
Abstract
Background Variations in the origin, course, and branching of visceral arteries, particularly those of the celiac artery and superior mesenteric artery (SMA), are well documented in medical literature. Identifying any variation is necessary prior to abdominal surgery.
Case Report A 72-year-old male presented after a pancreatic body mass was incidentally found on abdominal computed tomography (CT). The CT revealed an anatomic anomaly of the splenic artery. The patient's splenic artery originated from his SMA rather than from his celiac artery.
Conclusion Accounting for this anatomic anomaly prior to performing an open distal pancreatectomy and splenectomy was essential to the surgery's success. Ligation of the splenic vein followed by early ligation of the splenic artery allowed for minimal splenic congestion. Preoperative planning and understanding the patient's unique anatomy minimized the risk of an adverse outcome.
INTRODUCTION
The splenic artery is the largest and most tortuous branch of the celiac trunk. After originating from the celiac trunk, the artery courses laterally, posterior to the stomach, and along the superior border of the pancreas. At the tail of the pancreas, the artery divides into its terminal branches that enter the hilum of the spleen.1 Variations in origin, course, and branching of visceral arteries, particularly those of the celiac trunk and superior mesenteric artery (SMA), are documented in medical literature.2 However, splenic artery origin from the SMA occurs infrequently. For certain abdominal surgeries, it is imperative to know the anatomic location of the splenic artery. An unforeseen variant in splenic artery anatomy could lead to inadvertent iatrogenic injury, prolonged operative time, and/or increased blood loss.
CASE REPORT
A 72-year-old male was referred for evaluation of a pancreatic body mass found unexpectedly on an abdominal computed tomography (CT) scan performed to investigate a possible aneurysm of the abdominal aorta. The patient reported back pain but was otherwise asymptomatic. CT with contrast revealed a 4.1 × 2.7-cm mass within the pancreatic body, resulting in dilatation and atrophy of the pancreatic tail. The splenic vein was obliterated, and the splenic artery was encased by the mass. The patient's arterial anomaly—his splenic artery originated from his SMA—was readily appreciated on the sagittal and coronal CT images (Figures 1A, 1B, and 1C).
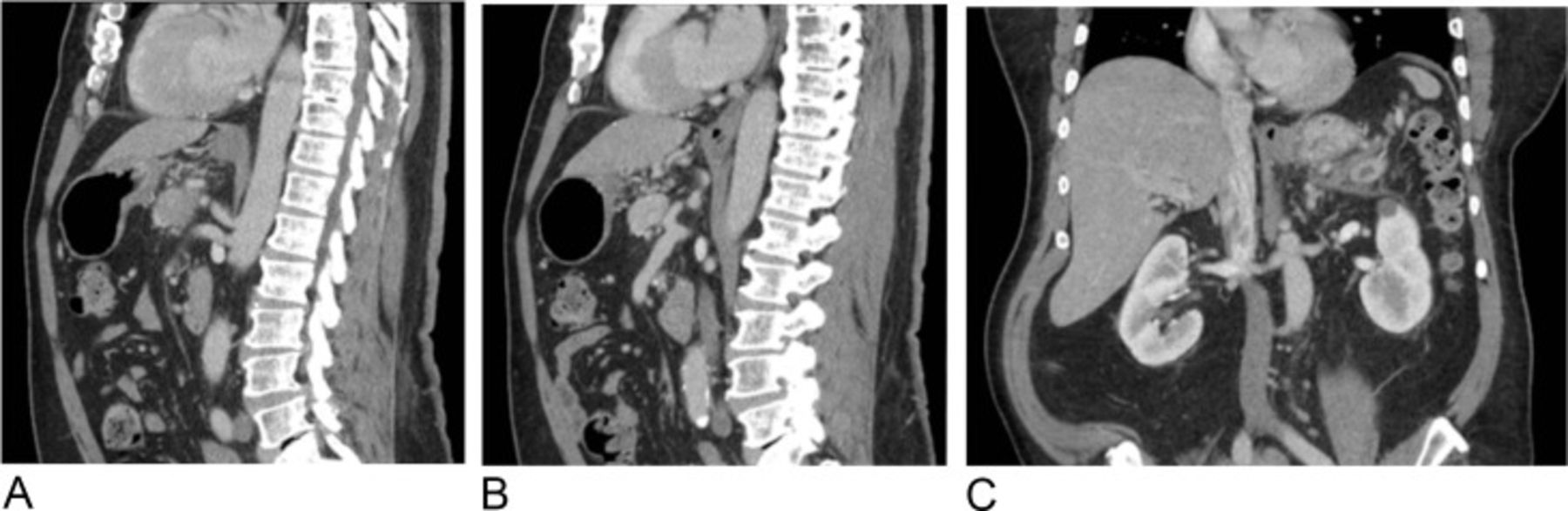
Preoperative computed tomography images show the celiac and superior mesenteric artery (SMA) origins from the aorta (A), the splenic artery's origin at the SMA coursing superiorly (B), and the splenic artery in the coronal view coursing superolaterally (C).
The patient's preoperative diagnosis was adenocarcinoma of the body/tail of the pancreas, and an open distal pancreatectomy with splenectomy was completed. After the neck of the pancreas was divided for distal pancreatectomy, the splenic artery was identified. The splenic artery was traced to its origin at the SMA as the SMA was surgically dissected proximally to the aorta. After originating from the SMA, the splenic artery branched laterally, posterior to the pancreatic body and tail. Normally, the splenic artery courses superior to the splenic vein, and the artery can be ligated before the vein to minimize venous congestion of the spleen. In this case, the splenic artery was located directly posterior to the splenic vein. Therefore, the vein had to be ligated initially to obtain adequate visualization for the ligation of the artery. With the superior mesenteric vein, portal vein, and splenic vein easily visualized, the splenic vein was divided at its confluence. This division allowed visualization of a 2-cm segment of splenic artery (Figure 2). The splenic artery was then ligated and divided rapidly to minimize venous congestion. With the splenic artery divided, the open distal pancreatectomy with splenectomy procedure continued in the standard fashion with an en bloc segmental tangential resection of the proximal small bowel adherent to the mass. Planning for this anatomic variant of the splenic artery was imperative to successfully completing the procedure.
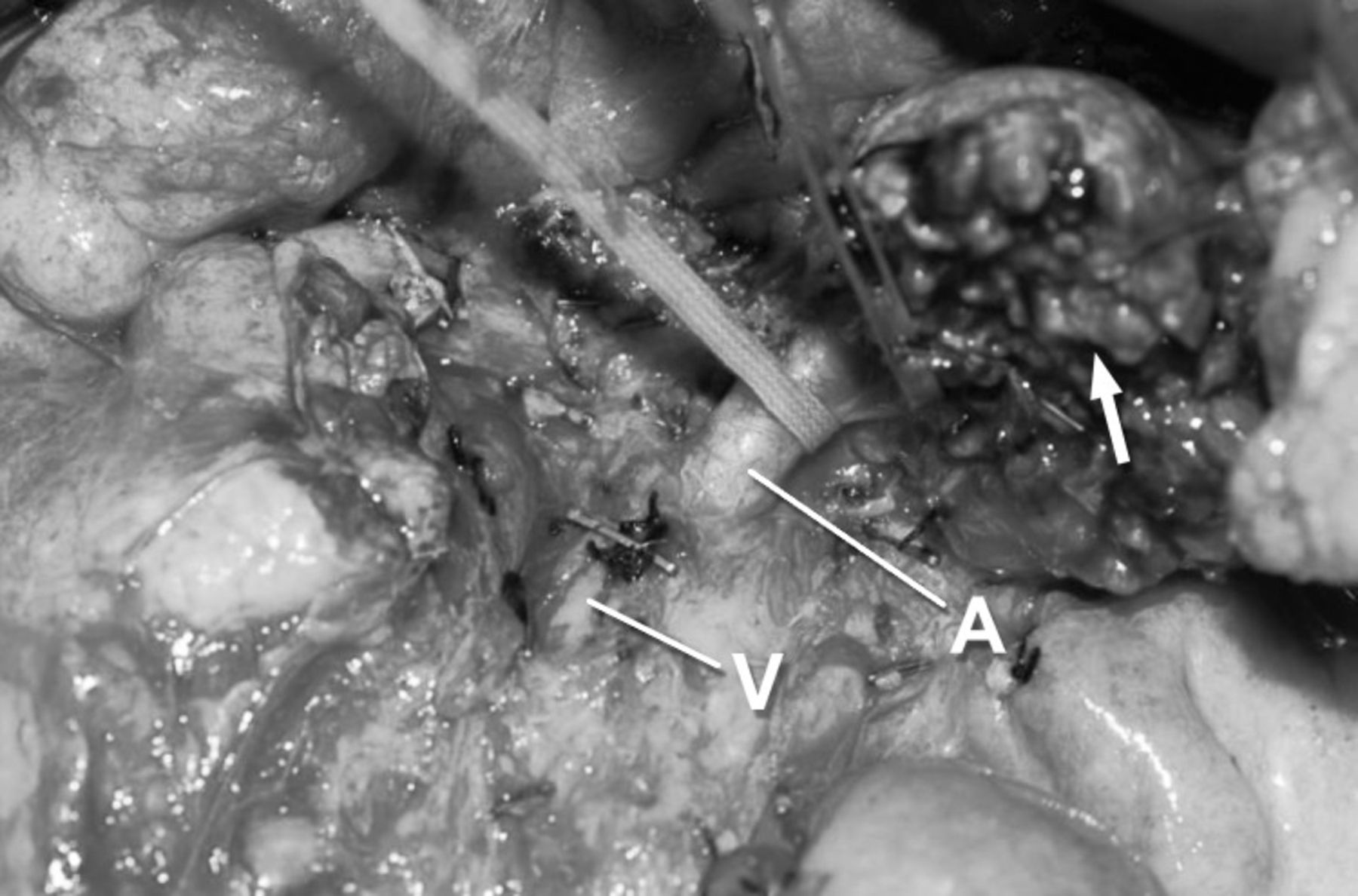
Photograph shows umbilical tape around an isolated 2-cm segment of splenic artery (A) before ligation and the splenic vein (V) divided at its confluence. The arrow shows the body of the pancreas divided anteriorly.
The postoperative diagnosis was adenocarcinoma of the body/tail of the pancreas as expected. The margins were clear with 14 negative nodes.
DISCUSSION
Trifurcation of the celiac trunk into the hepatic, splenic, and left gastric arteries is the usual anatomy in 86% of humans,3 but trifurcation appears to be incomplete in 9%.2 The origin of one or more of the main branches of the celiac trunk from the SMA is present in 7% of cases.2 In 2013, 36 studies were analyzed in a systematic review of celiac trunk variants. This review found that the hepatogastric trunk with the splenic artery arising independently from the SMA had an incidence of 0.03% (3 of 9,829).4 In a study of the positioning of the splenic artery in relation to the pancreas, 74.1% were suprapancreatic, 2.8% retropancreatic, and 4.6% intrapancreatic.1 Similarly, in a case report of 28 cadaveric splenic arteries, 90% were suprapancreatic, 8% were retropancreatic, and 2% were intrapancreatic.5 In our case, the splenic artery was retropancreatic. Because of the variant, the artery was posterior to the splenic vein. Proper recognition of the splenic artery's position preoperatively enabled the surgeon to quickly ligate the artery after the vein, minimizing splenic congestion and potential blood loss.
CONCLUSION
Proper preoperative planning allowed the surgeon to perform an open distal pancreatectomy and splenectomy while minimizing adverse events. If this anatomic anomaly had gone unrecognized prior to surgery, it could have prolonged operative time, increased blood loss, caused iatrogenic injury, and/or increased morbidity. Recognition of this anomaly is also important in other abdominal surgeries, especially upper gastrointestinal procedures, pancreatic surgery, and abdominovascular surgery.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care and Medical Knowledge.
ACKNOWLEDGMENTS
The authors have no financial or proprietary interest in the subject matter of this article.
- © Academic Division of Ochsner Clinic Foundation
In this issue








{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.