
Abstract
Background: In 2012, the Scottsdale Osborn Medical Center intensive care unit (ICU) had a rate of catheter-associated urinary tract infection (CAUTI) among the highest in Arizona hospitals, with 54 infections reported. To address the high rate of CAUTI in the Osborn campus ICU, the project team participating in the Alliance of Independent Academic Medical Centers (AIAMC) National Initiative IV joined the CAUTI systemwide oversight team in the ambitious goal to eliminate CAUTI from Scottsdale Healthcare.
Methods: The quality improvement project to eliminate CAUTI took place throughout calendar year 2014 at the Osborn campus and involved the AIAMC project team, the CAUTI systemwide oversight team, and support from the Scottsdale Healthcare information technology team. A CAUTI bundle based on current best-practice guidelines for prevention of CAUTI was finalized in January 2014. In addition, the AIAMC project team spearheaded and coordinated 6 initiatives based on current guidelines to attempt to reduce unnecessary urinary catheter use in the hospital system. The initiatives included education, mandatory prompts and reminders in the electronic medical record, daily patient tracking, a resident quality champion, and a urine retention protocol.
Results: Catheter days in the ICU dropped by approximately one-third during the first 2 quarters of 2014 and then appeared to level off. The CAUTI numbers and rate fluctuated in the ICU without much change during 2013 and 2014 but then dropped in 2015. However, the national definition of CAUTI changed in the first quarter of 2015, and the change in definition was estimated to reduce the number of reported CAUTIs in our hospital by 25%-30%. Urinary catheter days in the non-ICU units declined relatively steadily from the last quarter of 2013 through midyear 2015. CAUTI rates were fairly low in this setting during the observed quarters. In the emergency department (ED), both urinary catheter insertions and the insertion rate dropped during 2014. The insertion rate dropped from approximately 4% of all ED patients prior to the initiative to just 1%.
Conclusion: The greatest success of this AIAMC National Initiative IV project was the dramatic and sustained decrease in urinary catheter insertions in the ED. The project also helped achieve an important reduction in urinary catheter days in the target hospital ICU and non-ICU floors and likely helped to reduce CAUTI rates as well. Intensive education efforts involving nurses, residents, attending physicians, and quality improvement staff were crucial elements in the initiative. Tracking patients with urinary catheters and electronic order entry and stop reminders played an important role. Despite progress, much work remains to eliminate CAUTI from the hospital.
INTRODUCTION
Scottsdale Healthcare participated in the Alliance of Independent Academic Medical Centers (AIAMC) National Initiative IV from September 2013 through March 2015. An AIAMC project team was assembled to work towards the National Initiative IV goal to integrate quality improvement and patient safety efforts with graduate medical education (GME). Scottsdale Healthcare had a single 27-resident family medicine residency with a busy inpatient teaching service at the Scottsdale Osborn Medical Center campus during the initiative.
In 2012, the Osborn campus intensive care unit (ICU) had a rate of catheter-associated urinary tract infection (CAUTI) among the highest in Arizona hospitals, with 54 infections reported. CAUTI is the most common form of hospital-associated infection, with an estimated 560,000 cases per year in the United States1 causing more than 13,000 deaths per year.2 In 2009, the Centers for Disease Control and Prevention1 and the Infectious Diseases Society of America3 both updated their guidelines for preventing CAUTI. To address the high rate of CAUTI in the Osborn ICU, Scottsdale Healthcare formed a CAUTI systemwide oversight team. The AIAMC project team joined the effort to lend GME support and collaborate with the systemwide team on the ambitious goal to eliminate CAUTI from Scottsdale Healthcare.
METHODS
The CAUTI quality improvement project took place throughout calendar year 2014 at the Osborn campus. Because no patient-identifiable data were used, the study was exempt from institutional review board oversight. Project participants were the AIAMC project team and the CAUTI systemwide oversight team, with support from the Scottsdale Healthcare information technology team.
The family medicine residency associate director chaired the AIAMC team that included the family medicine residency director, 2 residents, the chief academic officer, the vice president of quality and safety, the chief medical officer, and an academic project coordinator.
The AIAMC team worked with the CAUTI systemwide oversight team and in January 2014 finalized a CAUTI bundle based on current best-practice guidelines for the prevention of CAUTI.3 The bundle listed indications for urinary catheters, stressed sterile insertion and appropriate catheter care for patients who required a urinary catheter, and introduced the StatLock device to secure catheters and prevent unwanted movement. The teams also worked to obtain wicking pads as an alternative to a urinary catheter to measure urine output in incontinent patients who could not cooperate. Wicking pads were introduced in the ICU in March 2014.
In addition, throughout 2014, the AIAMC team spearheaded and coordinated a number of initiatives based on current guidelines1,3,4 to reduce unnecessary urinary catheter use in the hospital system:
1. Continuing medical education: A multidisciplinary continuing medical education conference addressing CAUTI prevention was presented in January 2014 as a kickoff event. Conference attendees included residents, nurses, attending physicians, and quality improvement staff. A sentinel event patient case was presented along with information regarding CAUTI, indications for urinary catheters, and strategies to reduce catheter use.
2. Emergency department (ED) initiative: In January 2014, intensive nursing and physician education aimed at reducing urinary catheter use was started in the ED, spearheaded by Chris Marcuzzo, MD. In March 2014, the Picis electronic medical record (EMR) used in the ED was modified to create a mandatory drop-down selection box listing the appropriate indications for urinary catheter placement. The ordering provider had to select one of the indications from the drop-down menu before she/he could continue with the urinary catheter order.5
3. Patient tracking: In April 2014, daily tracking of patients who had urinary catheters was added to the nursing staff daily management system. Numbers were posted on a tracking board in each ward and updated daily. At the same time, the resident teaching service began to track on the daily patient census which patients had urinary catheters and the indications for use.
4. Resident quality champion: One of the residents on the AIAMC team was appointed as the inaugural resident quality champion in July 2014. This newly created position continued with the appointment of a second-year resident when the previous quality champion graduated. The resident quality champion sits on the systemwide Quality Resource Management Committee, coordinates multidisciplinary continuing medical education conferences, and coordinates patient safety case presentations at monthly resident-faculty meetings.
5. Electronic stop orders: An EMR initiative was implemented in August 2014 in the ICU and on the medical and surgical floors of the hospital. An EMR prompt reminded physicians each day when a patient had a urinary catheter in place and asked whether the catheter could be removed. If the physician clicked no, the system asked for the indication for continued use.6,7
6. Urine retention protocol: Based on best-practice guidelines,8 a urine retention protocol was created for use after urinary catheter removal to reduce the rate of reinsertion. The CAUTI systemwide oversight team approved the protocol in August 2014, and it was added to the hospital EMR as a nursing protocol in November 2014.
RESULTS
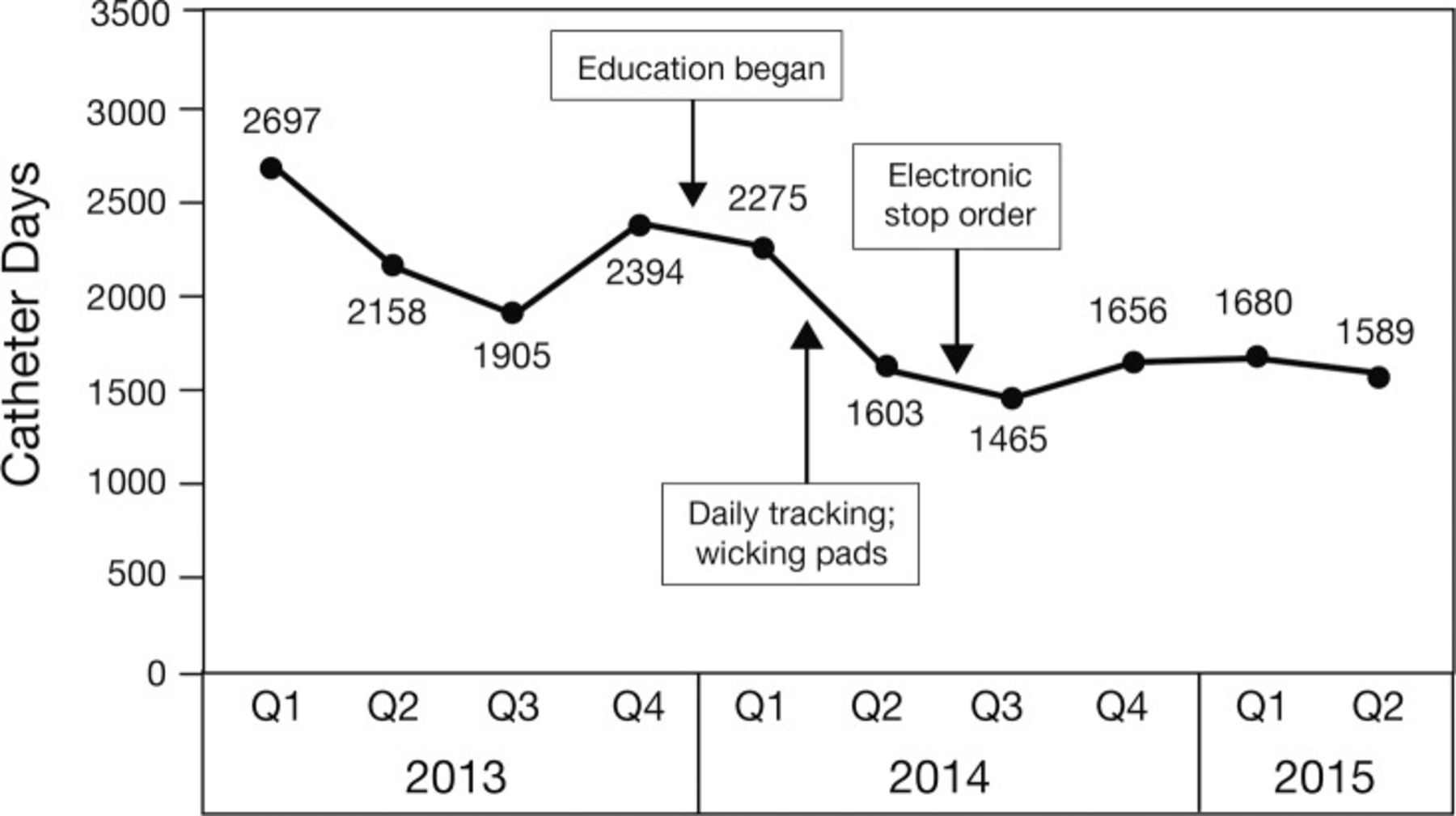
The Osborn campus ICU has tracked the urinary catheter days and CAUTI numbers in each quarter for several years. Each day a patient has a urinary catheter in place counts as one urinary catheter day. The total number of urinary catheter days for each quarter in the Osborn ICU from the start of 2013 until midyear 2015 is reported in Figure 1, along with the timing of the initiative interventions. Catheter days in the ICU dropped by approximately one-third during the first 2 quarters of 2014 and then appeared to level off.

Catheter days per quarter in the Scottsdale Osborn Medical Center intensive care unit. Q, quarter.
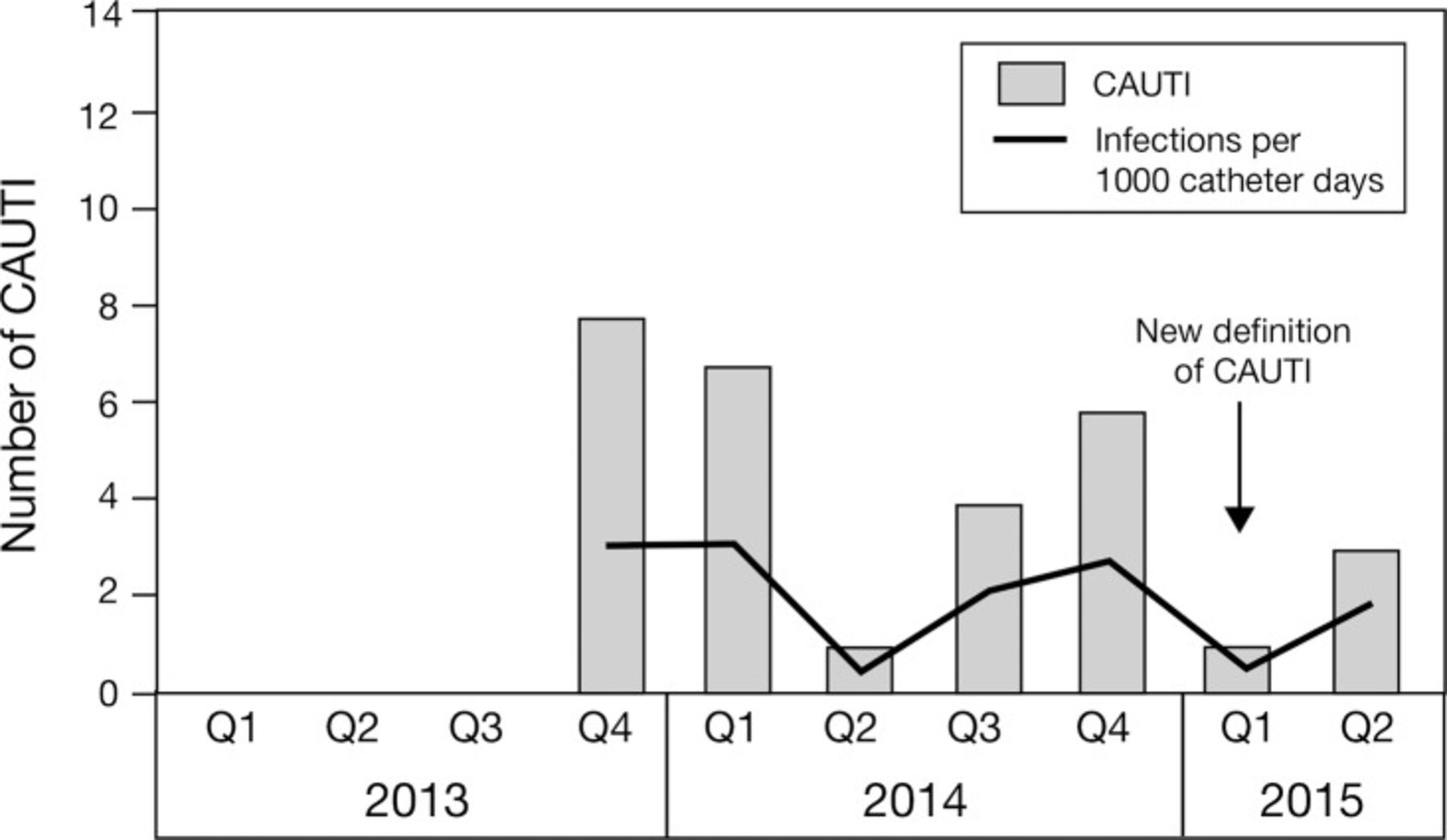
The total numbers of CAUTIs and the calculated CAUTI rate (CAUTI per 1,000 urinary catheter days) for the same period in the Osborn ICU are reported in Figure 2. The CAUTI numbers and rate fluctuated in the ICU without much change during 2013 and 2014 but then dropped in 2015. Of note, the national definition of CAUTI changed in the first quarter of 2015.9 The new definition removed nonbacterial pathogens, increased the colony count to 100,000 bacteria, and limited CAUTI to one in each 14 days in a given patient. This change in definition was estimated to reduce the number of reported CAUTIs in our hospital by 25%-30%.

Catheter-associated urinary tract infection (CAUTI) in the Scottsdale Osborn Medical Center intensive care unit. Q, quarter.
The Osborn campus began tracking urinary catheter days and CAUTI numbers in non-ICU units during the fourth quarter of 2013. Consequently, historic data prior to this CAUTI initiative are not available for comparison. The total number of urinary catheter days for each quarter from the last quarter of 2013 through midyear 2015 for the non-ICU units at Osborn is reported in Figure 3, along with the timing of the CAUTI initiative interventions. As shown on the figure, urinary catheter days in the non-ICU units declined relatively steadily during this time. The total number of CAUTIs and the calculated CAUTI rates for the same period for the non-ICU units are reported in Figure 4, again with the caveat that the definition of CAUTI changed in 2015. CAUTI rates were fairly low in this setting during the observed quarters.

Catheter days per quarter in the Scottsdale Osborn Medical Center non-intensive care units. Q, quarter.

Catheter-associated urinary tract infection (CAUTI) in the Scottsdale Osborn Medical Center non-intensive care units. Q, quarter.
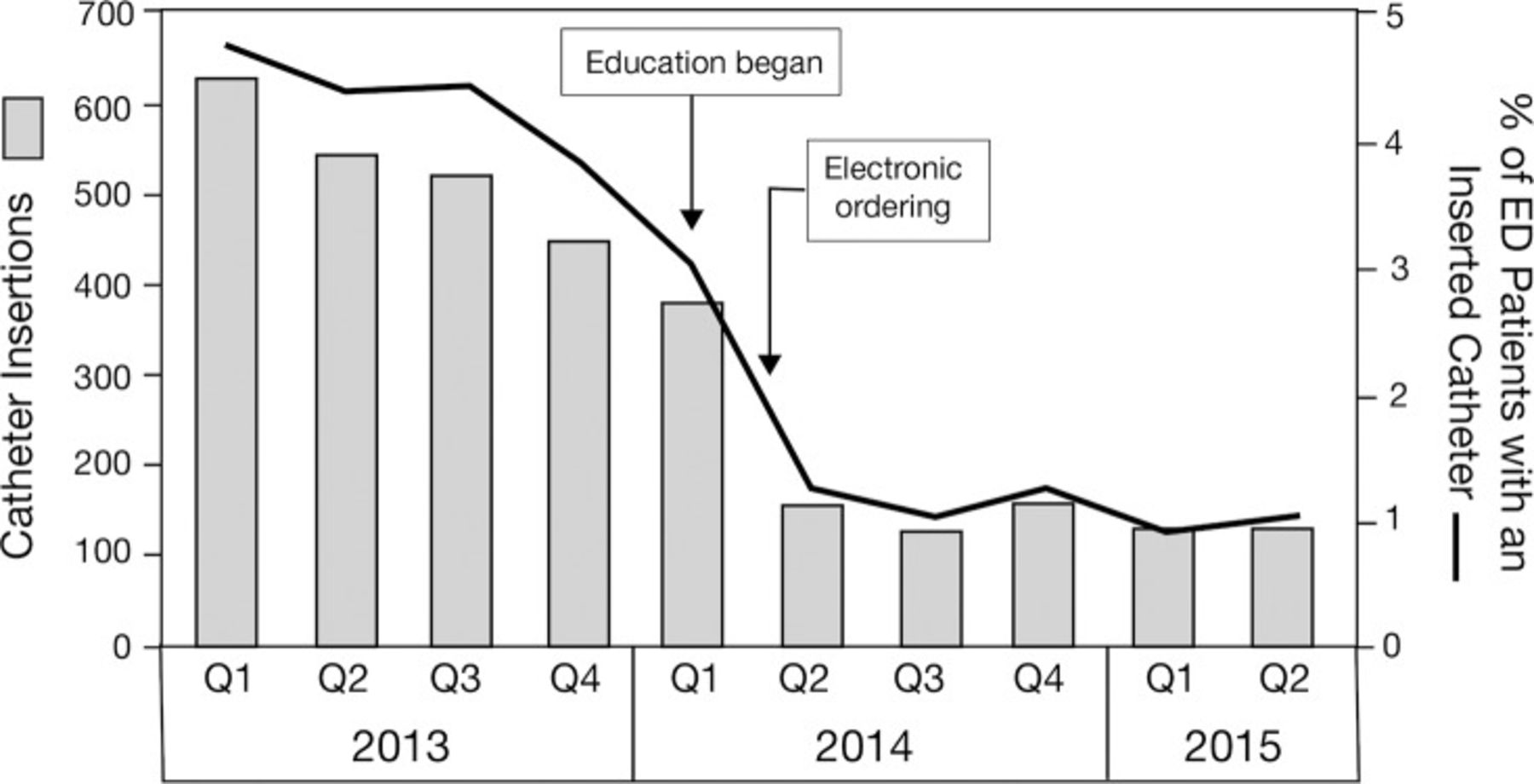
Data regarding urinary catheter insertions in the Osborn campus ED were obtained from Picis, the EMR used to document ED visits. A separate charting system is used for Level I trauma patients, so these patients were not included in this analysis. Total non-Level I trauma visit numbers were obtained for each quarter and used to calculate the rate of urinary catheter insertion per ED patient. The total number of urinary catheters inserted in the ED in non-Level I trauma patients per quarter from 2013 through midyear 2015 is shown by the bars in Figure 5. The line on the graph in Figure 5 represents the rate of urinary catheter insertion as the percentage of patients. The timing of the ED CAUTI initiative interventions is also shown. In the ED, both urinary catheter insertions and the insertion rate dropped during 2014.
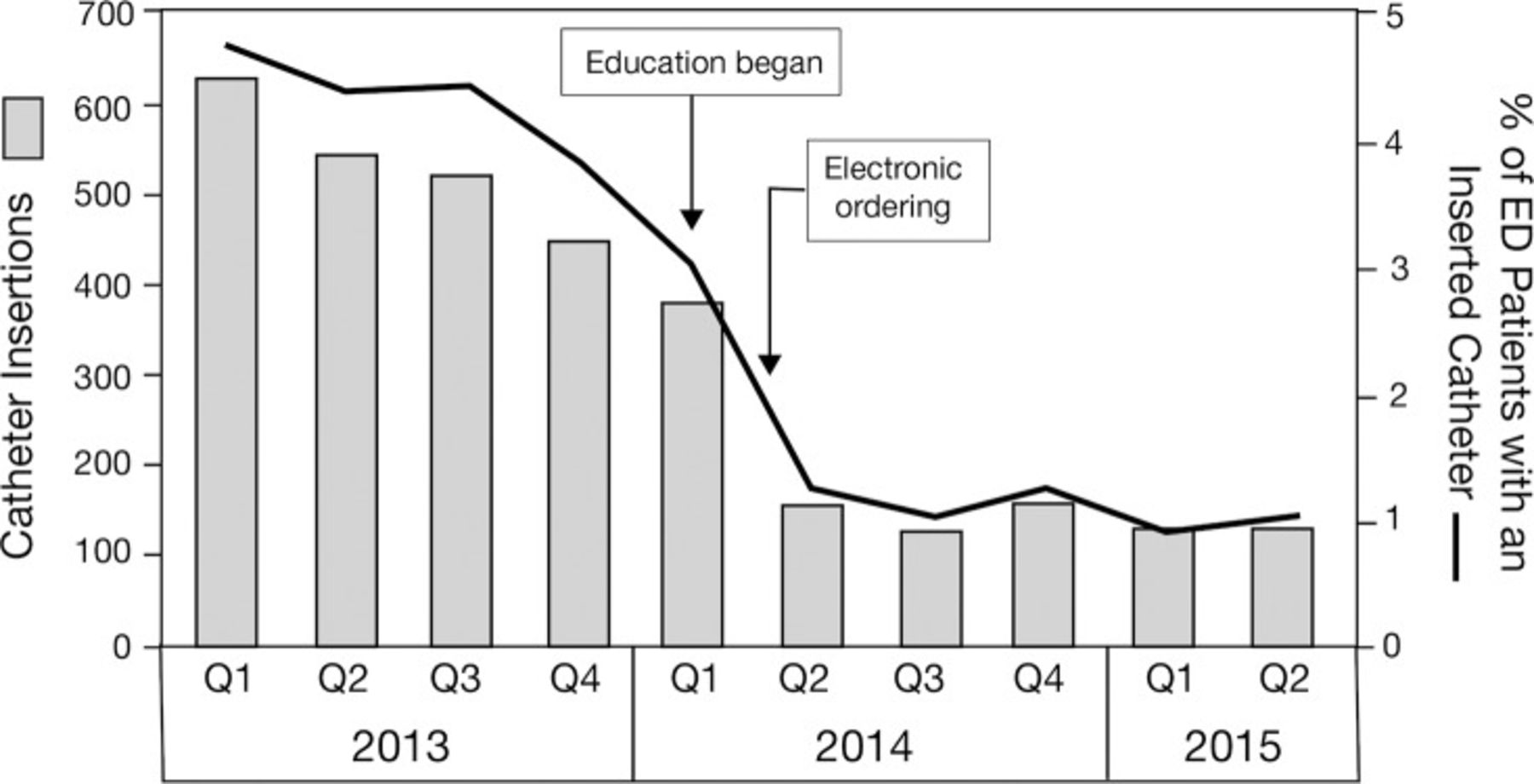
Catheter insertions and rate of insertion in the Scottsdale Osborn Medical Center emergency department (ED). Q, quarter.
Because of the limited number of quarterly data points and the change in the CAUTI definition at the start of 2015, statistical analysis of the data trends could not yield reliable results.
DISCUSSION
Guidelines for CAUTI prevention stress that the most effective and cost-saving measures are to limit the use of urinary catheters to patients who have a clear indication and to remove catheters as soon as they are no longer required.3 The AIAMC team CAUTI initiatives stressed education for nurses, physicians, and residents regarding the indications for urinary catheters and the risks and harms caused by urinary catheters in an effort to prevent their unnecessary use. Education efforts for personnel in the ICU, on the non-ICU floors, and in the ED began in January 2014.
The literature suggests that systems-based interventions such as electronic prompts to ask for an indication prior to insertion and electronic reminders to remove the urinary catheter as soon as possible are effective ways to reduce CAUTI.4-7 The AIAMC team successfully implemented electronic reminders in the ED in March 2014 and in the hospital in August 2014. Using the EMR to make nurses and physicians more aware of the patients who had urinary catheters led to earlier removal and helped to prevent CAUTI.1,3,8 The daily tracking of patients in the hospital who had urinary catheters that was implemented in April 2014 also helped raise awareness among nurses, physicians, and residents. The final strategy—to offer wicking pads as an alternative to urinary catheters and to develop a urine retention protocol to help prevent reinsertion—was not as successful as the other initiatives. Adoption of wicking pads was slow and inconsistent, and the urine retention protocol was delayed until November 2014 because of the numerous committees that had to approve it.
The combination of education, electronic reminders, and daily tracking appeared to reduce the number of urinary catheter days by approximately one-third during the initiative. Unfortunately, CAUTI rates did not decrease much during 2014. The AIAMC team members believe that some nurse and physician champions assisted with the progress of the initiative, but longstanding practices were difficult to change. The early vision of a urinary catheter-free ICU with wide adoption of wicking pads failed to materialize. Both nurses and physicians showed some resistance, and wicking pads are far more labor intensive than a urinary catheter in a critically ill patient. We were encouraged that the CAUTI rate dropped dramatically in 2015, but we do not know how much of the drop might be attributed to the new, stricter definition of CAUTI.
Unfortunately, historic data on urinary catheter days and CAUTI were not available for non-ICU units in the Osborn hospital; however, data collected since the start of the initiative showed a steady reduction in urinary catheter days of nearly 40% during the 7 quarters. CAUTI rates fluctuated but were fairly low throughout the intervention period. On the floors, nurses felt that the daily tracking raised awareness and was a key factor in reducing urinary catheter use. Another key factor was that fewer patients arrived on the floors from the ED with a urinary catheter in place.
Because the CAUTI rates remained constant during most of the initiative, the CAUTI bundle—including sterile insertion, catheter care, and use of the StatLock device—does not appear to have been effective. Of note, a randomized controlled trial of use of the StatLock device failed to find a reduction in CAUTI.10
The greatest success of this project was the dramatic and sustained drop in urinary catheter insertions and insertion rates in the ED that was achieved by the second quarter of 2014. Although insertion rates had started to fall slightly during 2013, ED staff attribute the dramatic drop to the intensive education efforts that started early in 2014. The addition of the mandatory drop-down box in the EMR to choose an indication for a urinary catheter helped to reinforce the behavior change and to keep urinary catheter insertion rates low.
The major culture change that occurred in the ED is widely acknowledged at our institution. The default prior to the initiative was the placement of a nurse-initiated indwelling urinary catheter in virtually every patient who required a urinalysis and could not cooperate or was bedbound. Consequently, a significant number of patients admitted to the hospital through the ED had a urinary catheter. After the CAUTI initiative, patients with a urinary catheter are rarely admitted from the ED. The AIAMC team is very proud that the insertion rate dropped from approximately 4% of all ED patients prior to the initiative to just 1% at the end of the CAUTI initiative.
CONCLUSION
Guidelines suggest that reducing urinary catheter days appears to be the key to prevention of CAUTI. The greatest success of this AIAMC National Initiative project was a dramatic and sustained decrease in urinary catheter insertions in the ED. The project also helped achieve an important reduction in urinary catheter days in the target hospital ICU and non-ICU floors and likely helped to reduce CAUTI rates as well. Intensive education efforts involving nurses, residents, attending physicians, and quality improvement staff were crucial elements in the initiative. Tracking patients with urinary catheters and electronic order entry and stop reminders played an important role. Adoption of alternatives to urinary catheters such as wicking pads was limited. Despite progress, much work remains to eliminate CAUTI entirely. Culture change is difficult and takes time, but the involvement of resident, physician, and nurse champions is helpful. The creation of a resident quality champion position will help ensure resident involvement in ongoing quality improvement initiatives in the system.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care, Medical Knowledge, Professionalism, and Systems-Based Practice.
ACKNOWLEDGMENTS
The authors have no financial or proprietary interest in the subject matter of this article. Dr Greg Alaestante presented a summary of this project as a poster at the Alliance of Independent Academic Medical Centers national meeting in March 2015 in New Orleans, LA. The poster and project description form were published in the proceedings of the National Initiative IV binder and in the Spring 2016 Ochsner Journal special issue Proceedings of National Initiative IV.
The authors would like to acknowledge Patricia Gray, network manager for patient safety and infection control, for her invaluable help with data collection and the initiative and Chris Marcuzzo, MD for his role in spearheading the emergency department initiative.
- © Academic Division of Ochsner Clinic Foundation
In this issue








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.