
Abstract
Background: Oral case presentation is an essential skill in clinical practice that is decidedly varied and understudied in teaching curricula.
Methods: We developed a curriculum to improve oral case presentation skills in medical students.
Results: As part of an internal medicine clerkship, students receive instruction in the elements of a good oral case presentation and then present a real-world case in front of a video camera. Each student self-evaluates his/her presentation and receives evaluations from his/her peers. We expect peer and self-evaluation to be meaningful tools for developing skills in oral presentation.
Conclusion: We hope to not only improve the quality of oral case presentations by students but also to reduce the time burden on faculty.
INTRODUCTION
When done correctly, oral case presentation is a powerful clinical skill. A fluent case presentation allows for efficient and effective transitions between providers. Such communication is essential within and between provider teams and between physicians and supporting staff. The oral case presentation also serves as a useful proxy for assessing student competency in clinical reasoning and patient care.1-3
Despite its clear importance, oral case presentation has not been consistently and effectively taught in medical school. Student and faculty perceptions of the oral case presentation vary widely.3 Evaluations of the oral case have also varied, and the variation has been attributed to interrater variability4-6 despite attempts to standardize the process.7 The variance in expectations is exacerbated by nonspecific faculty feedback that forces students into formative changes contrary to the intent of the feedback.8
Course directors and clinical educators have defined what makes an excellent oral case presentation.9,10 Some have attempted to develop curricula that standardize training based on these expectations11 or curricula that go beyond standardization alone.2 In 2012, Heiman et al assessed a curriculum that takes advantage of both online learning modules and deliberate practice in the preclinical years.12 These methods are effective but are time and resource intensive and require significant faculty involvement.
Other studies of interventions to improve case presentation skills have shown mixed results for the outcome of summative end-of-clerkship evaluations; however, summative ratings may have poor accuracy and reliability for assessing specific skills.11,13 No study has assessed the direct instruction and evaluation of oral case presentations, nor has any compared peer and self-evaluation to the evaluation of faculty members.
The purpose of this education innovation was to create a sustainable, scalable method of coaching and evaluating oral case presentations. Our objective was to develop a curriculum that (1) aligns faculty and student perceptions of the purpose of oral case presentation, (2) clarifies what makes an excellent oral case presentation, and (3) trains students to communicate effectively and efficiently with the healthcare team. To accomplish these objectives, we developed evaluation criteria that meaningfully assess the elements of the oral case presentation with a clear aim to foster growth. We hope the methodology also helps with coaching and aids peer and self-evaluations free of faculty commitment. It should allow for real-world implementation rather than sterile simulation.
Success will be defined by affirmative answers to 2 questions: Can a brief curriculum within the internal medicine core clerkship improve the ability of medical students to present oral cases? Can this process alleviate faculty time burden by using peers as evaluators and self-reflections as means to improve the measured skill?
THE COURSE
Three oral presentation sessions are scheduled as part of the internal medicine clerkship at Baton Rouge General. The first session occurs during the second week of an 8-week block. Students, independent of their peers, bring a history and physical of a patient they have admitted and present an oral history and physical in front of a camera. The session is repeated at weeks 5 and 7. The students record 3 separate oral presentations at weeks 2, 5, and 7 that are both peer and self-evaluated.
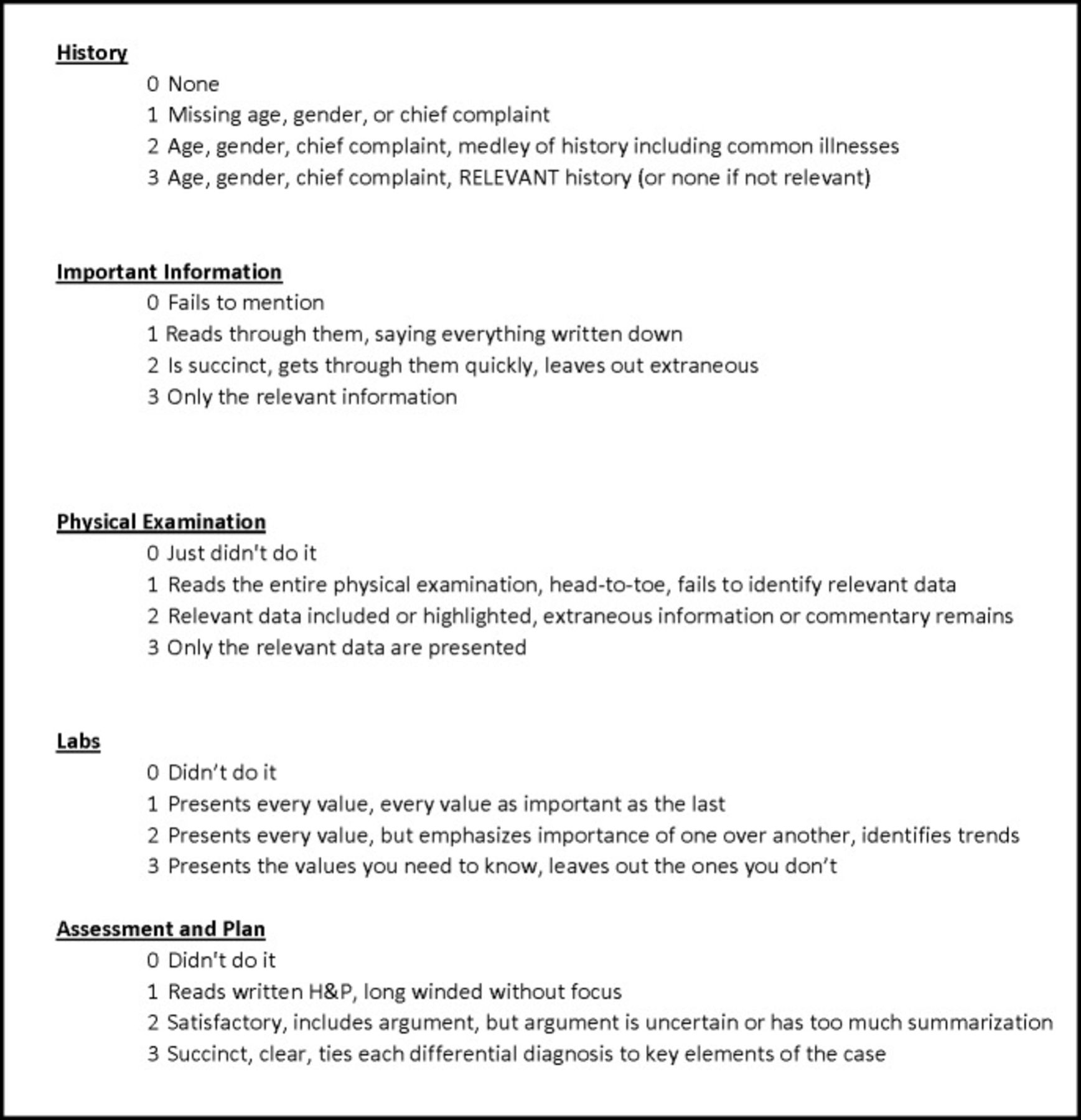
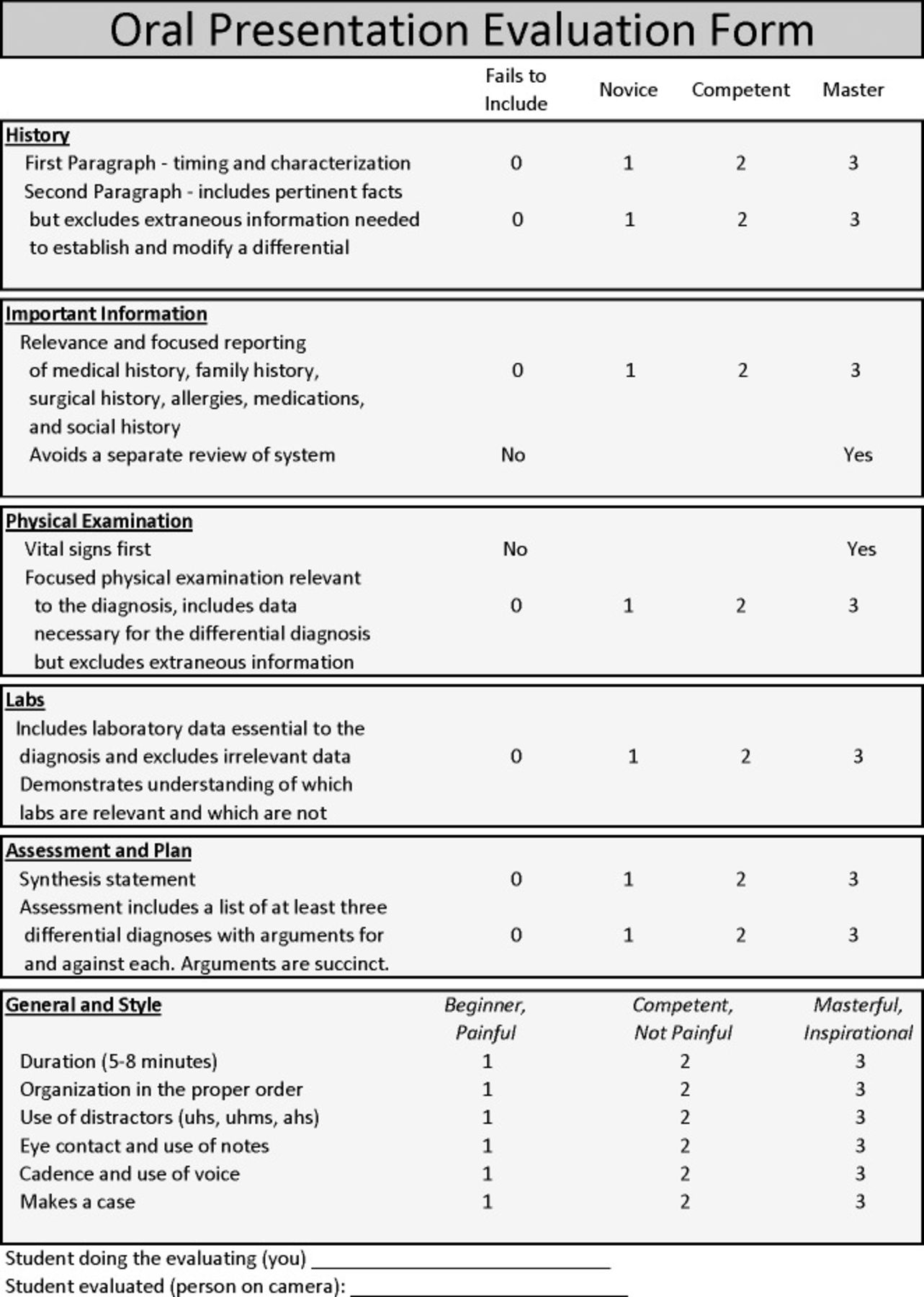
After the first session, students are given a perception survey (Figure 1) followed by a 30-minute lecture by the clerkship director that demonstrates the differences between the written history and physical and the oral case presentation, as well as their significance. Students then watch 2 prerecorded case presentations; one is excellent, and the other is abysmal. The clerkship director reviews what makes a strong case presentation vs a poor case presentation. The session concludes with an explanation of the scoring system (Figure 2) and the scorecard itself (Figure 3).

Perception survey distributed to students at the beginning and end of the course.
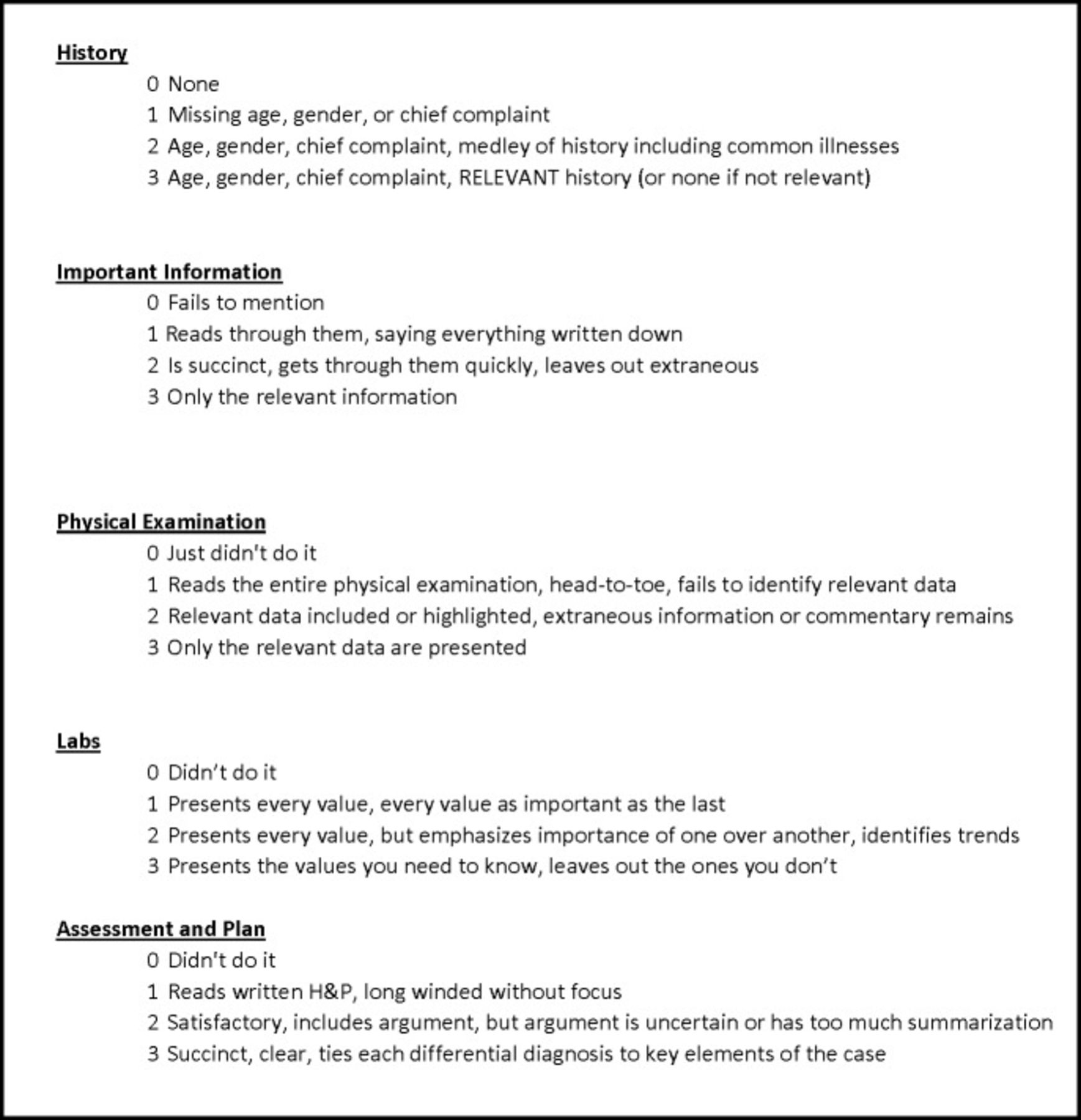
Explanation of the scoring system. H&P, history and physical.

Oral presentation scorecard.
At the end of each session, students have 72 hours to evaluate themselves and each other. The videos are uploaded to an unlisted YouTube channel and are hosted for free, viewable only by those with a link. At the end of 72 hours, the videos are changed to private, viewable only with a Google account and a specific invitation. Students view the videos individually on their own time, rather than in a group environment.
Assessment is performed through an evaluation tool (Figure 3) that has been converted to a web format for ease of data storage and acquisition. Scores are reported to the students.
For the initial study, faculty members also viewed the videos at the end of the block. If data demonstrate that the students can reasonably evaluate their peers as well as faculty can evaluate their peers, faculty evaluation will be eliminated from the model.
To ensure that students accurately evaluate each other, they are instructed that the portion of their grade represented by this evaluation is based on how closely their evaluations match faculty evaluations, not necessarily how well they perform on the video. Higher scores do not necessarily mean a higher grade; demonstration of accurate measurement drives scoring.
THE TOOL
Members of the Clerkship Directors in Internal Medicine (CDIM) have provided recommendations for what makes a good oral case presentation,9 and Green et al reported what hospitalists and clinical educators in practice thought was important.10 Attempts at developing tools to assist in education and evaluation have also been made.11,13 One, published by faculty at Northwestern, took the approach that the teaching tool should be the evaluation tool.12 We adapted this approach as the underlying foundation for our evaluation of oral case presentations but expanded it to cover a greater spectrum beyond yes or no. A single distracting phrase “uh” is different than every sentence punctuated by an “uhm,” and a 5-minute case presentation does not have the same consequence as a 14-minute case presentation. Therefore, the scale was modified to 0-3, rather than 0-1. Likewise, to assign greater emphasis to the act of speaking and the presentation rather than simply to the content, we added items to reflect the CDIM members' and other clinical educator recommendations.
CONCLUSION
Spoken communication is critical in the practice of medicine. In the traditional model of instruction, teaching this skill requires a large amount of time or is variably experiential. This innovation in medical education has multiple benefits compared to traditional education. First, it will attempt to assess whether faculty are needed to evaluate and grade students or whether students are capable of adequate peer evaluation. Second, this course will teach and evaluate a skill with a true-to-life evaluation; the evaluation does not focus on whether a task is performed but on how well it is performed. Third, it will assess whether traditional experience (presenting on the wards) can be augmented simply by reviewing peers, thereby alleviating a significant faculty time burden.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care and Medical Knowledge.
ACKNOWLEDGMENTS
Dr Dustyn Williams is the clerkship director in internal medicine for the Tulane University School of Medicine campus in Baton Rouge, LA, and founder of the online video-based education company OnlineMedEd. Dr Shravani Surakanti is an internal medicine resident at Baton Rouge General Medical Center.
- © Academic Division of Ochsner Clinic Foundation
REFERENCES
In this issue








{kind=link}
{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.