
Abstract
Background: Demographics are changing on a global scale. In the United States, an aging population continues to work, either by preference or because of insufficient resources to retire. Of even greater importance, a younger generation, referred to as the Millennial Generation, will soon predominate in the workforce and even now accounts for nearly 100% of resident physicians. By the year 2020, there will be 5 generations in the workplace.
Methods: This paper defines and details the characteristics of the 5 generations and examines how the vision, attitudes, values, and expectations of the most recent generations will reshape the workforce and graduate medical education.
Results: The need for change is imminent to educate the next generation of physicians. Among the changes necessary to adapt to the multigenerational challenges ahead are adopting mobile devices as preferred communication tools; using social networking sites to recruit residents; adding games, simulations, and interactive videos to the curriculum to engage students; breaking down departmental silos and forming learning teams that come from different specialties; developing benchmarks and milestones to measure progress; extending the social learning ecosystem beyond the resident years; embracing diversity as the norm for both practice and learning; and providing both coaching and mentoring.
Conclusion: For decades, resident physicians have shown commitment, tenacity, and selflessness while shouldering the dual responsibility of patient care and the pursuit of their own education and skills development. Resident engagement has been shown to drive change in undergraduate medical education and in the learning and performance of their teachers. The latter is evidence of reverse mentoring that will be a major factor for improvement in this digital age. We have only to embrace this opportunity to the benefit of our patients, our learners, and ourselves.
INTRODUCTION
Demographics are changing on a global scale. In the United States, an aging population continues to work, either by preference or because of insufficient resources to retire. Of even greater importance, a younger generation, referred to as the Millennial Generation, will soon predominate in the workforce and even now accounts for nearly 100% of resident physicians. By the year 2020, there will be 5 generations in the workplace, and the majority of them will be Millennials (Figure 1).1
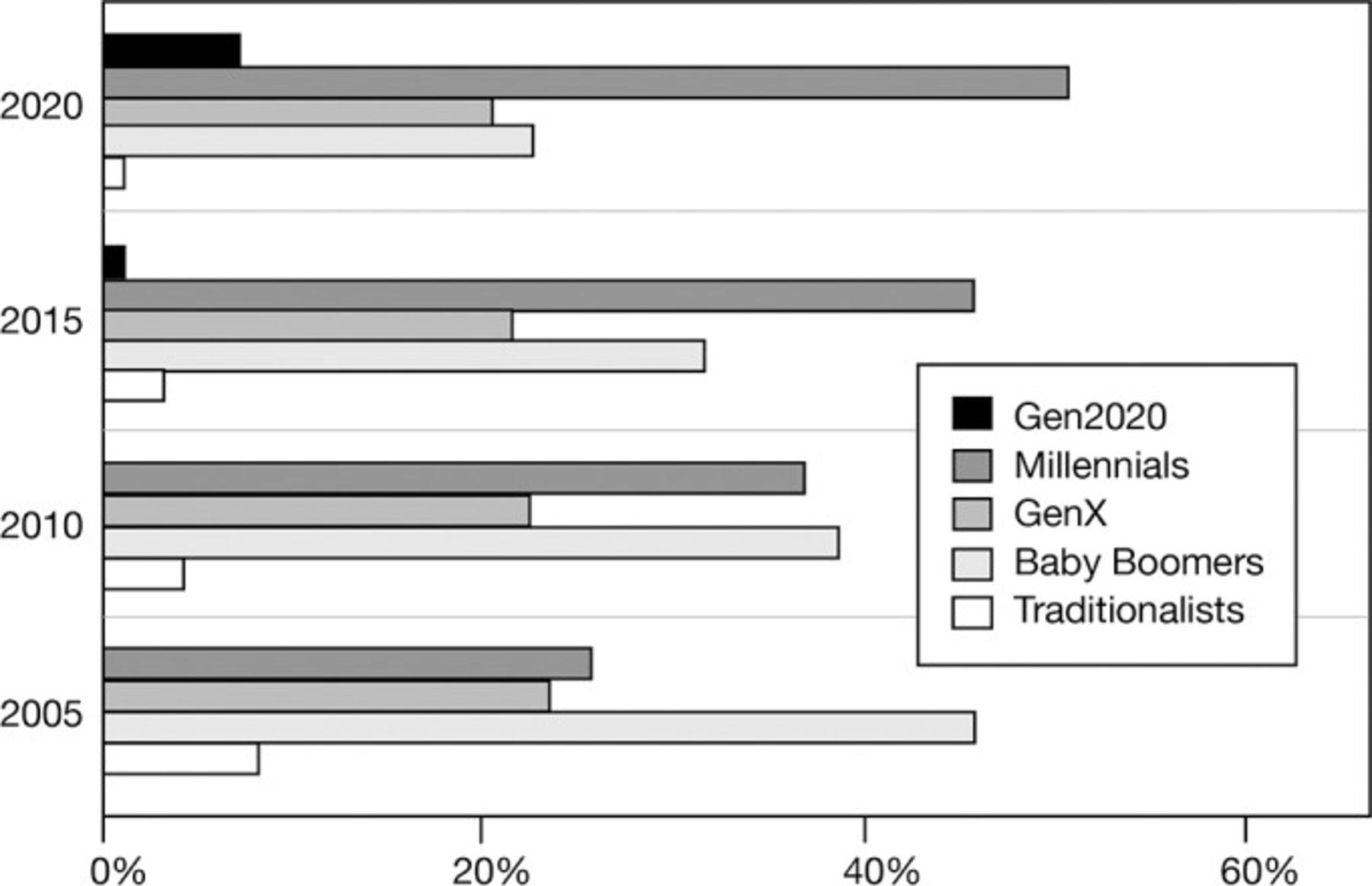
Five generations in the workplace (source: US Bureau of Labor Statistics1).
The generations differ in their perspectives on personal life and work and have different expectations that must be addressed by their teachers, mentors, coaches, and leaders. The Millennial Generation and the coming generation are technologically adept, far beyond the capabilities of their older peers. They are comfortable with diversity and social media, and they enjoy social networking and social learning. Graduate medical education must adapt and reform to successfully educate the next generation of physicians.
Now more than ever, graduate medical education must change to accommodate new generations of learners and prepare them for entry into the practice of their chosen specialty. To prepare for the changes necessary to educate the new generations, it is important to understand the 5 generations currently involved in both the educational sphere and the workplace: Traditionalists, Baby Boomers, Generation X, the Millennial Generation, and Generation 2020.
A CHANGING WORKFORCE
The Millennial Generation will soon predominate in the workforce, and another generation will soon enter the college ranks and subsequently enter the job market or postgraduate studies. The Millennial Generation will account for more than 50% of workers in 2020, and Generation 2020—the 5th generation—will account for another 10%.1 In 2005, Baby Boomers were predominant, accounting for more than twice the percentage of the next most numerous generation. In 2020, that statistic will be reversed, and Millennials will outnumber all the other generations added together.
The Pew Research Center has published an extensive survey of attitudes and characteristics of the Millennial Generation and draws comparisons with previous generations, specifically the Boomers.2 Previously, 2 other authors examined the forces and environment that shaped the Millennial Generation as they were growing up and drew stark comparisons with the workforce they will continue to join.3,4 In 2007, the Nortel Corporation published a position paper titled “Hyperconnectivity: An Unstoppable Force of Change” that details the tremendous impact on recent generations, especially with the flood of mobile devices that perform a myriad of functions beyond those of a mere phone.5
Industries other than healthcare have growing concerns about the coming years. In a highly referenced and detailed white paper from Hewitt Associates,6 the authors describe an unstoppable and radical transformation characterized by a smaller and less skilled workforce that is increasingly global, highly virtual, vastly diverse, autonomous, and empowered. Corporations such as Deloitte Consulting7 and organizations such as the American Hospital Association8,9 are concerned about the multigenerational workforce and are also anticipating another certainty: the available workforce is shrinking. Meister and Willyerd10 predict a global shortage of workers, particularly in Russia and China, and point to the year 2020 as a turning point. Consequently, by 2020, countries including China, Germany, and the United States will have to deal with this shortage. Graduate medical education may not face severe reductions in the numbers of qualified people, but faculty will have to change curricula and develop new teaching skills to meet the needs of the learners in their programs.
As detailed below and presented in the Table, the generations differ in their perspectives on personal life and work and have differing expectations that must be addressed by their teachers, mentors, coaches, and leaders.
Characteristics of the Five Generations
The Five Generations8,10,11
The Traditionalists, also known as the Silent Generation or Veterans, were born before 1946 and currently number about 46 million people. In terms of demographics, they have replaced The Greatest Generation who were born before 1928. Traditionalists grew up during the Depression and then went directly to war. They were in uniform for the duration of World War II, and these experiences shaped their attitudes and beliefs. They believe in duty and sacrifice and are used to working with limited resources. They value accountability, responsibility, and practical experience. They are loyal to their employers and expect corporate and institutional loyalty in return. They value academic credentials and believe in tenure; their learning experience was mainly didactic with dependence on rote memorization during their early years. They are patriotic and respect authority; many of them were back in uniform during the Korean War. By 2020, all the members of this generation will be older than 74, and some of them will still be working.
Baby Boomers were born between 1946 and 1964 and currently number 78 million. They are also referred to as the Cold War Generation or the Economy Generation because of the rapid growth in the US and world economies that occurred during their adult years. Some of the older Boomers are now retired; the younger members of the cohort are still working and are in senior management. Despite an early rejection of the values and politics of their parents during the Vietnam era, they are driven by success and are goal oriented. Boomers value team building and relationship building. Their metrics for job performance are hours worked and financial rewards. In their view, their career equals their identity, but they are concerned with work-life balance and view the two spheres as separate entities. They grew up watching television; by 1958, 83% of families had at least one television in the home. Through this visual medium, they were exposed in almost real time to the Vietnam War, the Kennedy assassination, and the rapid development of the space program and NASA (the National Aeronautics and Space Administration). As adults they witnessed the development and release of the personal computer in 1981, initially at work and then as a tool for home use. They are the parents of the Millennial Generation.
Generation X, the Gen Xers, were born between 1965 and 1980, a relatively short time span compared to the other generations. This generation is currently about 50 million people; because of their numbers and short time span, in the generational analysis they have been referred to as the Sandwich Generation. Older Gen Xers are in senior management positions; others are in mid-career. They were defined by social changes, most notably the high increase in the divorce rate. These were the latchkey children, used to being alone and responsible. They are self-reliant, independent, and entrepreneurial. They highly value free time and time with family and seek work-life balance, much like the Boomers. They are loyal employees but are risk averse; they respect production over tenure. Other social and economic changes that shaped them include the AIDS epidemic, the Gulf War, and the 1987 market crash. They generally respect but do not trust authority, and they do not trust government. They are concerned that they will not have adequate resources to retire.
The Millennial Generation, also referred to as Gen Y, Net Gen, the Google Generation, or Echo Boomers, were born between 1981 and 1996. The older end of this cohort is working, and the more junior Millennials are completing their formal education. They are digitally competent, confident, and hyperconnected through the internet, personal computers, and mobile phones. They have Facebook accounts, use Google to the point of turning the noun into a verb, and watch YouTube. They do not read newspapers, use email, or watch television; e-learning solo is their least preferred learning preference compared to experiential learning, even if it is a simulation or computer game. They are highly educated, optimistic about their future, in a hurry, and broke. This generation has been the hardest hit by the downturn in the economy. They are innovators and communicators and are team oriented. They have definite expectations for their jobs and careers. They attach major importance to an employer that offers challenges and will expand their skills; a repeated requirement is the ability to find a coach and mentor to progress in their organization—the faster the better. They assert that if these expectations are not met in a job, they will quit. Another requirement is employment by a firm that has integrity and social responsibility, given the misbehavior of highly paid executives in their formative years. When the subject of work-life balance is broached, they indicate that there is no difference between work and personal life; it is a continuum. Thus, to them work-life balance is passé and irrelevant. Consistent with this world view, the results of one study show the ease with which they move seamlessly from work to free time. When asked to submit a stick drawing of themselves at work and another drawing of themselves at leisure, the Boomers showed distinct differences in apparel and accoutrements. When Millennials were asked to perform the same task, their 2 drawings were nearly alike; eg, a woman might add high heels and jewelry to her work figure but little else. This attitude has led to their designation as the “no-collar” generation, emphasizing their attitude that every day should be a dress-down Friday.12
Generation 2020 is still defining itself; what is apparent is that this generation born after 1997 will be even more hyperconnected and facile with computers and the internet than the Millennials. Their web experience began even before they started school with sites such as Disney's Club Penguin and Webkinz. Many middle school children merely tolerate their formal classroom experience until they can return home and go online. They have a sophisticated world view when polled, with expectations of global learning opportunities, comprehensive personal medical data storage, and limitless opportunities for experiential learning and strong peer groups. Their mobile device will be their office, classroom, concierge, music player, video player, computer, and phone—all rolled into one. In 2020, this generation will be freshman medical students. Among graduating high school students in this generation, college attendance is predicted to continue to fall, with as many as two-thirds of these students foregoing college to seek immediate job opportunities because of the high costs of postsecondary education and the inability to manage the debt. The hyperconnectivity of this generation will further challenge educational systems at all levels, including graduate medical education.
Generational Self-View
The generational characteristics described above were generated by research groups, especially the Pew Research Group.11 Another aspect of the Pew report is relevant. In a poll of 4 generations, the Pew researchers requested a free text rather than a multiple choice response to the question “What makes your generation unique?” Traditionalists, Boomers, and Gen Xers all thought they were unique because of their work ethic. Boomers and Traditionalists also listed values and morals. Millennials and Gen Xers listed technology use. Also in the top 5 responses for Millennials, not listed by other generations, were music/pop culture, liberal attitudes, and clothes. All 4 of the generations thought they were unique because they are smarter than the other generations. This response is echoed in the Millennial opinion that older generations have much to learn from them.
THE SOCIAL LEARNING ECOSYSTEM
Graduate medical education will be challenged by the tendency for Millennials and Generation 2020 to prefer social learning, and this preference will drive change.
Meister and Willyerd10 have developed what they define as a social learning ecosystem that divides learning into competency-based learning and context-based learning (x-axis) and further into content created and guided by organizations and content created and guided by users (y-axis). This model displays in 4 quadrants (Figure 2). Graduate medical education has traditionally concentrated on quadrant 1. Consideration of the 4-quadrant model has application to the future direction of graduate medical education.

The social learning ecosystem (adapted with permission from Meister and Willyerd, The 2020 Workplace: How Innovative Companies Attract, Develop and Keep Tomorrow's Employees Today10).
Quadrant 1: Guided Competency Development
Quadrant 1 represents formal learning and primarily features the lone learner model. This model has application going forward, but current residents do not like being assigned a module complete with a slide show followed by an array of questions. They consider such a presentation dry, dull, stale, and unworthy. They want a fun social learning experience. They complain that conferencing on the computer has taken the worst of live presentations and put them on the web, ie, death by PowerPoint and talking heads.
An example of turning a topic that is dry, dull, and boring into an experiential learning encounter is the method of teaching finance at www.celebritycalamity.com. This activity allows the learner to save a celebrity from financial disaster while learning aspects of credit, finance, annual percentage rates, credit costs and limit, and debt management.13 Similar programs are being developed in medicine so people will participate voluntarily instead of on command. For example, the Institute for Healthcare Improvement Open School has developed modules that have been popular with medical students and residents despite the 16-hour time investment. However, they tend to navigate the modules in a group setting. Pedagogy has gone digital.
Quadrant 2: Guided Contextual Learning
Quadrant 2 represents experiential learning. One application in medicine is simulated learning, but this modality has not progressed as far as originally hoped. One issue is the style of teaching that accompanies simulated learning. Because of the lack of slides and the canned talk in the simulation environment, the style of teaching is more that of a facilitator than a dogmatic teacher. Few in medicine have taken the time to develop this skill. Once achieved, the results are dramatic, and the best learning results when the facilitator does not know what is coming next in the scenario but rather works with the students to solve the problem and take appropriate action.
Another technique for guided contextual learning is on-demand mentoring. The activities of a coach and a mentor are often confused, although at times there is overlap. On-demand mentoring is anonymous, asynchronous, and confidential. The mentor must be outside the reporting line of the individual; otherwise this type of learning is coaching.
Last, we can consider mobile learning a component of this quadrant because the Millennial Generation and the generation to follow do not distinguish between work and outside-of-work life.
Quadrant 3: Social Competency Development
Mentoring can also fit in quadrant 3. Some industries refer to this kind of learning as stratified talent management. It is mentoring according to groups. In graduate medical education, a system could potentially be designed for postgraduate year (PGY) 1 and PGY 2 residents, another for PGY 3 and PGY 4, and another for fellowship positions. Twitter provides a means for giving on-demand microfeedback (limited to 140 characters) as Millennials want constant feedback on both performance and career development. To complete the teaching-learning cycle, leader feedback should be immediate. For example, following a presentation, the presenter might want a short analysis. Was the presentation relevant? Good content? The right amount of time dedicated to the subject?
Quadrant 4: Social Contextual Learning
Quadrant 4 represents peer-to-peer learning, and it should be individualized. Given advances in information technology and platforms, participation in content generation by users (resident physicians) is limitless. Knowledge sharing will improve learning and retention through the power of learners connecting with one another.
Organizations on the forefront of innovation and corporate learning have invested heavily in peer-to-peer learning. One example is British Telecommunications (BT) that has developed the Dare2Share corporate social learning network that extends beyond the classroom.11 A BT employee survey indicated that 78% of employees preferred to learn from their peers. The goal of Dare2Share is to develop learning that is “more relevant, immediate, and presented in the context of everyday work.” The result of working within this quadrant is not to replace formal learning but to augment and to formalize social learning.
Practical Application of the Social Learning Ecosystem
An anecdote demonstrates the usefulness of the social learning ecosystem model. A basic science department chair, along with two senior members of the faculty, approached the dean of the medical school with a complaint. They were upset that students were not attending class; fewer than one-third of the class was present for any given lecture. They complained that responding to the demands of the students to provide an extensive syllabus was a major cause of the absenteeism, and they insisted that the dean enforce mandatory attendance.
The dean took the complaints under consideration but with the knowledge that the class had averaged in the 90th percentile on the recent United States Medical Licensing Examination (USMLE). Informal conversations with students indicated that they enjoyed studying the discipline, and class enthusiasm was at a high level.
The dean further learned that two of the junior faculty, on their own time, had organized study sessions outside of the formal curriculum, resulting in guided contextual learning and peer-to-peer learning. Delving deeper, she discovered that one faculty member had identified a classroom with moveable furniture for Saturday sessions. The classic classroom had a podium for the teacher in the front of the room with tables for seating 3 rows of 8 students. In the classroom with moveable furniture, placing her workstation in the center of the room resulted in 4 radials of 6 students, 3 on each side of the table. Students could easily see and speak with every student in the room as they went through a guided exercise. Thus, each student supported not only his/her learning but learning in the peer group as well.
Our own research relates to this model. We used the Kolb Learning Style Inventory to assess the preferred learning style of 90 PGY 1 residents in various programs.14,15 The survey places the learner on an x-axis of active experimentation vs reflective observation (processing along a continuum) and a y-axis of concrete experience vs abstract conceptual thinking (the perception continuum). The resulting 4 quadrants identify preferred learning styles: converging, diverging, accommodating, and assimilating. We stratified participants into anesthesiology, surgery, and internal medicine. The anesthesiology and surgery residents were clustered lower on the perception continuum, ie, toward abstract and conceptual thinking, and were evenly distributed along the processing continuum. Internal medicine house staff and fellows were randomly distributed in all 4 quadrants.15
Next, we compared anesthesiology faculty and their preferred learning style with anesthesiology residents (16 faculty and 25 residents), and their learning styles were identical.16 When anesthesiology and surgical residents were interviewed, they indicated they did not care for lectures but attended them. They did not take notes. They viewed attendance at lectures as a social compact to meet and interact with their peers. They had a positive response to simulation, but for technical and procedural learning they preferred to “YouTube it” and review a procedure on their own time, at their own pace, with repetition until they achieved “learning satisfaction.”
Important to note is that the Kolb concept of organizational learning requires moving through all 4 quadrants to address the preferred style of all learners.
SPECIFIC CHALLENGES TO GRADUATE MEDICAL EDUCATION
Given the predictions that the Millennial Generation will predominate in the workforce and in the learning force and that a generational gap will occur, the need for change is imminent to (1) educate the next generation of physicians and (2) ensure an adequate number and quality of physicians and other providers necessary to care for patients. The following suggestions are consistent with those of demographers and leaders in the business community to help achieve these goals.
1. Mobile devices will prevail as preferred communication tools. The expansion in technology will be extraordinary, and the ability to protect information will expand accordingly. Learning and information will be available on demand. Adapting teaching methodologies to mobile delivery will be necessary to enhance social learning.
2. Resident recruiting will encompass social networking sites. The current method of resident recruitment is flawed. Sorting by USMLE scores, Alpha Omega Alpha membership, class rank, or other parameter occurs too frequently and results in an event-driven recruiting technique (completing the forms at the Electronic Residency Application Service). The process of learning for individual medical students will be available on their social networking sites and will be individualized and much more representative of the student's learning potential and work ethic than the parameters currently used to select residents.
3. The resident curriculum will use games, simulations, and interactive videos as delivery modes to engage students who have grown up with Webkinz, game devices, and interactive videos such as those available at the Khan Academy website.17,18 Salman Khan, the educator who created the nonprofit Khan Academy in 2006 to provide “a free, world-class education for anyone, anywhere,” has devised his videos (stop it, rerun it, review it, and then proceed after you get it) to great effect. Other industries foster learning with alternative reality games to engage learners in a highly collaborative and social experience to not only learn complex skills but also to engage in critical thinking and problem solving.
4. Better learning and improved practice will be achieved by breaking down departmental silos and forming learning teams that come from different specialties. For example, a problem in diagnosis may involve surgery and radiology; the management phase will involve teaming with surgery and anesthesiology; and further care might depend on internal medicine, physical medicine, and other specialties.
5. Progression through residency will no longer simply be in the time domain. Benchmarks and milestones will be developed to measure progress. In parallel with the changes in resident recruiting, certification by board examination, computer-based examination, and/or oral examination will include considerations/evaluations beyond the examination score.
6. The responsibilities of program to resident and of resident to program will be ongoing after graduation: the social learning ecosystem will extend beyond the resident years, and ongoing education will be interactive. The practitioner will maintain a learning portfolio, one that started during residency, to maintain maintenance of certification in the specialty.
7. Diversity will become the norm for both practice and learning. Multicultural talent within any organization will be a strategic business priority, and graduate medical education will be no exception. In addition to ethnic and gender diversity, workers across the 5 generations and international citizens will strengthen healthcare education and delivery.
8. It will be an imperative to understand the difference between coaching and mentoring and to provide both.19,-,21 Feedback will be expected with short turnaround.22 Annual or quarterly evaluations will not be replaced but will be insufficient to meet the needs of the Millennials and Generation 2020.
9. Generational differences will have to be addressed to facilitate learning and the development of the 6 Accreditation Council for Graduate Medical Education competencies and to ensure practice-based learning and lifelong learning. The focus on the resident cohort is appropriate because they quickly move into practice settings. Also, this emphasis is the fastest and most efficient way to drive change in medical education and practice.23
CONCLUSION
Never before have 5 generations of physicians been working and learning together. The challenges to build teams and support interactive learning are daunting, but with challenges come opportunities. For decades, resident physicians have shown commitment, tenacity, and selflessness while shouldering the dual responsibility of patient care and pursuit of their own education and skills development. Resident engagement has been shown to drive change in undergraduate medical education and the learning and performance of their teachers. The latter is evidence of reverse mentoring that will be a major factor for improvement in this digital age. We have only to embrace this opportunity to the benefit of our patients, our learners, and ourselves.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care, Medical Knowledge, and Professionalism.
ACKNOWLEDGMENTS
The authors have no financial or proprietary interest in the subject matter of this article.
- © Academic Division of Ochsner Clinic Foundation








{kind=link}
{kind=link}