
Abstract
Background: Inadequate patient adherence to a medication regimen is a major factor in the lack of success in treating hyperlipidemia. Improved adherence rates may result in significantly improved cardiovascular outcomes in populations treated with lipid-lowering therapy. The purpose of this metaanalysis was to evaluate the effectiveness of interventions aimed at improving adherence to lipid-lowering drugs, focusing on measures of adherence and clinical outcomes.
Methods: We searched the Cochrane Central Register of Controlled Trials, MEDLINE, EMBASE, PsycINFO, and the Cumulative Index to Nursing and Allied Health Literature databases through January 14, 2015, and also used the results from previous Cochrane reviews of this title. Randomized controlled trials of adherence-enhancing interventions for lipid-lowering medication in adults in an ambulatory setting with measurable outcomes were evaluated with criteria outlined by the Cochrane Handbook for Systematic Reviews of Interventions.
Results: Twenty-seven studies randomly assigning 899,068 participants to a variety of interventions were analyzed. One group of interventions categorized as intensified patient care showed significant improvement in adherence rates when compared to usual care (odds ratio 1.93; 95% confidence interval [CI] 1.29-2.88). Additionally, after <6 months of follow-up, total cholesterol decreased by a mean of 17.15 mg/dL (95% CI 1.17-33.14), while after >6 months total cholesterol decreased by a mean of 17.57 mg/dL (95% CI 14.95-20.19).
Conclusion: Healthcare systems that can implement team-based intensified patient care interventions, such as electronic reminders, pharmacist-led interventions, and healthcare professional education of patients, may be successful in improving adherence rates to lipid-lowering medicines.
INTRODUCTION
Lipid-lowering therapy has long been an underutilized therapy to lower cardiovascular risk despite compelling evidence of the effectiveness of this therapy.1 Recent recommendations by the American College of Cardiology/American Heart Association are expected to significantly increase the number of individuals for whom statin therapy is indicated.2 Poor adherence rates have been shown to be important factors in inadequate treatment of hyperlipidemia as well as in worse outcomes regarding recurrent myocardial infarction.3-6 A metaanalysis confirmed an approximately linear relationship between the absolute reduction in low-density lipoprotein (LDL) cholesterol and the proportional reductions in the incidence of coronary and major vascular events.7 Statin therapy resulted in a 19% proportional reduction in coronary heart disease death per mmol/L LDL cholesterol reduction. A study in England estimated that 7,000 myocardial infarctions and 2,500 strokes could be avoided each year if high-risk individuals received lipid-lowering treatment.8 These figures show the impact of lipid-lowering drugs on public health and thus the importance of the public's acceptance of and adherence to these medications.
Adherence can be defined as the degree to which patients take medication as prescribed. Adherence can either be intentional or nonintentional. Many factors can influence adherence rates, including adverse effects, denial, inadequate knowledge regarding therapy, memory disturbances, and unreceptive attitudes to treatment. No reliable indicators of adherence exist, and demographic factors such as age, sex, or social class are poor predictors of adherence.9 Therapies for asymptomatic conditions such as hyperlipidemia can be particularly challenging to both the doctor and the patient. Adherence rates in hyperlipidemia trials range from 37%-80%, depending on factors such as study population, background morbidity, classes of drugs, duration of follow-up, and adherence-measuring methods.10 Studies indicate that ideal cholesterol levels are achieved in fewer than 50% of people receiving antilipid therapy and that only 1 in 4 patients continues taking medication long term.1,8 Not unexpectedly, primary prevention trials have even higher discontinuation rates than secondary prevention trials, indicating a relationship between adherence and awareness of illness.10 Evidence of this association was present in a geriatric-based study in which 60% of patients prescribed a statin for acute coronary syndrome discontinued treatment within 2 years compared to 75% of those without coronary disease.11
Duration of therapy is also strongly correlated with discontinuation rates in both primary and secondary prevention strategies.1,11 Poor adherence rates are directly correlated with increases in all-cause mortality as well as recurrent myocardial infarction rates in patients being treated for secondary prevention.6 Discovery of effective strategies to improve adherence rates in both primary and secondary prevention of cardiovascular disease has the potential to significantly improve the health of a community.
The purpose of this metaanalysis was to evaluate the effectiveness of interventions to improve adherence to lipid-lowering drugs, focusing on measures of adherence and clinical outcomes. This study was conducted as an update from previous Cochrane reviews published in 2004 and updated in 2010 on this same topic.12,13
METHODS
The review considered randomized controlled trials (RCTs) of parallel group or crossover design that used individual or cluster randomization. The population studied was all adults (older than 18 years) who were prescribed lipid-lowering medication for primary or secondary prevention of cardiovascular disease in ambulatory care settings. Interventions of any type intended to increase adherence to self-administered lipid-lowering medication vs usual care or no intervention were included. Stratification of interventions into groups was performed on pragmatic grounds, as generally accepted categories do not exist. To determine study similarities, a grid was created into which studies were placed with similar interventions and comparators. The authors cataloged all of the various interventions, comparators, and outcome measures. The interventions were grouped into 1 of 7 categories. The most common comparator was that of usual care. Various outcome measures were identified and evaluated for commonalities among the studies. Studies that were found to have both similar interventions and comparators were then further grouped according to similar outcome measures. When not provided, we estimated the SD for the difference between means by using the formula σd=sqrt (σ1 2/n1 + σ2 2/n2).
Primary Outcomes
The primary outcome of adherence to lipid-lowering medical therapy was assessed by 1 of 3 methods:
1. Indirect measures of adherence (eg, pill count, prescription refill rate, electronic monitoring)
2. Subjective measures of adherence (eg, patients' self-reports in diaries, interviews)
3. Direct measures of adherence (tracer substances in blood or urine)
Secondary Outcomes
The following secondary outcomes were also included in the review:
1. Physiologic indicators (eg, total cholesterol)
2. Health outcome indications (eg, quality of life, morbidity, mortality)
3. Adverse effects
4. Implications for costs (impact of intervention on economic outcomes, economic evaluation)
In the literature, physiologic indicators, health outcomes, and adverse effects have been used as proxy measures for adherence. Studies were included only if these indicators were reported in association with adherence outcomes.
Search Methods for Identification of Studies
The 2010 Cochrane update searched the Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library 2008, Issue 1), MEDLINE (January 2000 to March 2008), EMBASE (January 1998 to March 2008), PsycINFO (1972 to March 2008), and the Comprehensive Index to Nursing and Allied Health Literature (CINAHL) (January 1982 to March 2008). CENTRAL incorporates all controlled trials from EMBASE and MEDLINE except in the most recent years. An appropriate RCT filter was used for MEDLINE14 and EMBASE.
In this update, we included the studies analyzed from the previous review that had last been run on March 31, 2008. The search terms were updated and rerun. Some terms were added to increase the sensitivity in the CENTRAL, MEDLINE, and EMBASE searches. The most recent search occurred on January 14, 2015, and included the following databases: CENTRAL Issue 1212 (The Cochrane Library); MEDLINE (OVID) 1946 to January 2015; EMBASE (OVID) 1980 to January 2015; PsycINFO (OVID) 1806 to January 2015; and CINAHL Plus with Full Text 1937 to January 2015. Searching these databases yielded the following numbers of references: CENTRAL 933; MEDLINE 1,921; EMBASE 2,510; PsycINFO 291; and CINAHL 1,130 for a total of 6,785. Limits to entry dates or equivalent were applied to MEDLINE, EMBASE, and PsycINFO to identify only those records that have been added to the databases since the last search. Results were deduplicated. The RCT filters for MEDLINE and EMBASE were updated according to the latest recommendations in the Cochrane Handbook for Systematic Reviews of Interventions. The RCT filters used for PsycINFO and CINAHL are based on the Cochrane RCT filter.15 No language restrictions were applied.
Three review authors (J.P.S., M.D.M., R.U.) selected studies independently by assessing titles and abstracts. Full-text articles of studies with potential relevance were obtained. Following this initial screening, trials were selected independently by applying predetermined inclusion criteria (J.P.S., M.D.M., R.U.). Disagreements were discussed and resolved between the review authors (M.L.vD., R.E.D.). A spreadsheet was used to identify and extract duplicate studies.
Study outcome data were extracted by using a predefined data collection tool that had been developed by one of the authors (M.L.vD.) and piloted on a random sample of 3 studies. The risk-of-bias assessment on all included studies was performed with the latest version of Review Manager v.5.3 (RevMan; The Cochrane Collaboration). Data were extracted by 3 review authors (J.P.S., M.D.M., R.U.) with a second author checking the extracted data for accuracy.
Risk-of-bias assessment was performed by using the Cochrane Collaboration's tool for assessing risk of bias in the Cochrane Handbook for Systematic Reviews of Interventions.15 We assessed the following risk-of-bias categories: selection bias (method of random number generation and the process of allocation concealment); performance and detection bias (blinding of participants, providers, and outcomes assessors); attrition bias (how incomplete data were managed); and reporting bias (if all intended outcomes were reported).
Each of the studies was marked as high risk, low risk, or unclear risk for each of these risk-of-bias categories. We also took into consideration the method used to measure adherence, as some methods are more likely to be biased than others. For instance, medication refill data are likely to measure adherence more objectively than manual pill count, even if outcome assessors are not blinded to group allocation. Judgment of unclear risk was applied to risk assessment for blinding if patient and physician were not blinded or if outcome assessors were not blinded. Judgment of unclear risk was also applied to any risk assessment if information was not provided or if information was insufficient to permit judgment.
For dichotomous data, we reported the results as odds ratios with 95% confidence intervals (CIs). For continuous data, we reported mean difference (MD) with SD of premeasurements and postmeasurements. The unit of analysis in our metaanalysis was the patient. However, if this was not the case, such as in cluster randomized trials, adjustments for clustering in the pooled analysis were planned by following the guidelines in the Cochrane Handbook for Systematic Reviews of Interventions.15 If data for analysis were missing, we attempted to obtain information from authors. If no additional data were provided, we used data only for which results were reported.
We used the data analysis tools in RevMan v.5.3 to assess heterogeneity, indicated in the forest plots measuring treatment effect. Heterogeneity was determined by first assessing the comparability of the included studies in terms of population, setting, and outcomes. Only studies that were sufficiently similar from a clinical perspective were considered for pooling. Statistical heterogeneity was assessed by calculating the I-squared statistic.
Studies were grouped according to the 7 types of interventions that we identified. Pooling of data and metaanalysis were performed where possible. Data were pooled by using a random effects model. Dichotomous outcomes were used for analysis of medication adherence, and continuous outcomes were used for analysis of clinical markers. For the comparison of the intervention of intensified patient care vs usual care, a random effects model was chosen for data pooling owing to substantial heterogeneity (I2>50%) in some analyses, as random effects models include consideration of heterogeneity in the effect estimate. We performed sensitivity analysis for the pooled results by removing the studies that contributed to heterogeneity and comparing the overall outcome estimate.
RESULTS
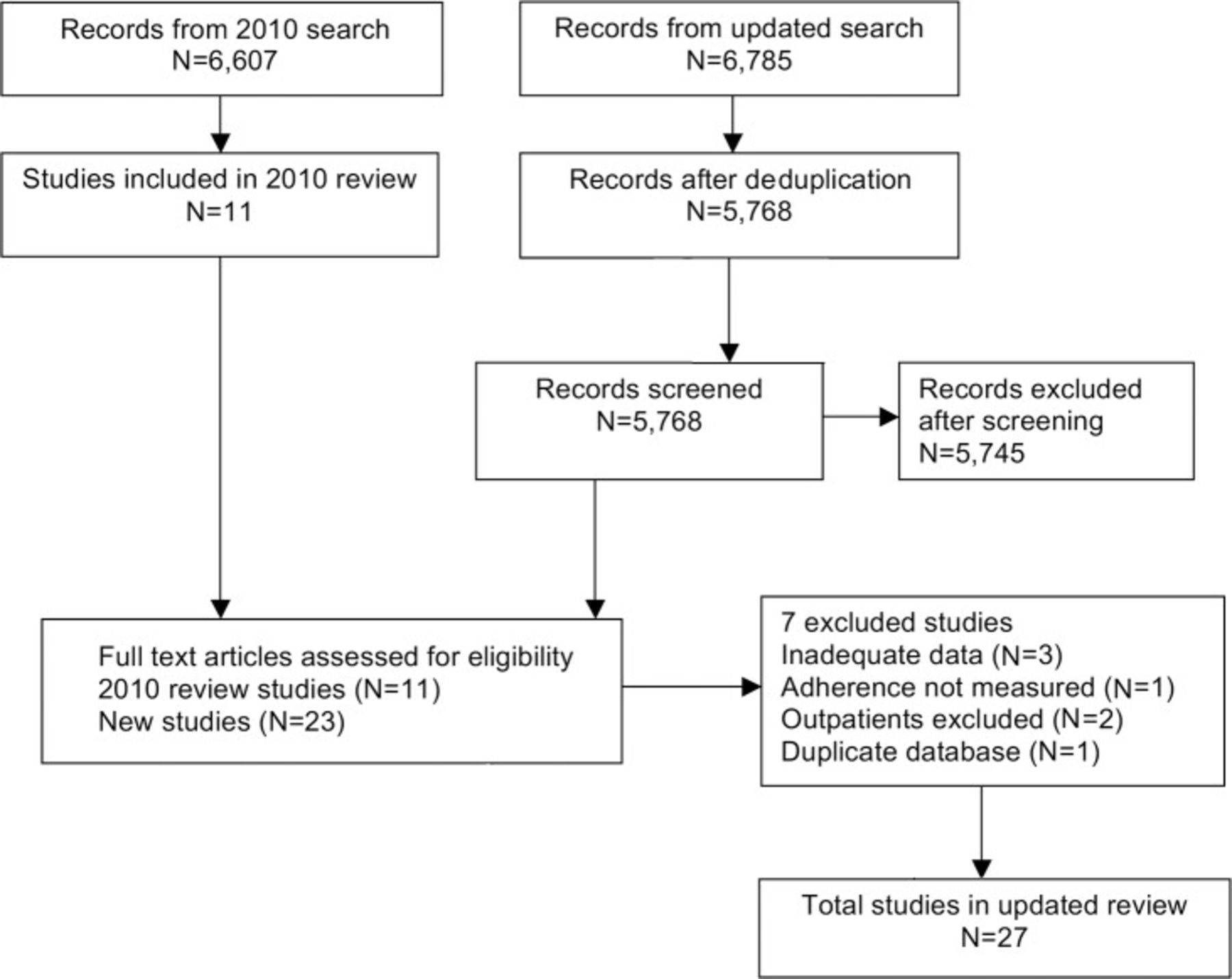
The search in January 2015 retrieved 6,785 articles from all sources. After deduplication, 5,768 titles were reviewed. Of these references, 5,745 studies were excluded by assessing titles and abstracts that did not meet the study criteria for inclusion. Thirty-four full-text articles were retrieved of which 7 studies16-22 were excluded. Sixteen new studies were added to the 2010 review. The 2015 update of this review includes a total of 27 studies. Figure 1 summarizes the results of the literature search.

Summary of search selection.
The study sizes varied from 3023 to 861,89424 with a total number of 899,068 participants included in the full review. Most trials included male and female participants. Two trials included only men.25,26 Mean ages ranged from 49-76.5 years; ages were not reported in 2 studies.27,28 The studies varied greatly in types of participants, setting, medication, interventions used, and outcomes measured.
Interventions
Stratification of interventions into groups was performed on pragmatic grounds, as generally accepted categories do not exist. Seven main groups were identified:
3. Intensified patient care with reminders via mail, telephone, and hand-held pill devices23,26,34-46
5. Decision support systems48
6. Administrative improvements49
7. Large-scale pharmacy-led automated telephone intervention24
The lipid-lowering medications used to treat hyperlipidemia in 23 of 27 trials were statins (3-hydroxy-3-methyl-glutarylcoenzyme A [HMG-CoA] reductase inhibitors).23,24,27-29,31-33,35-49 Fibrates were used in 1 trial.46 Anion-exchange resins or bile acid sequestrants were used in 3 trials.23,26,30 Niacin or nicotinic acid were used in 2 trials.25,26 Two trials used a combined medication regimen,23,25 and 2 trials did not specify a lipid-lowering medication.34,49 There was some overlap among these groups because some studies contained more than 1 lipid-lowering drug among those studied. Drug therapy was most commonly started after study allocation; only 5 studies included patients who were already taking lipid-lowering medication.19,27-29,46 Follow-up times ranged from no follow-up to 24 months. Most studies achieved their endpoint outcomes at 9 months beginning at 3-month intervals. The frequency of intervention varied, ranging from 1 intervention to 12 interventions.
Outcome Measures
The methods used to measure adherence included self-report, the Medication Adherence Report Scale, time to discontinuation, medication possession ratio (MPR), proportion of days covered, continuous multiple interval (CMA), Medication Event Monitoring System (MEMS), drug profile review, prescription refill rate, prescription abandonment, and pill count. Self-report was assessed by asking patients if they had taken their medication as prescribed and how many doses they had missed during a given period. MPR is defined as the number of days on medication after study enrollment divided by the number of days between the first fill and the last refill plus the day's supply of last refill. CMA is defined as the ratio of days' supply obtained to total days between refill records, based on pharmacy records. MEMS is an electronic system of standard pill bottles with microprocessors in the cap that record the timing and frequency of bottle openings, providing detailed and reliable outcome measures at low risk for bias. Drug profile review by a physician on each visit with study participants was used in 1 study.49 Prescription refill rates were based on information obtained from pharmacies. The different methods of measuring adherence were one of the main obstacles in comparing results from the studies, a situation that was further complicated by the fact that some authors used more than 1 method to measure adherence during their trials.
Serum lipids consisting of total cholesterol, high-density lipoprotein, LDL, and triglycerides are physiologic indicators of patient compliance that were the most frequently reported secondary outcomes in 15 of 27 studies.23,25,29-31,33,34,36,39,41-44,46,47 Other reported secondary outcome measures included side effects experienced and self-reported lifestyle measures. None of the studies provided data on morbidity or mortality as additional outcome measures.
Risk-of-Bias Analysis
Ten studies were assessed as unclear risk for random sequence generation because they did not provide sufficient information to make a judgment. The remaining 17 studies were assessed as low risk because they reported using a computer-generated allocation process, telephone allocation, or allocation by a statistician who was not involved in conducting the study.
Twelve studies were assessed as unclear risk for allocation concealment because they did not report sufficient information to allow judgment. The remaining studies were assessed as having a low risk because allocation concealment was adequately described and deemed appropriate.
Regarding bias relating to study blinding, 22 studies were assessed as unclear risk because they had an unblinded, open-label study design or did not report an open-label design. Blinding of those assessing the adherence outcome was not reported in most trials.
One study was classified as high risk for attrition bias owing to a high rate of attrition in the return of a survey tool. Five studies were assessed as unclear risk owing to variable rates of study attrition or not reporting on attrition. Twenty-one studies were assessed as low risk because they reported minimal to no loss to follow-up.
Effects of Interventions
The matrix of comparisons in the included studies is shown in the Table.
Matrix of Interventions and Comparators in Included Studies
1. Drug Regimen Simplification vs Usual Care
.Simplifying the drug regimen was attempted in 4 studies,25,29-31 and no consistent pattern emerged in terms of improving adherence. Owing to dissimilarities in the type of lipid-lowering therapy used as well as in the measured outcomes, pooling of the data from these studies could not be performed.
2. Patient Education and Information vs Usual Care
.Four studies sought to improve medication adherence by improving patient information and education, with no consistent significant improvement found.27,28,32,33 These types of interventions included activities such as pharmacist-mediated information and postal backups; videotapes to members of a health maintenance organization; and a package consisting of an educational leaflet, details of the free phone patient helpline and website, and labels with a reminder to take study medication. However, given the dissimilarity of the outcome measures, pooling of data for these 4 studies was not possible.
3. Intensified Patient Care vs Usual Care
.Intensified patient care was associated with improved adherence in 10 of 15 RCTs, with results from 8 trials reaching statistical significance. A positive and significant trend toward improvement in lipid levels was reported in 2 studies.42,43
Pooling of data for medication adherence at ≤6 months was possible in 7 studies.23,35-38,42,43 Pooling of data for medication adherence at >6 months was also performed in 3 studies.23,39,45
The types of effective interventions in this category included regular phone calls; regular review by a community pharmacist; a simple calendar reminder of medication taking; a pharmaceutical care program; educational counseling at each visit; nurse-led cardiovascular risk-factor counseling; and a multifaceted intervention consisting of pharmacist-led counseling, patient education, teamwork with the patient's primary physician, and voice messaging. Some of the interventions that did not show an effect included telephone and postal reminders; an integrated intervention program (composed of nurse counseling, adherence tip sheet, copay relief card, and the opportunity to enroll in a 12-week cholesterol management program); and a protocol of 5 pharmacist-delivered telephone counseling calls.
Pooling of the Results
We grouped the results into long-term and short-term adherence outcomes. Short-term results were defined as those outcomes measured at ≤6 months, and long-term outcomes were outcomes measured at >6 months. Results were then pooled according to long-term or short-term outcomes.
Medication Adherence at ≤6 Months
Pooling of data for medication adherence at ≤6 months using per-protocol analysis of dichotomous outcomes included 7 studies involving a total of 11,204 participants.23,35-38,42,43 The studies had considerable heterogeneity (I2=88%). Metaanalysis estimated an odds ratio of 1.93 (95% CI 1.29-2.88), favoring the intervention at 95% CI (Figure 2).

Medication Adherence at >6 Months
Pooling of data for medication adherence at >6 months using per-protocol analysis of dichotomous outcomes included 3 studies involving a total of 663 participants.23,39,45 The studies were homogeneous (I2=0%). Metaanalysis using a random effects model estimated an odds ratio of 2.87 (95% CI 1.91-4.29), favoring the intervention at 95% CI (Figure 3).

Reduction in Total Serum Cholesterol (mg/dL) at ≤6 Months
Pooling of data was also possible with studies using total cholesterol and LDL as an outcome. Pooling of data for total serum cholesterol at ≤6 months using per-protocol analysis of continuous outcomes included 4 studies with 430 participants.23,34,42,43 The studies had considerable heterogeneity (I2=89%). Metaanalysis using a random effects model estimated an MD of 17.15 mg/dL (95% CI 1.17-33.14) favoring the intervention (Figure 4), indicating a reduction in total serum cholesterol of 17.15 mg/dL as a result of the intervention. Removing the studies that contributed most to the heterogeneity,42,43 involving a total of 127 participants, from the pooled analysis resulted in an MD of 3.79 mg/dL (95% CI −2.42, 10.00), I2=18%, favoring the intervention but not reaching statistical significance.

Reduction in Total Serum Cholesterol (mg/dL) at >6 Months
Pooling of data for total serum cholesterol at >6 months using per-protocol analysis of continuous outcomes included 2 studies with 127 participants.23,34 The studies were homogenous (I2=0%). Metaanalysis using a random effects model estimated an MD of 17.57 mg/dL (95% CI 14.95-20.19) favoring the intervention (Figure 5), indicating a statistically significant reduction in total serum cholesterol of 17.57 mg/dL.

Reduction in LDL Cholesterol (mg/dL) at ≤6 Months
Pooling of data for LDL cholesterol at ≤6 months using per-protocol analysis of continuous outcomes included 3 studies with 333 participants.23,42,43 The studies had moderate heterogeneity (I2=53%). Metaanalysis using a random effects model estimated an MD of 19.51 mg/dL (95% CI 8.51-30.51) favoring the intervention (Figure 6), once again indicating a statistically significant reduction in LDL cholesterol of 19.51 mg/dL. Removing the studies that contributed to the heterogeneity,42,43 involving a total of 30 participants, from the pooled analysis resulted in an MD of 9.00 mg/dL (95% CI −3.57, 21.57), favoring the intervention but not reaching statistical significance.

Only 1 trial was present in each of the following categories and accordingly, pooling of data from multiple studies was therefore not possible: complex behavioral approaches47 vs usual care; decision support systems48 vs complex behavioral approaches; administrative improvements49 vs usual care; and large-scale pharmacy-led automated telephone intervention24 vs usual care.
DISCUSSION
This systematic review identified new evidence to suggest that patient interventions, which we grouped as intensified patient care, may improve patient adherence to lipid-lowering therapy when compared to usual care. The interventions that were identified to be successful in the intensified patient care group typically involved strategies beyond those that a single clinician could provide. Instead, healthcare delivery systems are best equipped to deliver the types of interventions that have been shown to best improve adherence rates. These interventions involved strategies such as pharmacist-led interventions,36,45 multidisciplinary educational or counseling sessions,40,44 and automated reminders of various types.23,35 A combination of all of these types of interventions, along with an added focus of teamwork with the primary physician, also proved to be effective.39 The interventions appeared to be effective in improving medication adherence both over the short term (<6 months) and the long term (>6 months). Physiologic outcome data in the form of cholesterol levels also demonstrated significant improvement over short-term and long-term periods. Other types of interventions, which were grouped as drug regimen simplification, complex behavioral approaches, decision support systems, administrative improvements, and a large-scale pharmacy-led automated telephone intervention, did not consistently show an overall improvement in adherence rates or other physiologic measures of adherence. Some outcomes were not measured in all studies, and comparisons were made only where possible.
The significant increase in research activity in this field has yielded more robust data from which to derive conclusions. The types of studies in the intensified patient care intervention category included large groups of outpatients and would seem to be generalizable to other outpatient cohorts. Studies in the other intervention categories addressed the objectives of our metaanalysis; however, given the relatively small number of comparable studies with similar interventions and outcome measures, no clear trends emerged. The interventions in the intensified patient care intervention category are applicable in current practice. Many large healthcare systems are evaluating methods to improve the health of large populations of patients. Large-scale structural interventions such as those noted in the intensified patient care group of interventions are generally feasible for these types of systems.
Exploration of additional patient factors that influence adherence to drug therapy may help in identifying other targets for interventions. Other potential areas of research to explore include factors such as patient knowledge, health beliefs, risk perception, memory, side effects of medication, medication costs, and patient inconvenience.50 The phenomenon of adherence is complex, and it seems reasonable for interventions to address this complexity with a patient-centered approach. Consideration of patient beliefs and preferences should be acknowledged and incorporated into adherence-enhancing interventions.51 An important consideration for future studies should include the development of improved methods for measuring adherence. Long-term follow-up of 12 months and more will also help to reveal a more realistic picture of adherence to lifelong treatment and allow for the evaluation of morbidity and costs. Finally, studies evaluating these types of interventions on other outcomes such as morbidity, mortality, quality of life, and cost-effectiveness would be very useful.
The interventions in this metaanalysis were carefully examined for methodologic flaws given the unclear risk of bias inherent to the protocols of a number of selected studies. Multiple independent authors reviewed data at various checkpoints, ensuring the selection of a series of rigorous studies. The authors assessed that systematic error did not threaten the validity of the results in this review. We have searched extensively in several different databases and hand-searched reference lists to identify eligible studies. In addition, 2 authors selected studies independently, thus minimizing the risk of overlooking any relevant study. It is nevertheless still possible that we missed relevant ones.
CONCLUSION
Given the importance of lipid-lowering therapy in both primary and secondary prevention, strategies to improve adherence rates for these potentially life-saving therapies should have significant benefit in patients for whom this therapy is recommended. In this metaanalysis, the effectiveness of interventions identified as intensified patient care was generally demonstrated by improvements in both adherence rates and in lipid levels. The effect appeared durable and was significant over both short-term and long-term periods. Healthcare systems that are able to involve teams of these healthcare professionals in implementing such interventions may well be successful in decreasing the burden of cardiovascular disease in the populations whom they serve with improved adherence to lipid-lowering medications.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care, Medical Knowledge, and Systems-Based Practice.
ACKNOWLEDGMENTS
The authors have no financial or proprietary interest in the subject matter of this article. The authors report no outside funding for this review.
- © Academic Division of Ochsner Clinic Foundation








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}