV variables such as HR and blood pressure (BP) compared to sham meditation.24 The study included 82 undergraduate students (34 males and 48 females) with no prior meditation experience. They participated in 3 training sessions for mindfulness meditation or sham mindfulness meditation, or they were randomized to a control group. The study concluded that meditation intervention was more effective at reducing negative mood, depression, fatigue, confusion, and HR compared to the sham and control groups.
A study evaluating 41 participants who had sustained acute coronary syndrome in the previous 6-18 months assessed a 4-day spiritual retreat's effects on depression and other measures of well-being compared to a lifestyle change program and a control group (usual cardiac care).25 The spiritual retreat included guided imagery, meditation, drumming, journal writing, and nature-based activities. The lifestyle program included nutrition education, exercise, and stress management. Both retreat groups received follow-up phone coaching twice a week for 3 months. At baseline, the spiritual retreat group had the highest depression scores, but this group had significantly lower depression scores at all postintervention time points (P≤0.002). Although several measures improved in all 3 groups by 6 months, the spiritual retreat group had immediate improvement after the retreat. This result was maintained for the duration of the study over 3 months.25
In 2012, Barnes and Orme-Johnson published an update on a specific form of meditation known as transcendental meditation (TM),26 a practice that has been shown to reduce sympathetic nervous system activation. Dillbeck and Orme-Johnson reported that acute reductions in respiratory rate and plasma lactate occur during TM practice while control subjects sitting with their eyes closed have increased basal skin resistance.27 Additionally, the subjects practicing TM had a lower baseline HR and respiratory rate, a lower plasma lactate level, and spontaneous skin resistance responses outside of meditation.27
Delui et al studied meditation in patients with cardiovascular disease and depression.28 The 45 patients were randomly assigned to 3 groups: relaxation, meditation, or control. After completing the Beck depression scale and a self-assessment of anxiety, patients underwent a series of 10 sessions of physical muscle relaxation (PMR) or mindfulness meditation, or they received no intervention. Significant reductions in depression scores, systolic blood pressure (SBP), and HR were seen in the meditation group compared with the control group.
Additional studies on the relationship between PS and CHD have been performed on various patient demographics. In a study published in 2014, 5,313 men and women of Hispanic or Latino ethnic backgrounds were scored on their chronic stress burden, based primarily on self-reported stress from domains including finances, work, relationships, health, drug or alcohol use, or additional stressors. After adjusting for sociodemographic, behavioral, and biological risk factors, patients with higher chronic stress burden scores had an increased prevalence of CHD, stroke prevalence, diabetes, hypertension, and smoking.29
In African American subjects, PS has been determined to play a role in the development of metabolic syndrome. By monitoring endothelial dysfunction, the effect of consciously resting meditation (a sound-based meditation) was compared with a control intervention of health education. Sixty-eight African Americans with metabolic syndrome risk factors were randomized to either the meditation or health education group and monitored for 1 year. Endothelial function was assessed by brachial artery flow-mediated dilation at baseline and at 6 and 12 months. Arterial elasticity, metabolic syndrome risk factors, and psychosocial and behavioral variables were also monitored. After 1 year, flow-mediated dilation improved in the meditation group but was not significantly higher than the flow-mediated dilation in the health education group. No significant change in arterial elasticity was seen in either group. However, most metabolic syndrome risk factors showed beneficial trends in the meditation group only.30
Evidence has linked meditation with reductions in prehypertension. Hughes et al studied mindfulness-based stress reduction (MBSR), an organized protocol of mantra and breathing-focused meditation, in 56 male and female patients with unmedicated prehypertension.31 The MBSR group was compared to a group randomized to receive PMR therapy. Participants received 8 weeks of MBSR or PMR sessions administered by a treatment provider and lasting approximately 2.5 hours each week. BP obtained in the clinic was the primary outcome measure. Patients randomized to the MBSR arm exhibited a 4.8 mmHg reduction in SBP and a 1.9 mmHg reduction in diastolic blood pressure (DBP) compared to a 0.7 mmHg reduction in SBP and an increase in DBP in the PMR group.31
As stated earlier, psychological risk factors are associated with CHD. Participation in meditation practices has been shown to reduce depression, anxiety, and negative mood and thus may have an indirect positive effect on CV health and well-being. This possibility has led the American Heart Association to classify TM as a class IIb, level of evidence B alternative approach to lowering BP.32
MEDITATION AND CHD MORTALITY
One of the earliest studies to evaluate the effects of TM on mortality was published in 1989.33 Seventy-three residents of 8 homes for the elderly were randomly assigned to a no-treatment group or 1 of 3 treatment groups: the TM program, mindfulness training in active distinction-making, or a relaxation (low mindfulness) program. The mean age of the study population was 81 years. After 3 years, the survival rate was 100% for the TM group and 87.5% for the mindfulness training group in contrast to lower rates for the other groups.33 A 15-year follow-up of this study demonstrated that the TM group had a lower CV mortality rate than the combined control subjects after adjusting for age, gender, and pretest SBP.34
A metaanalysis of 23 randomized controlled trials determined that the addition of psychosocial interventions, including meditation, breathing exercises, and physical relaxation techniques, in addition to standard cardiac rehabilitation regimens improved outcomes among patients with CHD.35 The metaanalysis evaluated a total of 3,180 participants––2,024 patients who received psychosocial treatment vs 1,156 control subjects. Linden et al observed in this analysis that psychosocially treated patients showed enhanced reductions in psychological distress, SBP, HR, cholesterol levels, and blood pressure compared to the control group. Furthermore, patients who did not receive psychosocial treatment showed greater mortality and adverse CV event rates during the first 2 years of follow-up with a log-adjusted odds ratio of 1.70 for mortality (95% confidence interval [CI], 1.09-2.64).35
Another metaanalysis of 37 studies evaluated the effects of psychoeducational programs.36 The analysis showed that these programs resulted in a 34% reduction in CV mortality, a 29% reduction in recurrence of MI, and significant positive effects on BP, cholesterol, body weight, smoking behavior, physical exercise, and eating habits (P<0.025).
A pooled analysis combined data from a study of 77 white American men and women (mean age 81 years) with data on 125 African American men and women (mean age 66 years) from another randomized trial.37 Mean follow-up was 7.6 ± 3.5 years. Compared with combined controls, the TM group showed a 30% decrease in the rate of CV mortality (relative risk 0.70, P=0.045) and a 23% reduction in all-cause mortality (relative risk 0.77, P=0.0399). These results suggest that the prevention and control of high BP through TM may contribute to decreased mortality from CV causes in elderly patients who have systemic hypertension.
In a controlled trial, 201 African American men and women with CHD were randomized to a TM program or a health education group.38 The primary endpoint was all-cause mortality, MI, or stroke. During the 5.4 year follow-up, the TM group had a 48% risk reduction in the primary endpoint (hazard ratio 0.52; 95% CI, 0.29-0.92; P=0.025). The data also demonstrated reductions of 4.9 mmHg in SBP (95% CI, 8.3-1.5 mmHg; P=0.01) and anger expression (P<0.05 for all scales).
Jayadevappa et al analyzed 23 African American patients hospitalized for congestive heart failure who were randomly assigned to a program of either TM or routine health education.39 After 6 months, the TM group had a significant increase in their 6-minute walk distance as well as improvement in depression scores and quality of life measures. Throughout the 6-month study period, the meditation group had a reduced number of hospitalizations compared to the health education group, indicating the possible mitigation of symptoms.
Although the data suggest a beneficial relationship between meditation and mortality, further studies are needed to assess the effects of meditation on mortality, especially among patients after MI and patients with congestive heart failure.
MEDITATION AND CV RISK FACTORS
During the past few decades, the effects of meditation on hypertension have been debated, and studies have shown conflicting results. A 1993 metaanalysis involving 1,264 patients attempted to assess the efficacy of cognitive behavioral therapies (such as biofeedback, relaxation, and meditation) on essential hypertension.40 Overall, the study concluded that cognitive interventions for essential hypertension are superior to no therapy but not superior to credible sham techniques or to self-monitoring alone.
Another study published in 1995 tested the short-term efficacy of 3 approaches––TM, PMR, or lifestyle modification exercise––on the treatment of mild hypertension in 127 elderly African Americans.41 The study was a randomized, controlled, single-blind trial with 3 months of follow-up in a primary care, inner-city health center. Groups using mental and physical stress reduction approaches (TM and PMR) were compared with a group using a lifestyle modification education control program and with each other. The primary outcome measures were changes in DBP and SBP from baseline to final follow-up, measured by blinded observers. Adjusted for significant baseline differences and compared with the control, TM reduced SBP by 10.7 mmHg (P<0.0003) and decreased DBP by 6.4 mmHg (P<0.0005). PMR lowered SBP by 4.7 mmHg (P=0.0054) and DBP by 3.3 mmHg (P<0.02). The reductions in the TM group were significantly greater than in the PMR group for both SBP (P=0.02) and DBP (P=0.03).
A 2008 metaanalysis looked at randomized controlled trials through 2006, comparing BP responses to TM to a control group. The analysis included 9 randomized controlled trials with subjects ranging in age from adolescent (mean age 16 years) to senior (mean age 81 years), including normotensive, prehypertensive, and hypertensive individuals meeting eligibility criteria.42 Anderson et al found that the TM program lowered SBP an average of 4.7 mmHg and DBP 3.2 mmHg compared with control groups. Subgroup analyses of the hypertensive groups and high-quality studies showed similar BP reductions in all groups.42
Rainforth et al identified 107 studies on the effects of stress reduction programs on BP, including 17 trials with 23 treatment comparisons and 960 participants with elevated BP.43 The stress reduction programs included relaxation, meditation, and biofeedback. Overall, no significant decrease in BP was seen among patients who underwent biofeedback, PMR, or stress management. However, the analysis showed a significant (P=0.002/0.02) SBP decrease of 5 mmHg and a 2.8 mmHg decrease in DBP among subjects who practiced TM.
Gregoski et al evaluated the effect of breathing awareness meditation (BAM), Botvin LifeSkills Training, and health education control on ambulatory BP and sodium excretion in African American adolescents.44 They found significant group differences for changes in overnight SBP and DBP and HR during the 24-hour period and during school hours. Participants in the BAM treatment group exhibited the greatest overall decreases on these measures (Bonferroni adjusted, P<0.05). The researchers concluded that BAM appeared to improve hemodynamic function and may affect sodium handling among African American adolescents who are at increased risk for developing CV diseases.
Meditation has also been linked with beneficial effects on insulin resistance and lipid profiles. A study of 103 subjects with stable CHD examined the efficacy of TM on components of the metabolic syndrome and CHD.45 Main outcome measures included BP, lipoprotein profiles, and insulin resistance. The study demonstrated that the TM group had beneficial changes in adjusted SBP (−3.4 ± 2.0 vs 2.8 ± 2.1 mmHg; P=0.04), insulin resistance (−0.75 ± 2.04 vs 0.52 ± 2.84; P=0.01), and HR variability (0.10 ± 0.17 vs −0.50 ± 0.17 high-frequency power; P=0.07) compared with the control group. However, no significant decreases in levels of total cholesterol, lipoproteins, and high-sensitivity C-reactive protein were seen, perhaps because of the high prevalence of statin use and near-optimal low-density lipoprotein cholesterol levels.
Cooper and Aygen compared 12 patients with hypercholesterolemia who regularly practiced meditation with 11 control subjects who did not practice meditation and found a 10% (P<0.005) reduction in fasting serum cholesterol levels in those who practiced meditation during a 13-month period.46 Another study demonstrated the postprandial hypoglycemic effect of sitting breathing meditation exercise on 50 patients with type 2 diabetes mellitus and a mean age of 63.1 years.47 Participants' levels of postprandial plasma glucose were significantly reduced by 19.26 ± 30.99 mg/dL, (P<0.001) at the second visit and by 17.64 ± 25.48 mg/dL (P<0.001) at the third week visit.
Another risk factor for CHD is elevated levels of plasma cortisol. In the Edinburgh study that included 919 patients (mean age 67.9) with type 2 diabetes mellitus, elevated plasma cortisol levels were associated with raised fasting glucose and total cholesterol (P<0.001) and with prevalent ischemic heart disease, independent of conventional risk factors.48 A study published in 1979 examining cortisol levels in 16 patients who were randomized into TM or control groups did not find any acute inhibitory effects of TM on secretion of rennin, aldosterone, or cortisol in the unstressed state.49 However, in the stressed state (following venipuncture), a consistent significant rise in cortisol occurred in the controls, while patients participating in meditation did not show this effect. Michaels et al concluded that chronic practice of TM may not directly influence cortisol in the unstressed state but could blunt the response to stress.49
In a study of postmenopausal women with similar risk of CV disease, Walton et al compared cortisol levels in patients who were long-term practitioners of TM with cortisol levels in patients who were not. Sixteen women who practiced TM for a mean of 23 years were matched to 14 controls. Cortisol response to a metabolic stressor (75g of glucose, orally) was tested in saliva and urine. Postglucose cortisol rose significantly faster in the control group than in the TM group. In addition, urinary excretion of cortisol was 3 times higher in the control group.50
Despite the numerous studies and metaanalyses of the studies on meditation in its various forms, investigators for the Agency for Healthcare Research and Quality reported that solid conclusions on the effects of meditation practices in healthcare cannot be drawn based on the available evidence.51 Further research on meditation practices should be conducted with an emphasis on design and implementation, as well as on analysis and result reporting.
FUTURE RESEARCH
Patients with CV risk factors such as hypertension and type 2 diabetes mellitus would likely benefit from meditation. Prospective trials are needed to study the effects of meditation on CV risk factors such as lipid profile, C-reactive protein, type 2 diabetes mellitus, and hypertension. Future studies are also needed to provide guidelines (duration, frequency) for daily use of meditation in everyday life.
It is still unclear how current medical therapies such as statins, beta blockers, and angiotensin-converting enzyme inhibitors impact overall CHD in comparison to meditation therapy. Further studies are needed to examine this effect. While aggressive lifestyle modification augments the beneficial effects of medications, it is still not certain how much benefit meditation as a lifestyle modification will bring to this paradigm of disease prevention or amelioration.
CONCLUSION
Meditation is believed to be efficacious in reducing sympathetic activity, lowering cortisol levels via modulation of the hypothalamic pituitary adrenal pathway, and reducing negative behavioral activity. Studies have shown that in addition to decreasing CV mortality, the beneficial effects of meditation improve conditions such as hypertension, type 2 diabetes mellitus, dyslipidemia, and high cortisol levels. However, future studies on the effects of meditation on health are essential to establish a nonbiased view of this emerging landscape.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care and Medical Knowledge.
Footnotes
The authors have no financial or proprietary interest in the subject matter of this article.
- © Academic Division of Ochsner Clinic Foundation








{kind=link}