
Abstract
Background Broad indications for the use of statin medications are resulting in more patients using these therapies. Simultaneously, healthcare professionals are strongly advocating recommendations to increase exercise training (ET) as a means of decreasing cardiovascular disease (CVD) risk and improving other parameters of fitness.
Methods We review the literature to explore mechanisms that may increase the risk of statin/ET interactions, examine the benefits and risks of combining ET and statin use, and offer strategies to minimize the hazards of this combination therapy.
Results The combined use of statins and ET can result in health gains and decreased CVD risk; however, multiple factors may increase the risk of adverse events. Some of the events that have been reported with the combination of statins and ET include decreased athletic performance, muscle injury, myalgia, joint problems, decreased muscle strength, and fatigue. The type of statin, the dose, drug interactions, genetic variants, coenzyme Q10 deficiency, vitamin D deficiency, and underlying muscle diseases are among the factors that may predispose patients to intolerance of this combined therapy.
Conclusion Effective strategies exist to help patients who may be intolerant of combined statin therapy and ET so they may benefit from this proven therapy. Careful attention to identifying high-risk groups and strategies to prevent or treat side effects that may occur should be employed.
INTRODUCTION
Physical activity reduces the risk of cardiovascular disease (CVD), both directly and by reducing other risk factors such as unhealthy lipid profiles, blood pressure, insulin resistance, and obesity.1-4 Statins further reduce the risk of CVD events and all-cause mortality,5 principally by lowering levels of low-density lipoprotein (LDL) cholesterol. Although statins are well tolerated, they can affect skeletal muscle, producing symptoms that range from myalgia to creatine kinase (CK) elevations and rhabdomyolysis. These statin-associated musculoskeletal side effects can be exacerbated by physical activity.6-8 Statin use is becoming more widespread as indications broaden for CVD risk reduction. Simultaneously, physical activity is increasingly recognized and recommended to reduce CVD risk.9 Statin-associated musculoskeletal side effects, exacerbated by recommended physical activity, could lead to reduced statin use in individuals who would benefit from statin therapy. This review explores mechanisms that may increase the risk of statin/exercise training (ET) interactions, examines the risks and benefits of combining physical activity and statin use, and offers strategies to minimize the hazards of this combination therapy.
DEMOGRAPHICS
Approximately 11% of the US population uses lipid-lowering drugs as treatment for hyperlipidemia, and 44.5% of Americans >65 years use such medications. Statin use has increased progressively in all age groups since 1988 because these agents are the most effective lipid-lowering medications, and the 2013 American Heart Association/American College of Cardiology guidelines have broadened the indications for their use.10 Simultaneously, the percentage of American adults engaging in physical activity has also progressively increased. In 1998, only 14.3% of adults met the Physical Activity Guidelines for adults established in 2008,11 whereas in 2010, 20.7% of American adults engaged in sufficient aerobic ET and strength training to meet these guidelines. The convergence of these 2 trends increases the possibility of unfavorable side effects from the interactions of these 2 therapies. Current estimates are that 7%-29% of statin users develop statin-associated musculoskeletal side effects.12
PHARMACOLOGY
Statins or 3-hydroxy-3-methylglutaryl (HMG) coenzyme A reductase inhibitors inhibit the conversion of HMG coenzyme A to mevalonic acid by blocking the HMG coenzyme A reductase receptor. Access of the HMG coenzyme A substrate is thus prevented because of the presence of the statin in the binding pocket of the enzyme,13 ultimately inhibiting both mevalonic acid and cholesterol synthesis (Figure). Mevalonic acid is also a precursor for ubiquinone (coenzyme Q10 [CoQ10]) production. Thus, inhibition of mevalonic acid production also results in lower CoQ10 levels as well as a reduction in dolichols and isoprenylated proteins that are involved in cellular respiration and muscle cell functioning.14-16
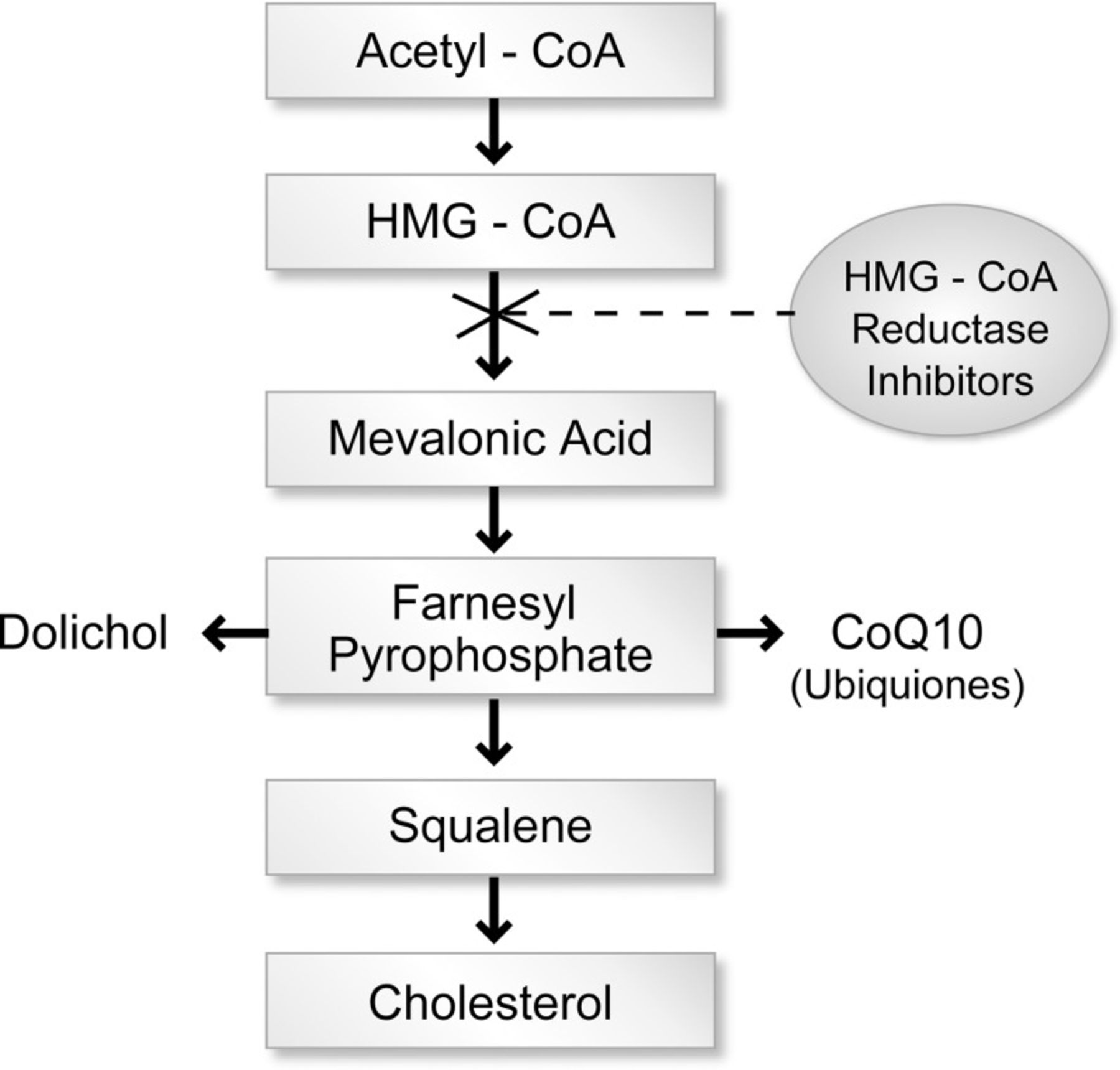
Pharmacology of statin metabolism.
Co, coenzyme; HMG, 3-hydroxy-3-methylglutaryl.
The half-life of most statins is 1-3 hours. Atorvastatin and rosuvastatin, however, have half-lives of 15-30 and 19 hours, respectively. Pravastatin and rosuvastatin are hydrophilic statins. Lovastatin, atorvastatin, fluvastatin, pitavastatin, and simvastatin are lipophilic.17-19
Pravastatin is the only statin that has no significant metabolism by the hepatic cytochrome P-450 (CYP) system; 20% of the absorbed dose is excreted renally. In the intestine and the liver, the CYP system is responsible for the metabolism of the other statins. Lovastatin, simvastatin, and atorvastatin are metabolized by the CYP3A4 isoenzyme. Fluvastatin and pitavastatin are metabolized by the CYP2C9 isoenzyme.18,19 Medications or substances that inhibit or bind to the CYP3A4 or CYP2C9 isoenzymes can increase the levels of those specific statins.17
Enzymatic inhibitors of CYP3A4 include azole antifungals (itraconazole, ketoconazole, fluconazole), macrolide antibacterials (erythromycin, clarithromycin), calcium channel blockers (diltiazem, verapamil), and tropical juices such as grapefruit juice. Grapefruit juice, pomegranate juice, and starfruit contain an inhibitor of the intestinal CYP3A4 isoenzyme that decreases intestinal catabolism and thereby enhances statin absorption.20,21 Human immunodeficiency virus protease inhibitors (ritonavir, nelfinavir, indinavir) are also recognized CYP3A4 inhibitors. Cyclosporine inhibits both intestinal and hepatic CYP3A4 activity and can therefore lead to increased bioavailability of statins metabolized by CYP3A4. Azole antifungal agents are recognized inhibitors of CYP2C9 as well as CYP3A4. Coadministration of itraconazole, ketoconazole, or fluconazole with fluvastatin or pitavastatin may increase the risk for statin toxicity. Patients with genetic variations in CYP enzyme activity may be at increased risk for statin-associated musculoskeletal side effects.22,23
Pharmacologic effects resulting in decreased serum statin levels occur when these CYP isoenzymes are induced. Drugs that may induce CYP may also decrease the effectiveness of statins by increasing their clearance. Such drugs include carbamazepine, dexamethasone, fosphenytoin, phenobarbital, phenytoin, primidone, rifampin, and St. John's wort. CYP2C9 is also induced by rifampin and increases the clearance of fluvastatin. Interestingly, omeprazole appears to possess a CYP3A4-inducing capacity that potentially increases biotransformation and, thus, decreases the levels of statins that are substrates of the CYP3A4 isoenzyme.18
MECHANISMS OF STATIN-ASSOCIATED MYOPATHY
The 2014 Statin Muscle Safety Task Force defined myalgia as muscle discomfort resulting in a sensation of pain, soreness, cramping, spasm, or achiness with or without an elevation in CK levels. Myopathy refers to muscle weakness with or without CK elevations.24 Muscle inflammation associated with elevated CK levels characterizes myositis. Myonecrosis refers to muscle injury and is graded by the degree of CK elevation. Severe myonecrosis associated with myoglobinuria or acute renal failure indicates clinical rhabdomyolysis.24
A variety of mechanisms may contribute to statin-associated myopathy. Reductions in myocyte cholesterol levels could reduce cholesterol required for sarcolemmal, endoplasmic reticular, or T-tubule membrane stability. Indeed, one study reported defects in T-tubule structure in asymptomatic patients who took statins.25 CoQ10 is a mitochondrial transport protein required for normal mitochondrial respiration. Statins inhibit CoQ10 production, and circulating CoQ10 levels decrease during statin therapy. This decrease has been attributed to statin-induced reductions in LDLs, including LDL and very-low-density lipoprotein (VLDL), that transport CoQ10, but ezetimibe therapy does not reduce CoQ10 levels despite reductions in LDL concentrations.26 However, according to a metaanalysis of 6 CoQ10 supplement studies and a careful study of CoQ10 supplementation in subjects with statin-associated myalgia confirmed by a blinded run-in protocol, CoQ10 supplementation has not been shown to reduce statin-associated myalgia.27,28 Other possible mechanisms of statin-associated myopathy include a reduction in GTP-binding proteins such as Ras, ROCK, and Rho that are needed for cell maintenance; alterations in fat metabolism either as a primary effect or via changes in mitochondrial function; or failure to repair damaged skeletal muscle because of reductions in atrogin-1 activity, vitamin D deficiency, and inflammation.29-33 Meador and Huey reviewed the combination of statin-associated myopathy and physical activity, postulating that mechanisms for this myopathy could include induction of skeletal muscle fiber apoptosis, alterations in ubiquitin-proteasome pathway activity, mitochondrial dysfunction, and terpenoid depletion.34
AT-RISK POPULATIONS
Populations at risk of musculoskeletal side effects from combined ET and statin therapy are the elderly, certain racial groups and genotypes, patients with mitochondrial diseases, and patients with underlying muscle diseases. Vitamin D deficiency is widespread and may also predispose individuals to excess risk.
The elderly appear to be at greater risk than the general population for statin-associated myopathies that can occur in up to 11% of patients in the geriatric population.35,18 Statins are commonly indicated medications for the elderly, given the high incidence of medical conditions such as diabetes mellitus, cerebrovascular disease, and CVD in this population.
Aging has a number of effects on muscular and cardiac activity, including an associated steady decline in the absolute heart rate that can translate into a decrease in cardiac output. Aging is also associated with a gradual decline in maximal oxygen consumption (VO2 max). Additionally, the elderly experience a steady decrease in the size and number of fast-twitch muscle fibers (type 2 fibers) with a relative increase in the proportion of slow-twitch muscle fibers (type 1 fibers).36
Patients of Asian race tend to have high levels of statins for a given dose of medication.18 Genetic differences involving the CYP enzymes may be responsible for these high serum levels. Indeed, rosuvastatin is labeled for lower doses in patients of Asian race.18 Patients in this population are at risk of experiencing side effects from rosuvastatin and achieve therapeutic LDL cholesterol reductions from lower doses of this drug.37 In Japan, statins are approved for use at lower doses than the doses approved in the United States.38
Myopathies related to abnormal genotypes also predispose individuals to statin-associated worsening of symptoms. Of 110 patients with primarily statin-associated myopathies, 11 (10%) had at least one abnormal allele for a gene affecting muscle metabolism.39 These patients may have had especially severe myopathy because many were willing to undergo skeletal muscle biopsy. Only 3% of asymptomatic patients on therapy tested positive for the abnormal alleles. The various genes involved those coding for carnitine palmitoyltransferase II deficiency, McArdle disease, and myoadenylate deaminase deficiency.
In another study, a genomewide scan conducted in 85 subjects with statin-associated myopathy yielded a single strong association of myopathy with the rs4363657 single-nucleotide polymorphism located within SLCO1B1.2 The prevalence of the variant in this population was 15%. SLCO1B1 encodes the organic anion transporting polypeptide OATP1B1, thereby regulating the hepatic uptake of statins. The majority of myopathies associated with 80 mg simvastatin were attributed to the 521C variant of SLCO1B1.2,40 Additional studies have shown that other polymorphisms of the SLCO1B1 gene result in elevated statin levels.41,42 The theory is that reduced hepatic uptake of statins in individuals with an abnormality in SLCO1B1 allows higher statin levels in the periphery, including skeletal muscle.
Because CoQ10 is required for mitochondrial adenosine triphosphate (ATP) generation, mitochondrial diseases associated with decreased CoQ10 production result in substantial risk from statin therapy. Genetic processes that interfere with CoQ10 production increase the risk for statin-associated myopathy. Genes coding for CoQ10 include COQ2, COQ4, PDSS1, and PDSS2. Defects in these genes are associated with severe infantile syndromes characterized by significant myopathies, dysmorphic features, ataxia, and mental retardation.43-45 Three genes in particular were implicated in 2011 as markers for statin-associated myalgia: COQ2, which participates in the biosynthesis of CoQ10; ATP2B1, which encodes a calcium-transporting ATPase involved in calcium homeostasis; and DMPK, which encodes a protein kinase implicated in myotonic dystrophy.46
Vitamin D deficiency has been identified as a risk factor for statin-associated myopathy.47 Biologically plausible mechanisms have been suggested. Low levels of vitamin D may shunt the action of CYP3A4 from metabolizing statin medication toward 25-hydroxylation for the production of active vitamin D, resulting in toxic levels of the statin.48 Lack of vitamin D may also alter gene transcription, preventing translation of proteins that repair muscle tissue structures and leading to a synergistic effect in statin-treated patients.29
Underlying muscle diseases also predispose affected patients to statin-associated myopathies. Some of the muscle diseases that may be aggravated or revealed by statin use are myasthenia gravis,49,50 McArdle disease,51 amyotrophic lateral sclerosis,52 myotonic dystrophy, muscular dystrophy, and motor neuropathies. Other populations at risk are patients with small body frame, alcoholism, and liver or renal dysfunction.18
STATIN/ET INTERACTION RISKS
When ET and statin medications are combined, patients are at risk for specific side effects. Muscle-related problems, decreased athletic performance, musculoskeletal derangements, and fatigue are among the most common problems. Symptoms of myopathy most commonly occur in proximal muscles, and symptoms such as muscle cramps most commonly occur at night.53 Rhabdomyolysis occurred in <0.01% of patients in a study of 30 clinical trials.35 Fatal rhabdomyolysis is exceedingly rare; Parker and Thompson found that fatal rhabdomyolysis associated with statin prescriptions occurred at a rate of 0.15 cases per 1,000,000 prescriptions.54 In a study of >250,000 patients, pravastatin was the least likely among several statins to result in a rhabdomyolysis-related hospitalization.55
Much more likely to occur than rhabdomyolysis among statin users are symptoms related to myalgia. Of 354 patients who self-reported muscle problems related to statins, 300 (85%) patients met formal criteria for probable or definite medication-adverse-effect (MAE) causality;56 93% of patients reported muscle pain, 88% reported fatigue, and 85% reported weakness. Atorvastatin users experienced more MAEs than lovastatin users. Higher potency statins caused MAEs in 100% of 39 rechallenges vs a 73% recurrence rate when lower potency statins were administered in the rechallenge. The MAEs also affected quality-of-life and functional domains in the survey.
Multiple studies have shown increased muscle injury measured by elevated CK levels after exercise in patients taking statins. Lovastatin resulted in significantly higher CK levels after treadmill walking.7 A study of Boston Marathon runners found a significant effect of statins on muscle injury as measured by both total CK levels and CK-MB levels 24 hours after the race in 37 statin users vs 43 marathoners who were not using statins. The study also found that older athletes were more susceptible to statin-associated muscle injury. No relationship between statin potency and differences in CK levels was observed.8
Even when patients do not experience muscle symptoms, muscle injury can occur when statin therapy is combined with ET, as measured by CK levels. The Effect of Statins on Skeletal Muscle Function and Performance (STOMP) study evaluated the effect of statins on muscle injury.53 This study randomly assigned patients to 6 months of atorvastatin 80 mg or placebo in a blinded manner. After 6 months, CK levels were slightly but significantly higher in patients receiving atorvastatin. This evidence of muscle damage occurred even in asymptomatic individuals. No change in exercise strength was observed between the 2 groups.53
Statin-associated symptoms of fatigue were reported in a study that randomized 1,016 patients to receive daily simvastatin 20 mg, pravastatin 40 mg, or placebo for 6 months. Patients rated their “energy” level and “fatigue with exertion” level at the end of the 6-month period. Statistically significant reductions in energy/fatigue scores occurred in patients taking statin medications compared to those taking placebo. The effect was most striking in women and in patients taking simvastatin.57
In a large, retrospective cohort study of physically active soldiers and veterans at Brooke Army Medical Center, statin users were compared with non–statin users. The statin users were found to be significantly more likely to have muscle strain, joint sprain, joint dislocations, or musculoskeletal pain than the non–statin users. The study required individuals to have received statin therapy for at least 90 days, and the average length of follow-up was approximately 2 years; 74% of the statin users used simvastatin.58
One of the most common patient concerns of the combined use of statins and ET is the decrease in athletic performance. Statins have been linked with decreases in athletic performance for many years. A 2010 literature review evaluated 6 studies assessing the effects of statins on muscular strength and 9 studies assessing the effects of statins on ET performance.59 The studies evaluating the effect on muscle strength were somewhat mixed. However, the best designed study in that group was a prospective cohort study of 774 individuals that indicated a significant decrease in leg strength and muscle quality in individuals aged 50-79 years who were using statins. Furthermore, the decrease in strength was reversible with treatment cessation.60
STATIN/ET INTERACTION BENEFITS
The benefits of ET are widely reported.61,62 People who participate in regular ET and who have higher levels of cardiorespiratory fitness have a reduction in all-cause mortality, coronary heart disease, and CVD mortality.61 ET reduces the risk of stroke, some cancers, type 2 diabetes mellitus, obesity, osteoporosis, and loss of function in old age, potentially enhancing brain health and function.63 Statins also reduce all-cause mortality when used to treat patients with hyperlipidemia, diabetes mellitus, and/or hypertension.64 A metaanalysis of 29 trials found that even in individuals with an estimated 5-year risk of CVD events of <10%, LDL cholesterol reduction was associated with a 1% absolute reduction in CVD events for 5 years.65
A study assessing >10,000 patients in the US Department of Veterans Affairs system demonstrated that statins and physical fitness independently correlated with reduced all-cause mortality. Furthermore, this study demonstrated that the combination of improving levels of fitness and statins produced an even greater reduction in mortality. The study found a relative risk as low as 0.30 in a highly fit population (metabolic equivalents >9.0) using statins, compared to a baseline of 1.35 in the least fit population (metabolic equivalents <5.0).66
ET decreases the risk of CVD by 30%-50%, an effect greater than expected if considering only its effect on traditional risk factors.1 ET also reduces LDL cholesterol, increases high-density lipoprotein,67 and lowers blood pressure. In patients without a predisposition to or diagnosis of CVD, statins reduce LDL cholesterol levels up to 50% and CVD events by 33%-50%.68 The combination of statins and ET has been shown to have additive benefits. ET itself seems to have benefits out of proportion to what one might expect from risk-factor modification alone. This effect may be the result of enhanced vagal tone and endothelial function. The beneficial interactions between this improved endothelial function and sympathetic outflow may ameliorate the deleterious effects of sustained hypertension on vessel walls.69 Conversely, and in support of this theory, increased sympathetic tone blunts dilation of the vessels in response to nitric oxide, released normally as a result of shear stress on the endothelial cells.70
POTENTIAL STRATEGIES TO LOWER THE RISK OF STATIN/ET INTERACTIONS
Multiple options exist to decrease the risk of adverse interactions between ET and statin therapy (Table).12 Limiting the quality or quantity of ET can decrease the risk of side effects. In the Prediction of Muscular Risk in Observational conditions (PRIMO) study, more intense ET increased the chance of myopathic symptoms.71 The PRIMO study found that 14% of subjects participating in intensive forms of sports had statin-related muscular symptoms vs 10.8% of subjects performing less active ET. Additionally, we have also reported cardiotoxicity with excessive endurance exercise, and most of the ET benefits are obtained at ET levels <40-45 minutes per day.72-74
Strategies to Decrease the Risk of Adverse Interactions Between Statin and Exercise Training (ET) Therapy
Changes in statin therapy can often result in improved tolerance of combined ET and statin therapy. Studies have shown that hydrophilic statins may be less toxic than lipophilic statins because of less predilection for the myocyte lipid membrane.17,75,76 However, in the PRIMO study, fluvastatin, a lipophilic statin, appeared to have a lower rate of muscular side effects.71
In the rat model, simvastatin and lovastatin, both lipophilic substances, are more likely to increase CK levels and to induce myopathy in skeletal muscle than pravastatin.77 In another study, simvastatin-treated rabbits were also noted to have more myotoxicity than rabbits treated with pravastatin.78 As further evidence of toxicity related to the lipophilicity of a given statin, cerivastatin—the most lipophilic of all of the statins—was removed from the market because of deaths resulting from rhabdomyolysis. In several studies, lipophilic statins have been shown to passively diffuse into myocytes.18
Cell culture experiments have indicated that certain statins appear to be much more intrinsically toxic to myocytes than others. Compared to both simvastatin and lovastatin, pravastatin was >100 times less toxic in decreasing rat myotubule protein synthesis.79 Avoiding harmful statin drug interactions should decrease the potential for elevated statin levels. Drugs metabolized by the CYP system, particularly those metabolized by CYP2C9 and CYP3A4, should be prescribed with caution.
Successful strategies include not only changing the type of statin but also adjusting the dosage of the drug. Recent studies have indicated that every-other-day statin use may be as effective as daily dosing in CVD risk reduction.80 In a retrospective cohort study of >100,000 statin users, >50% of the patients had discontinued the drug at some time during an 8-year period.81 Nearly 20% of the discontinuations were for statin-associated side effects. However, of the 6,579 patients who were rechallenged with a statin, 90% were able to tolerate some type of statin 1 year later. This study provides evidence that an individual who otherwise needs statin therapy should be considered for reinitiation of a statin even if a discontinuation was previously necessary.
CoQ10 may be a treatment option for patients with statin-associated myopathies, but some studies and large metaanalyses have failed to show a benefit.14,82 As previously described, low serum concentration of CoQ10 is common in patients taking statins. Atorvastatin produces a CoQ10-deficient state in mice and a resulting mitochondrial dysfunction.83 The deficiency and mitochondrial function were reversed with supplemental CoQ10. Indeed, CoQ10 has been shown to improve subjective fatigue sensation and physical performance,84,85 decrease muscle damage based on CK levels,86 and increase VO2 max. Caso et al found that 100 mg of CoQ10 decreased muscle pain by 40% after a 1-month treatment compared to treatment with vitamin E.87 In mitochondrial myopathies that produce a similar CoQ10-deficient state in muscle tissue, supplementation is likely an effective treatment.88 When lactate is used as a marker for muscle damage in patients with mitochondrial disorders, CoQ10 seems to diminish the initial rise in lactate upon exercise and increases VO2 max, although it failed to affect the total lactate level after exercise or improve overall exercise capacity in a 2010 randomized trial.89
In patients suffering from statin-associated myopathy, myalgia, and elevated CK levels, muscle biopsy specimens have revealed reduced CoQ10 levels.90 Cooke et al showed that CoQ10 supplementation increased both serum and muscle CoQ10 levels in athletes and nonathletes, increasing time to exhaustion.91 In older athletes prone to muscle damage and mitochondrial stress, a double-blind, randomized, crossover trial demonstrated that daily treatment with 200 mg of CoQ10 improved time to anaerobic threshold as well as muscle performance.3 In the animal model, CoQ10 supplementation increased CoQ10 levels in slow twitch muscle fibers and decreased ET-induced muscle injury.92
In 2012, Bookstaver et al conducted a randomized, double-blind trial of CoQ10 for the treatment of statin-associated myalgia.93 A population of 80 patients who experienced muscle pain in 2 or more extremities within 60 days of starting statin therapy were randomized to 120 mg CoQ10 (60 mg twice daily) or placebo. Pain was assessed using a 10-cm visual analog scale, as well as the short form McGill Pain Questionnaire. Despite observed decreases in both pain metrics after 30 days, no significant difference between treatment and placebo was observed. Likewise, in a study of simvastatin-associated myalgia, CoQ10 had no effect on myalgia as assessed by a visual analog scale.82
A review by Rosenfeldt et al found 6 studies showing improvement in exercise capacity with CoQ10 and 5 studies that did not.94 In 2007, Marcoff and Thompson reviewed the literature and concluded that the evidence for a benefit of CoQ10 in statin-associated myopathy was mixed, although they suggested that the low-risk profile of CoQ10 and its potential to improve clinical outcomes may warrant a therapeutic trial of CoQ10 for treatment of statin-associated myalgia, an opinion increasingly shared in the literature.14,95 The 2015 metaanalysis by Banach et al also failed to show that CoQ10 improved statin-associated myopathy.27
Another potential treatment of statin-associated side effects is L-carnitine. Carnitine is required for the transport of fatty acids across the mitochondrial membrane and energy production. Statins decreased carnitine levels in the rabbit model.96 L-carnitine may help with the possible disruption of mitochondrial membranes in patients with statin-associated myalgia. In rats, myotoxic doses of simvastatin resulted in significantly elevated levels of CK.97 This effect was reversed by administration of L-carnitine, and a concurrent improvement in walking ability was observed. Extrapolating carnitine dosing in these animal studies to potentially beneficial human dosing yields a human dose equivalent of 6 g of carnitine twice per day. However, most human studies have used doses of 3-6 g per day. Evidence exists of a high likelihood of underlying carnitine abnormalities or muscle disease carrier states in patients with statin-associated myalgia. These abnormalities include carnitine palmitoyltransferase-2 deficiency, McArdle disease carrier status, and lipid storage problems.98 These data suggest L-carnitine as a potential therapeutic option for further trials.
Vitamin D replacement in statin users with vitamin D deficiency may also be a successful therapy.48,99 In a 2009 study, replacing vitamin D and stopping the statin medication reversed myalgia complaints in 6 of 8 patients.48 Six of the patients agreed to retry statin medication while maintaining proper levels of vitamin D, and 4 of those patients tolerated the challenge without recurrence of myalgia for at least 6 months.
Other studies of large cohorts did not show a significant association between hypovitaminosis D and statin-associated myalgia. In a study of 129 patients, 57 patients with statin-associated myalgia and 72 patients without myalgia were compared.100 No statistical difference in vitamin D deficiency was observed between the 2 cohorts, using both the normal cutoff of 30 ng/mL as well as a lower cutoff of 15 ng/mL, suggesting that low vitamin D was not a likely underlying etiology in patients with statin-associated myalgia.100 A retrospective study of >5,000 patients using statins similarly found no difference in vitamin D levels between patients with myalgia and those without myalgia.101 A 2011 review by Gupta and Thompson concluded that, given widespread vitamin D deficiency, screening patients who experience problems with statin medications is appropriate, and normalization of low levels is otherwise indicated.29
CONCLUSION
Statins have been clearly shown to be potentially lifesaving medications and are indicated in many patients to decrease CVD risk. At the same time, caution should be exercised in prescribing statins and ET, particularly in high-risk groups. A cavalier approach to this combined therapy may unnecessarily expose individuals at risk to side effects, resulting in discontinuation of the treatment and subsequent increased risk for CVD events. Careful attention to identifying high-risk groups and strategies to prevent or treat side effects that may occur should be employed.
Clinicians have several therapeutic options when treating patients who perform ET and have statin-associated myopathy. Adjusting statin therapy by using the lowest possible dose, utilizing a hydrophilic statin, recommending a drug holiday followed by a rechallenge, or adding ezetimibe to enable LDL lowering on reduced statin dosage may be effective strategies. Although studies have not shown a consistent benefit, use of supplements such as CoQ10, vitamin D, or L-carnitine may be effective. Finally, keen attention should be given to avoid drug interactions known to increase the likelihood of statin myopathy.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care, Medical Knowledge, and Practice-Based Learning and Improvement.
ACKNOWLEDGMENTS
The authors have no financial or proprietary interest in the subject matter of this article.
- © Academic Division of Ochsner Clinic Foundation








{kind=link}