
INTRODUCTION
Moyamoya is a unique, chronic, progressive cerebrovascular condition that predominantly involves the intracranial internal carotid arteries and the anterior circle of Willis and is characterized by compensatory collateralization of small vessels. The characteristic angiographic appearance of these small collateral vessels leads to the name moyamoya that roughly translates from Japanese to “puff of smoke.” Moyamoya can refer either to a distinct cerebrovascular disease (moyamoya disease) or to a syndrome related to chronic and genetic diseases (moyamoya syndrome).1 We present the case of a patient with intracranial internal carotid artery stenosis and robust collaterals consistent with moyamoya syndrome.
HISTORY
A 53-year-old male with Down syndrome presented to an outside emergency department for evaluation after an all-terrain vehicle accident. At the time of presentation, the patient was at his baseline mental status, and no new focal neurologic deficits were noted. Workup was significant for traumatic subarachnoid hemorrhage visible on computed tomography (CT), and the patient was transferred to our center for further evaluation.
RADIOGRAPHIC APPEARANCE AND TREATMENT
Cranial CT demonstrated diffuse scattered subarachnoid hemorrhage and multiple remote infarcts in a watershed distribution involving the bilateral frontal lobes and the left parietal lobe. CT angiography showed severe stenosis of the bilateral proximal middle and anterior cerebral arteries with the suggestion of multiple deep lenticulostriate collaterals.
These findings were concerning for moyamoya syndrome, and the patient underwent cerebral angiography for further evaluation. Digital subtraction angiography (DSA) was performed via the right common femoral artery. The right internal carotid artery arteriogram demonstrated occlusion of the right internal carotid artery distal to the ophthalmic artery with prominent lenticulostriate and leptomeningeal collaterals to the right middle cerebral artery territory (Figure 1). A large right posterior communicating artery provided collateral flow to the right middle cerebral artery territory through the posterior cerebral artery collaterals. Selective right external carotid artery injection showed an enlarged right middle meningeal artery with collaterals to the bilateral anterior cerebral artery territories (Figure 2). The left vertebral artery injection showed collateral filling of the posterior aspects of the left middle cerebral artery via posterior cerebral artery collaterals. Left internal carotid artery arteriogram demonstrated high-grade stenosis of the left internal carotid artery distal to the ophthalmic artery with prominent lenticulostriate collaterals. The left ophthalmic artery was enlarged and provided collateral flow to the left anterior cerebral artery (Figure 3). The left external carotid artery showed an enlarged left middle meningeal artery with collateral flow to the left anterior cerebral artery. The patient was admitted to the neurocritical unit for close monitoring of neurologic status. No surgical intervention was undertaken because his neurologic status remained stable. The patient was discharged with vascular neurology and neurosurgery follow-up for further management.

Right internal carotid artery injection shows distal interior carotid artery occlusion with prominent lenticulostriate and leptomeningeal collaterals (white arrow) consistent with the characteristic “puff of smoke” appearance of moyamoya. Also shown are distal pericallosal (anterior cerebral artery) branches and distal middle cerebral artery branches (thick black arrows) filling via the enlarged posterior communicating artery (thin black arrow).
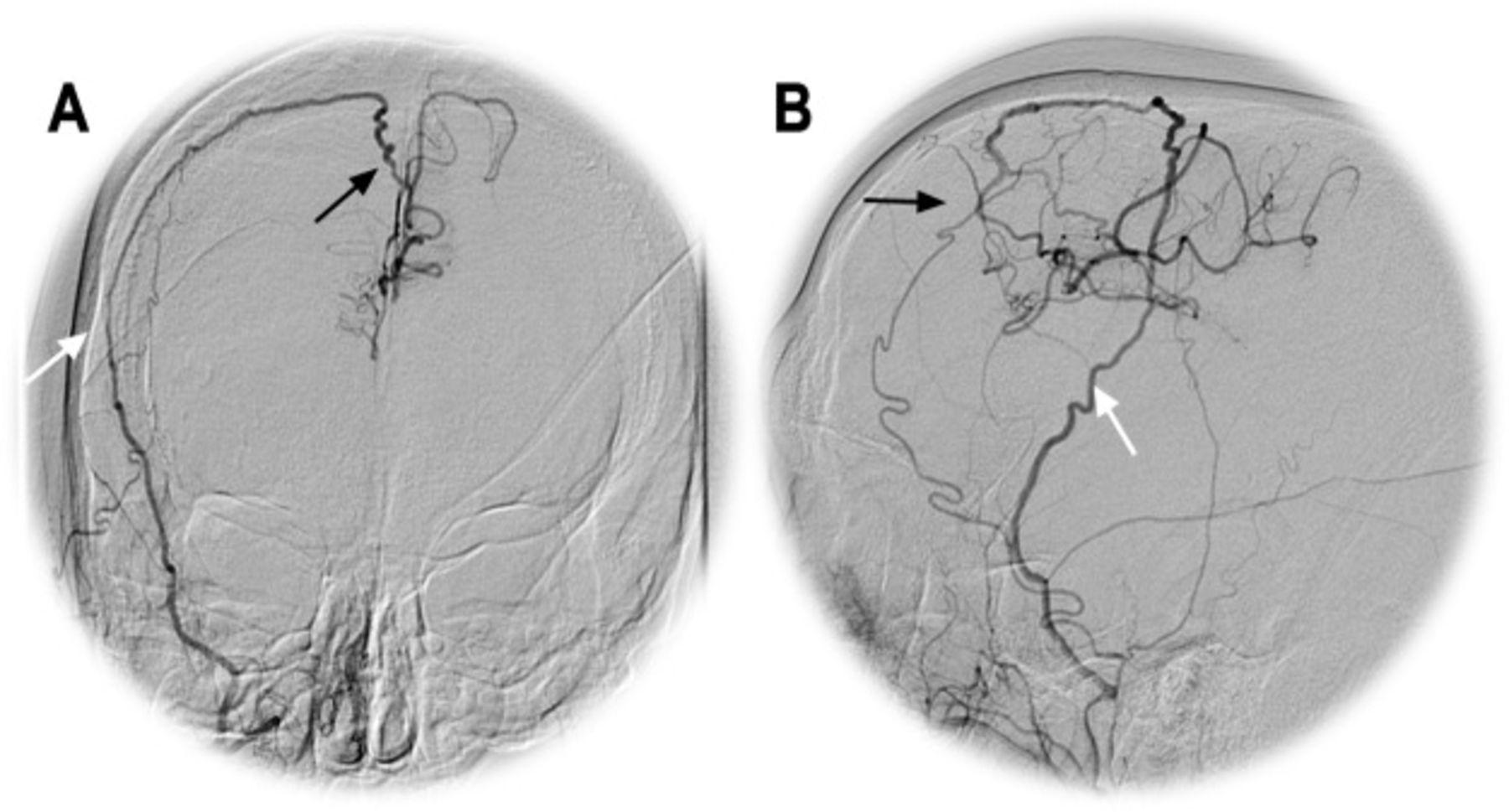
Right external carotid injection in (A) anteroposterior film and (B) lateral film. In both images, an enlarged middle meningeal artery (white arrows) can be observed crossing the midline and providing extracranial-to-intracranial collaterals to bilateral anterior cerebral artery territories (black arrows).

Left internal carotid injection shows high-grade interior carotid artery stenosis and A1 and M1 occlusion with lenticulostriate collaterals (white arrow) consistent with moyamoya. Additionally, an enlarged ophthalmic artery provides collaterals to the anterior frontal branches of the anterior cerebral artery (black arrow).
DISCUSSION
Moyamoya was first described in 1957 in Japan. Moyamoya disease predominantly affects people of East Asian descent but has been described in populations across the globe. The disease has a bimodal distribution with peaks occurring in children of approximately 5 years of age and in adults in their mid-40s. The disease is nearly twice as common in females. In Japan, moyamoya disease has a prevalence of 3 cases for every 100,000 children, a reported incidence that is 10 times greater than in European populations.2
The most common presenting symptoms in moyamoya syndrome are ischemic stroke and transient ischemic attacks (50%-75% of cases) and intracerebral hemorrhage (10%-40%), with hemorrhage being the more common presenting symptom in adults.3 Less commonly, patients present with seizures and headache and rarely with choreiform movements or psychiatric changes. As mentioned above, moyamoya disease presents as an isolated phenomenon with specific angiographic findings but without other systemic illnesses. Fifty percent to 75% of cases present as isolated moyamoya disease, most commonly among people of East Asian descent.3
When moyamoya disease presents in the setting of chronic and genetic diseases, it is referred to as moyamoya syndrome. The most common associations are with sickle cell disease, neurofibromatosis type 1, cranial radiation, and Down syndrome. Less common associations include congenital cardiac and vascular anomalies and congenital tumors, although multiple other infectious, genetic, hematologic, and metabolic disorders have been associated with moyamoya syndrome.3
Despite the increasing usage of noninvasive imaging,4 DSA remains the gold standard of diagnosis. CT may show areas of cortical watershed infarcts in patients with moyamoya syndrome, as in the case of our patient, and CT angiography can reveal proximal intracranial stenosis. Magnetic resonance imaging/magnetic resonance angiography can detect acute infarcts using diffusion-weighted imaging. Because of diminished cortical blood flow, fluid attenuation inversion recovery sequences may show linear areas of high signal intensity in a sulcal pattern known as the ivy sign.5 CT and magnetic resonance perfusion imaging are promising noninvasive methods to estimate regional cerebral blood flow and monitor the effects of treatment.
The treatment of moyamoya in the acute setting is focused on preventing complications of cerebral ischemia.3 To date, no acute therapy has been shown to improve outcomes in patients with moyamoya disease. Thrombolytic and antithrombotic therapies have been avoided because of concern for hemorrhagic conversion in areas of collateralization.6 Aspirin is currently recommended in the acute setting of moyamoya.7 The mainstay of current therapy in moyamoya is surgical revascularization for secondary prevention;3 however, no prospective, randomized clinical trials have been performed that compare medical therapy to surgical revascularization. Direct and indirect techniques exist for surgical revascularization. Direct revascularization involves anastomosis of a cortical middle cerebral artery branch with, most commonly, the superficial temporal or middle meningeal artery. Indirect techniques vary and include laying the superficial temporal artery or layer of muscle, dura mater, or galea aponeurotica (in various combinations) directly onto the pial surface. In a large retrospective survey from Japan, no statistical difference was observed in outcomes between medically and surgically managed patients.8 However, in a large survey of moyamoya disease in childhood, 38% of medically managed patients developed progressive symptoms and required surgery.9 A 2006 North American study found that medically treated adult patients had a 65% risk of recurrent ipsilateral stroke vs a 17% risk of stroke or death in surgically treated patients.10 In a 2005 systematic review, 87% of pediatric patients undergoing surgical revascularization received a symptomatic benefit from surgery, with a reported perioperative stroke rate of 4%.11 Surgery has also been shown to reduce rates of cerebral hemorrhage in the Japan Adult Moyamoya (JAM) Trial published in 2014,12 although the effects on functional outcome are uncertain.13
The natural history of moyamoya disease is variable but usually progressive, and progression may be slow or fulminant. In both the slow and fulminant disease courses, two-thirds of patients with moyamoya disease who are not treated are estimated to have symptomatic progression within 5 years.3
- © Academic Division of Ochsner Clinic Foundation
REFERENCES
In this issue








{kind=link}
{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.