
Abstract
Background Transposition of the great arteries (TGA) is a congenital heart defect that is associated with congestive heart failure, tricuspid regurgitation, and arrhythmias.
Methods This review identifies and critiques the existing methods of assessing and managing TGA with a focus on right ventricular function.
Results Echocardiography with novel strain methods and cardiac magnetic resonance imaging (MRI) are noninvasive imaging options, with cardiac MRI being the gold standard. Cardiopulmonary stress testing can be used to determine the severity of symptoms. For the medical management of right ventricular dysfunction in TGA, a closely monitored dosage of beta blockers and the concomitant use of diuretics for symptomatic relief have the strongest supporting data. Surgical options for patients with TGA include the insertion of a pacemaker to treat arrhythmias, which are more common in this population, or tricuspid valve replacement to alleviate systemic tricuspid regurgitation. If symptoms in a patient with TGA are not alleviated by these management techniques, more advanced options include the use of an Impella device (Abiomed), the insertion of ventricular assist devices, or orthotopic heart transplant.
Conclusion Physicians managing patients with TGA should take a multidisciplinary specialist approach to decide which route to pursue (medical or surgical) and when more advanced treatment options are necessary.
- Heart defects–congenital
- heart failure
- heart ventricles
- transposition of great vessels
- ventricular dysfunction
INTRODUCTION
Transposition of the great arteries (TGA) is a cardiac defect that accounts for 5%-7% of all congenital heart defects.1 In 2000, approximately 11,000 adults had TGA in the United States alone.2
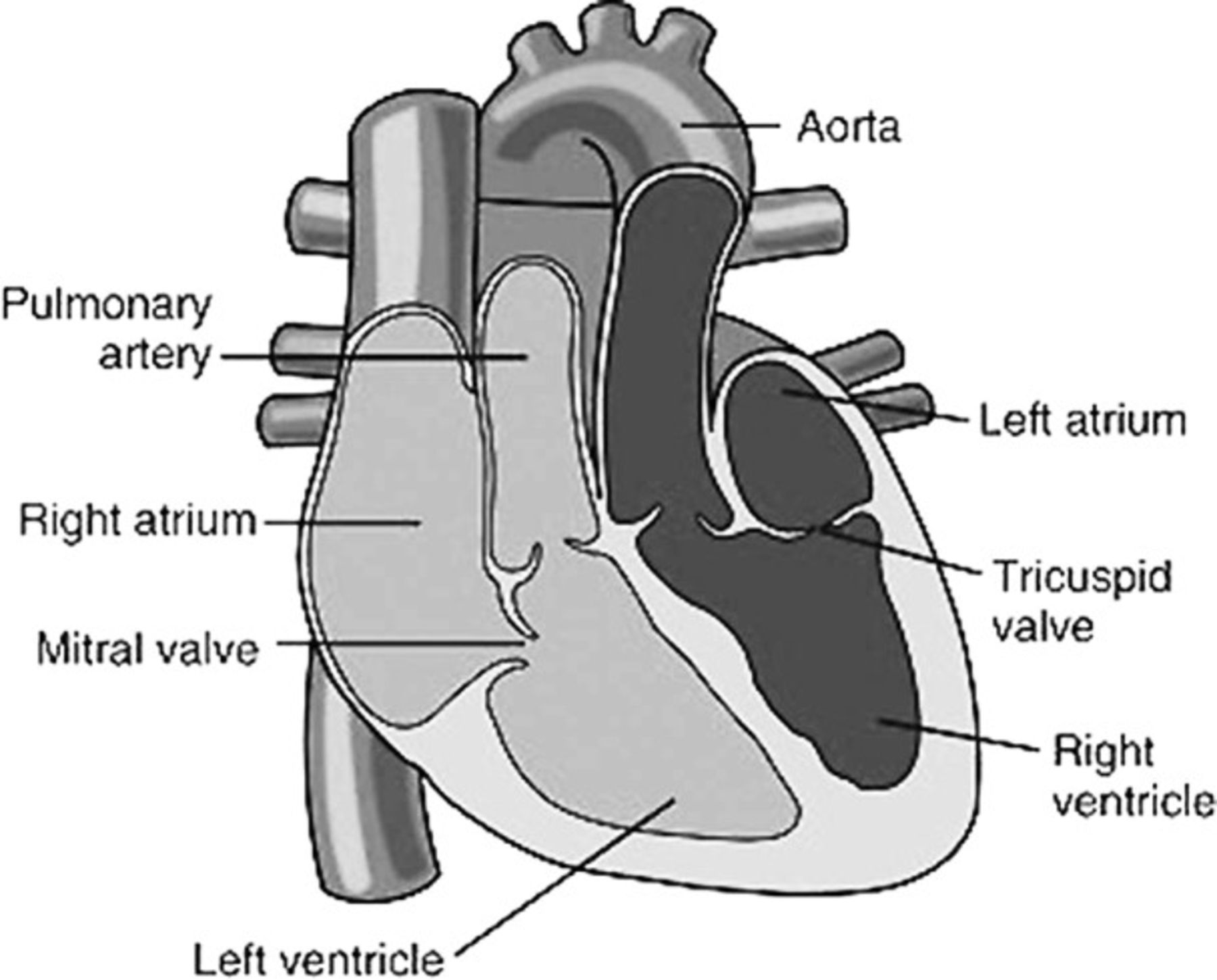
Levo-transposition of the great arteries (l-TGA) or congenitally corrected transposition of the great arteries has an incidence of 1:33,000 births.3 L-TGA is named after the characteristic left-sided loop made by the ventricles during embryologic development. In this anomaly, venous blood flow returns from the body into the right atrium, to a morphologic left ventricle, and into the pulmonary artery that bifurcates en route to the lungs. Freshly oxygenated blood returns via the pulmonary veins into the left atrium, through a systemic right ventricle, and then out the aorta into systemic circulation (Figure 1).4 Commonly, l-TGA is associated with other cardiac anomalies such as ventricular septal defects (70%), pulmonary stenosis (40%), tricuspid valve abnormalities (90%), and Ebstein anomaly.5 The complications of l-TGA include congestive heart failure, tricuspid regurgitation, and arrhythmias.

In levo-transposition of the great arteries, venous blood returns from the body into the right atrium, to a morphologic left ventricle, and into the pulmonary artery that bifurcates en route to the lungs. Freshly oxygenated blood returns via the pulmonary veins into the left atrium, through a systemic right ventricle, and then out the aorta into systemic circulation. Reproduced with permission from Elsevier.4
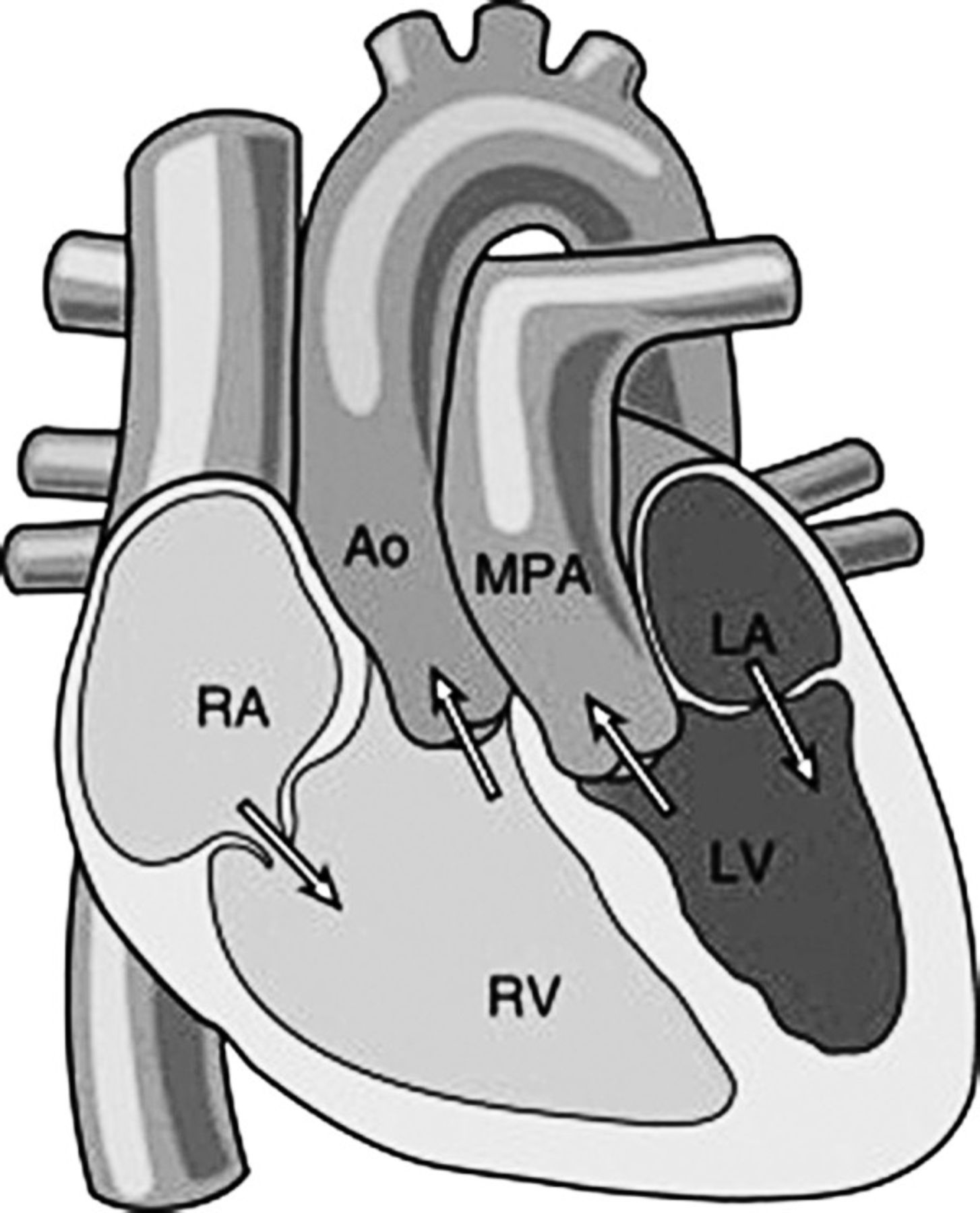
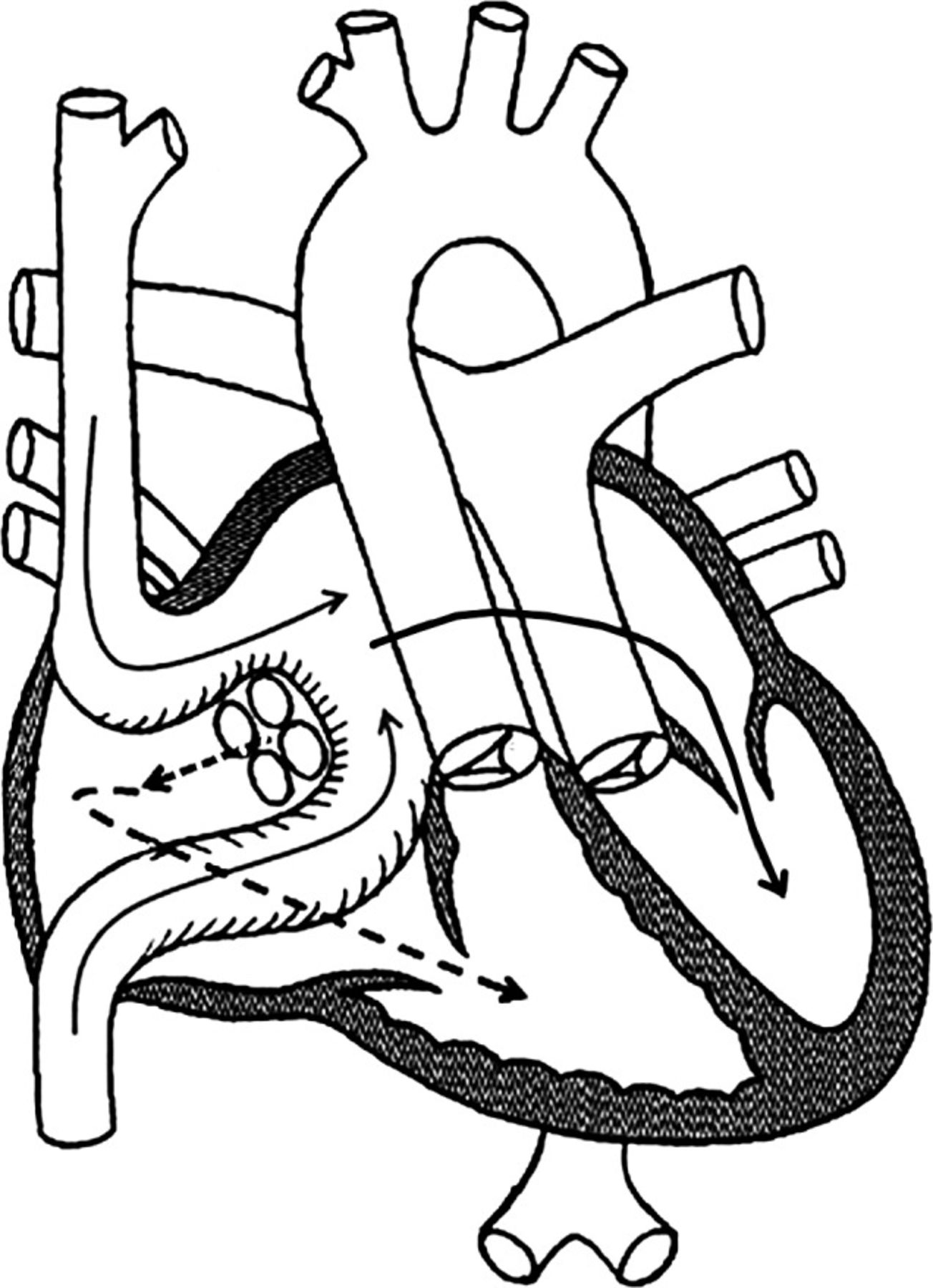
Dextro-transposition of the great arteries (d-TGA) or complete transposition of the great arteries has an incidence of 1:5,000 births.1 This condition is a dextro-cardiovenous loop in which venous blood returns through the right atrium to a right ventricle attached to an ascending aorta. In a parallel circuit, freshly oxygenated blood from the pulmonary veins enters the left atrium, drains into the left ventricle, and is then pumped back into the lungs by the main pulmonary artery (Figure 2).4 Patients with d-TGA commonly have associated septal defects or patent ductus arteriosus to allow for the combination of oxygenated and deoxygenated blood flow. If an infant is born without any lesions, an atrial septostomy is performed immediately with a Rashkind (balloon) or Blalock-Hanlon procedure (surgical correction) until the infant has time to develop and more definitive surgery can be performed. Until the 1980s, the Senning and Mustard procedures, commonly known as atrial baffles, were atrial switch surgical procedures that resulted in the exchange of blood between the right and left atria (Figure 3).6 However, long-term complications of these procedures include tricuspid regurgitation, pulmonary hypertension, systemic ventricular dysfunction, baffle leaks, superior vena cava stenosis, and various arrhythmias, including atrial node dysfunction and atrial flutter.7 From the late 1980s and early 1990s onward, d-TGA has been managed instead by arterial switch operations in which the ventriculoarterial discordance is rectified.1

In dextro-transposition of the great arteries, venous blood returns through the right atrium (RA), to a right ventricle (RV) attached to an ascending aorta (Ao). In a parallel circuit, freshly oxygenated blood from the pulmonary veins enters the left atrium (LA), drains into the left ventricle (LV), and is then pumped back into the lungs by the main pulmonary artery (MPA). Reproduced with permission from Elsevier.4

Atrial switch procedure (Mustard or Senning). Specialized channels (baffles) are made within the atrial chambers to divert deoxygenated blood from the body to the left ventricle and pulmonary artery (solid arrows) and to divert oxygenated blood to the right ventricle and aorta (dashed arrows). Reproduced with permission from Keck School of Medicine of University of Southern California CardioVascular Thoracic Institute.6
FAILURE OF THE SYSTEMIC RIGHT VENTRICLE
Patients with l-TGA and patients with d-TGA with atrial baffle have right ventricles working against systemic pressures. With time, the systemic right ventricle loses the ability to maintain cardiac output and becomes dysfunctional. Some theories for why the right ventricle is unable to compensate with higher volume and pressure of the systemic system are discussed below.
Anatomy
The structural difference between the left ventricle and right ventricle seems to be one reason for the right ventricle's inability to compensate. Using magnetic resonance imaging (MRI) and computed tomography (CT), Saremi described the differences between the two ventricles. The trabeculations in the right ventricle are coarse, thick, and located at the apex, while the left ventricle has trabeculations all along its thickened wall.8 Uniquely, the right ventricle has an infundibulum without significant trabeculations and a moderator band connecting the interventricular septum to the anterior papillary muscle. In comparison, the left ventricle has limited nontrabeculated area and two papillary muscles.
Through the use of spatial modulation of magnetization (a noninvasive magnetic resonance tagging technique), Fogel et al compared the regional wall motion and segmental strain (relation of myocardial distortion between systole and end diastole) in single right ventricles, systemic right ventricles, and normal systemic ventricles.9 They found marked differences in regional wall motion and strain in each of the comparison groups. More important, Fogel et al demonstrated that the presence of two ventricles, even if the right ventricle was systemic, improved contractility compared to single-ventricle physiology.
Another key anatomical difference between the right and left ventricles is the arrangement of cardiomyocytes in the ventricles. The cardiomyocytes in the right ventricle are arranged in a longitudinal pattern, while the cardiomyocytes in the left ventricle are predominantly circumferential with radial and longitudinal patterns.10 As a result, the right ventricle is morphologically ill equipped to deal with the chronic high-pressure load from systemic circulation.
Myocardial Fibrosis
A combination of arterial hypertension and elevated aldosterone levels has been associated with cardiac fibroblasts developing reactive myocardial fibrosis, and myocardial fibrosis has been associated with the development of left ventricular failure.11 Similar pathogenesis may be involved in a systemic right ventricle. An attempt to visualize the right ventricle of patients with d-TGA with atrial baffle using late gadolinium enhancement (LGE) on MRI found areas of abnormal myocardium representing myocardial fibrosis or edema. The extent of the LGE correlated with right ventricular failure and poor clinical outcomes such as reduced peak oxygen uptake,12 reduced right ventricular ejection fraction (EF), prolonged QRS on electrocardiogram, arrhythmias, and syncope.13
Myocardial Ischemia
With the increased right ventricular mass in systemic right ventricles, coronary flow reserve can be reduced without coronary obstruction; therefore, myocardial ischemia of the right ventricle may be another important factor in right ventricular dysfunction. A study comparing two groups of patients with l-TGA (one with associated lesions and one without) vs volunteers without structural heart disease showed on stress positron emission tomography that with adenosine, coronary reserve flow was decreased in patients with l-TGA compared to normal volunteers (195-201 mL/100 g/min and 309 mL/100 g/min, respectively, P<0.001).13 These numbers imply an altered vasoreactivity and changes in the microcirculation of the systemic right ventricle.
A study of 5 patients with l-TGA whose ages ranged from 3.5 to 34 years showed that 80% of the patients had reversible defects, and all of them had fixed defects shown by exercise sestamibi scans. The irreversible areas of fixed deficit demonstrated restricted wall motion and impaired ventricular contractility.13
Physiology
A cineangiography study evaluating right and left ventricles in children with l-TGA found that right (systemic) ventricular size was within the normal limits of expected parameters for children without heart problems. However, children who had significant systemic to pulmonary shunting (pulmonary-to-systemic flow ratio Qp:Qs >1.7) or tricuspid insufficiency had increased ventricular size and decreased EF.14 Patients with l-TGA can develop right ventricular systemic dysfunction for the reasons described above; however, patients with associated abnormalities may develop complications sooner. Consequently, the structural and muscular configuration of the systemic right ventricle predisposes it to tricuspid insufficiency. In a study of 40 patients with l-TGA, tricuspid regurgitation was an independent risk factor for death; 20-year survival with and without tricuspid regurgitation was 49% and 93%, respectively.13
ASSESSMENT OF RIGHT VENTRICULAR FUNCTION
As a consequence of right ventricle structural differences and exposure to systemic pressures and volumes, systolic dysfunction of the right ventricle is the most frequent and clinically relevant problem in patients with TGA.7 Rates of systemic ventricular dysfunction are higher with increasing age, presence of associated cardiac lesions, arrhythmias, pacemakers, and tricuspid valve surgery.13
Early detection of right ventricular dysfunction is crucial to prevent the late onset of congestive heart failure and valvular abnormalities. Van der Bom et al followed 88 patients with TGA for 4 years with echocardiography, electrocardiography, cardiopulmonary stress testing, and cardiac MRI, searching for information predictive of adverse clinical events.15 The study showed that patients with a right ventricular end-diastolic volume index >150 mL/m2 and peak exercise systolic blood pressure <180 mmHg were most likely to experience adverse clinical events: an annual event rate of 19% vs 0.9% in patients without these parameters.15
Two studies have been published evaluating longitudinal strain by echocardiography in the context of clinical events. Kalogeropoulous et al evaluated 64 adults (mean age, 29 years) with d-TGA with atrial baffle and noted that a right ventricular global strain ≥–10% had the strongest correlation with heart failure and ventricular tachycardia during a median of 2.4 years.16 Another study by Diller et al evaluated 129 adult patients (mean age, 35 years) with l-TGA (n=42) and d-TGA with atrial baffle (n=87) by echocardiography and cardiac MRI. Right ventricular longitudinal strain >–13% provided 72% sensitivity and 63% specificity for a clinical outcome of death, New York Heart Association (NYHA) Class III or greater, or arrhythmia.17 An interesting observation in the Diller et al study was the associated abnormal longitudinal strain of the subpulmonary left ventricle.
Echocardiography, cardiac MRI, CT, radionuclide angiography, and cardiopulmonary stress testing are imaging modalities used to evaluate right ventricular function. Each modality has its advantages and disadvantages, and a combination of resources tailored to each patient is ideal.
Echocardiography
Without radiation and at a relatively lower cost than cardiac MRI and CT, echocardiography allows visualization and quantification of atrial and ventricular chamber size, wall, and valvular lesions. Recordings from the apical 4-chamber view in end diastole provide the best estimates of right ventricular dimensions. The American Society of Echocardiography guidelines to assess right heart function in adults provide references for interpretation.18 Right ventricular dysfunction was correlated with a right ventricular index of myocardial performance >0.40 by pulsed Doppler and >0.55 by tissue Doppler, a tricuspid annular plane systolic excursion <16 mm, 2-dimensional fractional area change <35%, and tricuspid lateral annular systolic velocity <10 cm/s. Optimal evaluation of the right ventricle by echocardiography is limited by a poor imaging window and the expertise of sonographers and cardiologists.19 The assessment of the right ventricle in congenital heart disease is not standardized, but newer echocardiography techniques such as longitudinal strain hold promise as discussed above.
Cardiac Magnetic Resonance Imaging
Although the right ventricle is difficult to evaluate because of its complex shape, cardiac MRI is the gold standard of right ventricular assessment because of its ability to completely visualize the right ventricle.19 Orwat et al state in their review of imaging in congenital heart disease of adults that cardiac MRI is not only used to quantify the size and function of the right ventricle but also to identify associated structural abnormalities and areas of concern after surgery, such as aortic root, branches of pulmonary arteries, and right ventricular outflow tract.19 Dobutamine stress MRI has been used to identify right ventricular dysfunction in asymptomatic or slightly symptomatic surgically corrected d-TGA cases.20 Impaired filling and lack of change in stroke volume with stress characterize right ventricular dysfunction. Importantly, no contrast agent is necessary to evaluate right ventricular function with or without stress. However, unlike echocardiography, cardiac MRI cannot be used in patients with pacemakers/implantable cardioverter defibrillators, the inability to cooperate with breath holding, or claustrophobia. In addition, cardiac MRI has limited availability and should be performed at a dedicated adult congenital heart disease center.
Computed Tomography
In patients who may have contraindications to cardiac MRI, CT can be used to assess right ventricular size and function by using retrospective gating to image the myocardium. Quantification of the ventricle size is possible by tracing the ventricle with the area-length method.21 Although techniques to lower radiation dose have evolved, adults with congenital heart disease often need repetitive imaging that risks exposing them to ionizing radiation.19
Radionuclide Angiography
Radionuclide angiography or multigated acquisition scan is another option for visualizing the right ventricle; however, it also comes with the added risk of radiation with decreased spatial and temporal resolution.22 Radionuclide angiography was introduced in the 1970s and was the first modality used to quantify ventricular function. It has been mostly replaced by echocardiography and cardiac MRI.
Cardiopulmonary Stress Testing
Cardiopulmonary stress testing is useful in adults with congenital heart disease because it measures peak oxygen consumption (VO2), allowing for the prognostication of right ventricular dysfunction. Stress testing is a key determinant of exercise capacity.23
TREATMENT OF RIGHT VENTRICULAR FAILURE
Winter et al established that uncertainty exists about the best practices for managing systemic right ventricular failure because of the lack of convincing data on managing systemic right ventricle dysfunction and the inability to apply left ventricular failure management principles to right ventricular failure.13
Medical Management
Beta-adrenergic receptor blockers (beta blockers) decrease left ventricle systolic dysfunction, increase EF, and improve NYHA class, improving morbidity and mortality. These beneficial effects led researchers to propose beta blocker use for right ventricular dysfunction,24 and multiple studies have shown that beta blockers are beneficial for treating right ventricular dysfunction. A study evaluated patients with systemic right ventricles for a mean of 12.8 months.24 Radionuclide angiography was used to measure EFs at baseline and after administering bisoprolol 10 mg a day or carvedilol 12.5 mg twice a day. The study reported a median increase in EF from 41%-49% in both groups.24 In a study by Doughan et al of 60 patients with d-TGA with atrial baffle who were taking beta blockers, 73% of patients increased one to two NYHA functional classes. The average dose of carvedilol and metoprolol succinate was 24 mg/day and 47 mg/day, respectively, and no differences were seen between the two beta blockers in study endpoints. The patients not treated with beta blockers had higher right ventricular end-diastolic area at the 4-month follow-up, implying reduced myocardial remodeling in that group.25 Patients on beta blocker therapy require close monitoring because these patients can develop atrioventricular nodal block and sinus node dysfunction. Interestingly, Doughan et al correlated that only patients with pacemakers had improvement in functional class; patients with pacemakers received higher doses of beta blocker therapy than patients without pacemakers (mean maintenance dose of carvedilol, 28 ± 17 mg vs 12 ± 6 mg, respectively, P<0.05).25
Angiotensin-converting enzyme inhibitors and angiotensin receptor blockers have a valid role in reducing mortality in left ventricle failure and aldosterone-induced myocardial fibrosis, but evidence for their use in the morphologic right ventricle is inconclusive.13 One study showed that administration of enalapril 0.5 mg/kg/day (maximum dose, 20 mg twice a day) for 12 months did not affect total exercise time, functional capacity, VO2 (peak/rest), stroke volume, and cardiac index. These results were based on a multitude of measurements taken on a bicycle ergometer during the exercise test at baseline, 1 month, 6 months, and 12 months, using echocardiograms, peak VO2 using mass spectrometer, resting cardiac index, tidal volume, height, weight, and respiratory rate.26 A multicenter randomized control crossover trial of 29 adult patients with systemic right ventricles (mean age, 30 ± 10.9 years; 21 with d-TGA with atrial baffle and 8 with l-TGA) showed no significant differences in VO2 max, exercise duration, and N-terminal pro-B-type natriuretic peptide levels in patients when they were taking losartan compared to when they were taking placebo. The lack of effect in this study was postulated to be secondary to the lack of an increase in the neurohormonal levels in this population.27 However, a small study of 7 patients showed improvement in systolic function on echocardiography in EF and exercise time after limited administration of losartan for 8 weeks.13 Perhaps the improvement in right ventricular function and exercise capacity is significant in symptomatic patients with elevated neurohormonal levels.
Digoxin has been used to treat heart failure since the 1700s, but heart failure guidelines do not support the routine use of digoxin for patients with left ventricular dysfunction.28 In only one study, digoxin increased cardiac output by approximately 10% and decreased norepinephrine levels in patients with right ventricular dysfunction with pulmonary hypertension.29 No published studies exist on the use of digoxin in patients with right systemic ventricles.
Diuretics are essential for symptomatic treatment of patients with left ventricular failure. In theory, diuretics reduce afterload of the heart, enhancing contractility and reducing end-systolic volume. Whether they also improve functionality in the systemic right ventricle is yet to be answered. Empirical use of diuretics to alleviate right ventricular failure–related symptoms is common and harmless, eliminating the need for randomized trials.13
Aldosterone antagonists, such as spironolactone and eplerenone, are effective for treating left ventricular failure. The EVEDES (Eplerenone in Systemic Right Ventricle) study randomized 26 patients with d-TGA with atrial baffle to eplerenone or placebo. The patients underwent complete physical examination, cardiac MRI, and laboratory testing including neurohormones and collagen biomarkers. At one year, no significant change in symptoms, complete physical examination, or cardiac MRI findings showed a benefit of treatment; however, collagen turnover biomarkers improved in the eplerenone treatment group.30
Surgical and Procedural Management
Patients with congenital heart disease are at risk of atrial and ventricular arrhythmias. These arrhythmias can be secondary to the specific congenital anomaly or a consequence of surgical correction. Although prevalence varies by anomaly, atrial arrhythmias are estimated to be present in >30% of patients with congenital heart disease.31 After atrial switch procedures in patients with d-TGA, intraarterial reentrant tachycardia and atrial flutter commonly occur.31 Risk factors that worsen the prognosis of untreated arrhythmias include age, prolonged duration of follow-up with a cardiologist, and worsening degree of right ventricular dysfunction in l-TGA.32
Pacemakers can be considered for patients with symptomatic bradycardia or atrioventricular block who exhibit fatigue, dizziness, syncope, or dyspnea on exertion secondary to chronotropic incompetence. Sinus node dysfunction is common in d-TGA with atrial baffle, and atrioventricular block is common in l-TGA.33
Cardiac resynchronization therapy (CRT) is another method that can improve symptoms of arrhythmias. Currently, Class I indications are based on left ventricular failure: ventricular dysfunction with left ventricular EF <35%, left bundle branch block with QRS interval >150 ms, and NYHA Class II-IV.34 The precise indications for CRT use in congenital heart disease are undefined; however, retrospective trials analyzing patients with l-TGA and d-TGA with systemic right ventricles who received CRT for atrial and ventricular arrhythmias show promising results. An improved EF (13.3% ± 11.3%) by echocardiography or radionuclide angiography and a decreased QRS duration (38.2 ± 29.4 ms, P<0.05) were noted in 17 patients during a median follow-up of 4 months. Additionally, 13 of these patients had clinical improvement.35 Deciding on whether to use CRT is complex: patients underreport their symptoms, and assessment of right ventricular function is challenging using echocardiography alone as is the placement of coronary sinus leads.5 As clinicians, when a patient with TGA needs a pacemaker, we must consider and discuss the potential benefit of CRT.
Systemic tricuspid regurgitation progressively worsens the symptoms of heart failure in patients with TGA. The severity of the valve leak can be determined using parameters to quantify flow through the atrioventricular valve during systole. While mild tricuspid regurgitation may be tolerated, severe refractory tricuspid regurgitation requires surgical correction. Although rarely well tolerated in adulthood, one surgical option is the double switch (arterial plus atrial) procedure, an anatomic correction for possible reduction of severe tricuspid regurgitation. Occasionally, patients with severe tricuspid regurgitation and l-TGA may undergo partial pulmonary artery banding that results in a shift of the ventricular septum toward the systemic right ventricle and a reduction in tricuspid valve regurgitation.5 Tricuspid valve replacement is a reasonable option and has been shown to improve 10-year survival while preserving right ventricular EF. Forty-six patients with right ventricular EF >45% (n=17) were compared to another group of patients with right ventricular EF <45% (n=29) prior to undergoing atrioventricular valve replacement in l-TGA. Overall postoperative survival at 5 years and 10 years was 100% and 94% in group 1 (EF >45%) vs 92% and 55% in group 2 (EF <45%).36 Other variables associated with late mortality after valve replacement include subpulmonary ventricular systolic pressures >50 mmHg, presence of atrial fibrillation, and NYHA Class III-IV.37
Advanced treatment options may be necessary for patients with TGA with systemic right ventricle and symptoms not amenable to medications, pacemaker, CRT, and surgical correction. An Impella device (Abiomed) may be used to provide right ventricular support, and implantations of ventricular assist devices (biventricular assist devices and right ventricular assist devices) have been successful in patients with TGA, especially as a bridge to heart transplantation.38 Orthotopic heart transplantation may be an option if pulmonary artery pressures are not elevated and surgical anatomy is amenable. In a review of heart transplantation for congenital heart disease, 22% of transplants were performed to treat TGA, and the a 5-year survival rate was 69%.39
CONCLUSION
More adults than children live with congenital heart disease, and a significant number of these patients have TGA and systemic ventricles. With a paucity of research and guidelines built on expert opinion, it is important to understand the anatomy, associated anomalies, and surgical corrections of TGA and systemic ventricles. With this understanding, we become more knowledgeable about the complications, most appropriate diagnostic tests, and treatment options of TGA and systemic ventricles. Today, we are primarily treating right heart failure and arrhythmias in TGA. Our noninvasive imaging options for the assessment of right ventricles include echocardiography with novel strain methods and cardiac MRI. We should also use cardiopulmonary stress testing to help determine the true severity of symptoms. From a medication standpoint, beta blockers titrated to maximum dose have the most supportive data, and diuretics are used mostly for symptoms. In this complex population, when symptoms persist, a team of multidisciplinary specialists can evaluate the appropriateness of pacemaker, heart failure, and surgical treatment options. A personalized, multidisciplinary plan is the future of congenital heart failure management.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care, Medical Knowledge, and Systems-Based Practice.
ACKNOWLEDGMENTS
The authors have no financial or proprietary interest in the subject matter of this article.
- © Academic Division of Ochsner Clinic Foundation
REFERENCES
In this issue








{kind=link}
{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.