
Abstract
Background Stress-induced cardiomyopathy, also known as takotsubo cardiomyopathy, is not fully understood. It is thought to occur in patients who have signs and symptoms consistent with acute myocardial infarction but display no obstructive coronary lesions during heart catheterization. Characteristics include transient left ventricular dysfunction, wall motion abnormalities on echocardiogram, new electrocardiographic ST-segment changes, and the occurrence of a precipitating stressor.
Case Report We present a patient who underwent Heller myotomy and suffered acute heart failure in the immediate postoperative period. Left heart catheterization revealed clean coronary arteries, and the patient fully recovered days later. While difficult to fully exclude drug-related causes, we believe this case to be consistent with takotsubo cardiomyopathy.
Conclusion This unusual postoperative complication following uneventful laparoscopic surgery should be kept in mind when unsuspected cardiovascular compromise is seen in the early perioperative recovery period. In addition to the rare occurrence of acute coronary ischemia syndromes and possible perioperative pulmonary embolic events, cardiovascular decompensation related to acute stress syndromes or idiopathic pharmacologic responses must be considered. Even patients who seem most healthy can have complications that warrant immediate attention and treatment.
INTRODUCTION
Stress-induced cardiomyopathy (SCM), also known as takotsubo cardiomyopathy or broken heart syndrome, is not fully understood. It is thought to occur in patients who have signs and symptoms consistent with acute myocardial infarction but display no obstructive coronary lesions during heart catheterization. Characteristics include transient left ventricular dysfunction, wall motion abnormalities on echocardiogram, new electrocardiographic ST-segment changes, and the occurrence of a precipitating stressor.1-4
We present an unusual circumstance of idiopathic acute heart failure following an uneventful laparoscopic esophagomyotomy to manage progressive dysphagia from achalasia of the esophagus.
CASE REPORT
A 59-year-old African American man with a diagnosis of achalasia of the esophagus established 2 years previously presented with a complaint of progressive dysphagia, fatigue, and a recent 30-pound weight loss. Esophageal manometric testing performed at the time of the original diagnosis demonstrated the classic findings of aperistaltic, low-amplitude esophageal contractions and an absence of lower esophageal relaxation in response to swallowing. He had experienced relief of his symptoms with endoscopic esophageal intramuscular injection of botulinum toxin shortly after diagnosis, but significant dysphagia had returned 6 weeks prior to this presentation. An esophagram revealed dilation of the intrathoracic esophagus and a smooth bird-beak tapering of the distal esophagus at the gastroesophageal junction, consistent with achalasia (Figure 1). The decision was made to perform a laparoscopic Heller myotomy with Dor fundoplication.

Barium esophagram reveals bird-beak tapering at the gastroesophageal junction and a dilated esophagus.
The patient had no other significant medical history and, specifically, no history of cardiovascular disease. He denied any history of chest pain or shortness of breath and stated he routinely achieved 4 METS (metabolic equivalents) of activity without any adverse symptoms.
Preoperative workup 1 week prior to surgery included a chest x-ray and a 2-dimensional (2-D) echocardiogram. The echocardiogram revealed normal biventricular systolic function with an estimated left ventricular ejection fraction of 60%-65%. Diastolic function was normal, and the patient had no valvular abnormalities. His preoperative chest x-ray was normal (Figure 2). On the day of the procedure, he denied any changes in symptoms, acknowledged continued dysphagia limiting oral intake, and reported he was otherwise in his normal state of health. His vital signs were stable with a heart rate of 56 bpm and blood pressure of 107/65 mmHg preprocedure. He was given 2 mg of midazolam in the preoperative area and was transported to the operating room. The patient was monitored via pulse oximeter, blood pressure cuff, and electrocardiogram (ECG). Anesthesia was induced intravenously with 150 mg of propofol and 100 μg of fentanyl. He was paralyzed with rocuronium and intubated without incident. Fiber-optic bronchoscopy after induction of anesthesia revealed mild bilateral changes of tracheobronchitis with minimal secretions bilaterally. A right, lower lobe bronchoalveolar lavage resulted in no bacterial growth. Esophagogastroduodenoscopy demonstrated moderate dilation of an amotile esophagus. The lower esophageal sphincter was noted at 41 cm from the incisors, and the sphincter failed to open with vigorous attempts of local insufflations. The sphincter was traversed with gentle persistent pressure applied by the tip of the flexible esophagoscope. The characteristic pop felt with release of the sphincter's muscular resistance was appreciated as the esophagoscope entered the proximal stomach. The stomach, pylorus, and duodenum demonstrated mild superficial inflammatory changes. After completion of these endoscopic interventions, the patient's abdomen was prepped, and intraabdominal access was achieved with an OPTIVIEW trocar (Ethicon US, LLC) under visualization after adequate carbon dioxide insufflations at 15 mmHg were established. A total of 5 ports were utilized for instrument and videoscope access. After anterior dissection of the phrenoesophageal ligament and mobilization of the anterior vagal pedicle over the lower 5 cm of the esophagus, as we have previously described,5 3 mL of 1:10,000 epinephrine/saline solution was injected into the anterior esophageal muscular/submucosal wall and the gastric submucosa around the gastroesophageal sling fibers to facilitate a plane of dissection and to enhance hemostasis during the esophagomyotomy. A Heller myotomy was performed extending proximally 5 cm from the gastroesophageal muscular sling fibers and distally to the submucosal venous plexus beyond the muscular sling fibers of the gastric cardia, ensuring a complete esophagomyotomy. A standard Dor fundoplication was then performed, with the esophagoscope left in place within the stomach to prevent excessive narrowing at the gastroesophageal junction during the fundoplication and to later assess the integrity of the esophagogastric mucosa and the adequacy of the myotomy.

Preoperative chest x-ray shows no abnormal findings.
The intraoperative course was uneventful, with minimal blood loss and completion of the procedure in 38 minutes. The patient experienced one brief period of hypertension that responded to treatment with metoprolol, intravenous (IV) fentanyl, and deepening of the anesthetic. He was otherwise hemodynamically stable throughout the procedure. He received a total of 2,200 mL of crystalloid and did not require any blood products. He was extubated in the operating room and taken in stable condition to the recovery room for postoperative monitoring.
In recovery, the patient remained on a facemask at 6 L of supplemental oxygen. He was noted to be hypotensive, with systolic blood pressures ranging from 80-90 mmHg and diastolic pressures ranging from 50-60 mmHg. Although his breathing did not appear labored, he had copious respiratory secretions and could not be weaned off supplemental oxygen because of persistent hypoxia. Physical examination demonstrated bilateral crackles. A chest x-ray revealed widespread airspace consolidation, concerning for pulmonary edema (Figure 3). An ECG was negative for ischemia, estimated by a lack of ST-segment elevation, and no cardiac conduction abnormality was appreciated (Figure 4). An arterial blood gas panel revealed pH 7.34, Pco2 56, Pao2 129, and HCO3 30. Because of the patient's worsening cardiorespiratory status, the cardiology team was consulted. A stat 2-D bedside echocardiogram revealed generalized hypokinesis of the inferolateral, basal, and midinferior wall, along with a hypokinetic apical septum. Left ventricular systolic function was severely depressed, with an estimated ejection fraction of 20%-25%. Right ventricular systolic function was normal. Cardiac biomarkers were significant for elevated troponin I of 4.29 ng/mL (normal range 0-0.026 ng/mL) and CPK-MB of 13.0 ng/mL (normal range 0.1-6.5 ng/mL). The patient was given 40 mg of IV furosemide, with no improvement in his respiratory status. He was then re-intubated and transferred to the intensive care unit for further management. Aspirin and clopidogrel (Plavix) were started because of his elevated troponin levels. Heparin was not administered because of his recent surgery. An arterial line was inserted for better hemodynamic monitoring. The patient did not require vasopressor therapy, and his blood pressure remained in the range of 90-130/57-85 mmHg overnight.
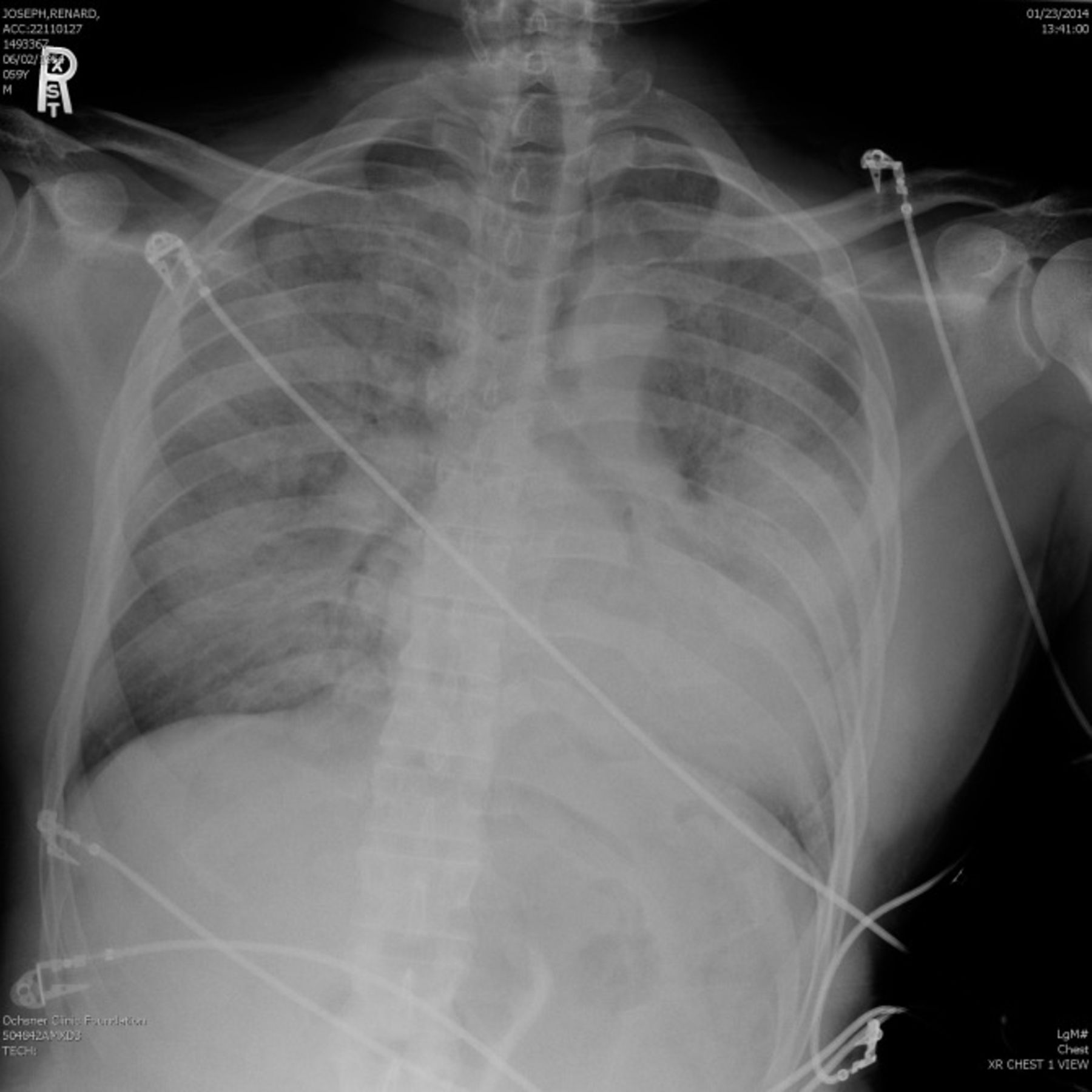
Postprocedure chest x-ray demonstrates acute onset of widespread airspace consolidation involving the lungs bilaterally and symmetrically, consistent with pulmonary edema and acute respiratory distress syndrome.

Electrocardiogram performed postoperatively does not reveal any ST-segment changes.
On postoperative day (POD) 1, left heart catheterization showed that normal left main, left anterior descending, left circumflex, and right coronary arteries had no blockages. A transthoracic echocardiogram showed left ventricular function was still depressed, with an estimated ejection fraction of 20%-25%. This echocardiogram also revealed a worsening of right ventricular systolic function that appeared severely depressed. No comment was made regarding diastolic function. Ultimately, the patient's lung function improved, and he was weaned off the ventilator and extubated on POD 3. A barium esophagram performed on POD 4 demonstrated a free flow of barium into the stomach without evidence of mucosal leak. The patient was discharged home on POD 5 on a soft postfundoplication diet. An outpatient echocardiogram performed 2 weeks after surgery demonstrated a return to normal left ventricular systolic and diastolic function, with an estimated ejection fraction of 55%-60%. Right ventricular size and function were also reported as normal. At his postoperative visit, the patient reported complete resolution of his dysphagia and denied any further cardiopulmonary symptoms.
DISCUSSION
Laparoscopic abdominal surgery is one of the most common surgical approaches used today. Laparoscopic management of achalasia of the esophagus with Heller myotomy has become a standard first-line management approach for this neuromotor esophageal condition. Cardiovascular complications occurring during laparoscopic surgery are rare, with a reported incidence <0.02%.5,6 A review of the literature did not reveal any reports of postoperative cardiac complications directly resulting from this procedure, making our case even more unique.7
Our hypothesis is that our patient suffered myocardial stunning or SCM in the immediate postoperative period, the cause of which is not completely understood. SCM is thought to be precipitated by severe acute physical or emotional stress and may account for as many as 2%-3% of patients presenting with signs and symptoms of acute myocardial infarction.1 Our patient's 30-pound weight loss and progressive fatigue may have been the precipitating events leading to his acute myocardial stunning. Clinical characteristics of SCM include transient left ventricular dysfunction, minimal or absent coronary artery obstruction, wall motion abnormalities on echocardiogram, new ECG ST-segment elevation or T-wave inversion, and the occurrence of a precipitating stressor.1,2 The most common echocardiogram findings are transient hypokinesis, akinesis, or dyskinesis of the left ventricular mid-segments, with or without apical involvement.3 Our patient did not experience any ECG changes; however, this finding does not exclude the diagnosis. Although ECG changes occur in many of these patients, in a 2010 case series report of more than 600 patients, 40% had normal ECGs at presentation.2 The pathophysiology is not completely understood but is thought to be related to catecholamine-induced myocardial stunning.3 In this same series, >90% of patients had elevated troponin levels, as our patient did. In 2008, researchers at the Mayo Clinic proposed criteria to diagnose takotsubo cardiomyopathy (Table).4
Mayo Clinic Proposed Diagnostic Criteria for Apical Ballooning Syndrome
Another hypothesis is that our patient may have suffered an adverse reaction to some of the medications he received intraoperatively. Case reports exist of patients developing acute, transient heart failure after general anesthetic with propofol and fentanyl induction;4,8,9 however, in our opinion, these reports do not establish a clear cause and effect relationship. In one of these reports,8 the possibility of SCM is ruled out because the patient's echocardiogram showed biventricular dysfunction and global hypokinesis. Additionally, the patient had absent ECG findings. In the second report,9 the possibility of SCM is not addressed. We know that propofol and fentanyl cause a decrease in systemic vascular resistance that is enhanced when these drugs are given in combination;10 however, this enhanced decrease in vascular resistance has the most clinical relevance in patients with limited cardiovascular reserve and is dose dependent. Our patient received a conservative dose of both propofol and fentanyl on induction. Furthermore, our patient had had a procedure under general anesthesia 2 months prior and was induced with a combination of propofol and fentanyl with no complications, making an adverse drug reaction unlikely.
CONCLUSION
The unusual postoperative complication of acute heart failure following uneventful laparoscopic surgery should be kept in mind when unsuspected cardiovascular compromise is seen in the early perioperative recovery period. While we cannot establish an exact diagnosis, SCM appears to be the most likely. The important lesson is that when diagnosed and treated quickly, most patients can fully recover as our patient did. All patients undergoing surgical procedures should be monitored carefully for cardiovascular instability in the postoperative period, regardless of their preoperative clinical status and the perceived uneventful nature of the operative intervention. In addition to the rare occurrence of acute coronary ischemia syndromes and possible perioperative pulmonary embolic events, cardiovascular decompensation related to acute stress syndromes or idiopathic pharmacologic responses must be considered. As in this case, even patients who seem most healthy can have complications that warrant immediate attention and treatment.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care and Medical Knowledge.
Footnotes
The authors have no financial or proprietary interest in the subject matter of this article.
- © Academic Division of Ochsner Clinic Foundation








{kind=link}
{kind=link}
{kind=link}
{kind=link}