
Abstract
Background: No consensus on the preferred means of evaluating patients after surgical placement of an inflatable penile prosthesis (IPP) currently exists. Many self-assessment questionnaires are available, but none specifically targets patients with IPPs. The purpose of this study was to assess the construct validity of the Patient Global Impression of Improvement (PGI-I) for evaluating patient satisfaction after placement of an IPP.
Methods: We conducted a multicenter prospective trial and enrolled patients who elected to have a 3-piece IPP surgically implanted. Postoperatively, patients completed the Sexual Health Inventory for Men (SHIM), Erectile Dysfunction Inventory of Treatment Satisfaction (EDITS), and PGI-I at 3, 6, and 12 months. The Pearson correlation coefficient (PCC) was used to compare scores over time.
Results: Fifty-six patients were enrolled, and complete data were available for 39 patients. At 3 months, the PGI-I correlated with the EDITS (PCC=0.83, P<0.01) and with the SHIM (PCC=0.73, P<0.01). At 6 months, the PGI-I correlated with the EDITS (PCC=0.74, P<0.01). At 6 months, the PCC between the PGI-I and the SHIM was 0.41 (P<0.05). At 12 months, the PCC between the PGI-I and the EDITS was 0.83 (P<0.01), and the PCC between the PGI-I and the SHIM was 0.61 (P<0.01).
Conclusions: Overall, the PGI-I appears to correlate with both the SHIM and EDITS and is a valid evaluation tool for use with patients after IPP placement.
INTRODUCTION
The inflatable penile prosthesis (IPP) has been used since 1973. Contemporary satisfaction studies using variable definitions and endpoints of satisfaction report rates between 69% and 98%.1 However, many studies evaluating satisfaction do not use a validated questionnaire, and no consensus exists on the preferred validated questionnaire. Additionally, the results of some of these studies seem to draw conclusions despite the fact that these questionnaires do not specifically address whether patients achieve a global sense of satisfaction; instead, the studies draw this important conclusion by indirect measures such as physician perception of outcome.
Although many self-assessment questionnaires exist, none specifically targets patients who have undergone placement of an IPP. Additionally, these questionnaires are lengthy and time consuming, leading to decreased patient compliance. Simplicity and brevity are important features of patient self-assessment questionnaires.2 Because of these factors, we sought to establish the validity of the Patient Global Impression of Improvement (PGI-I) for use with patients after IPP placement.
The PGI-I is a global assessment tool that has been previously validated for use in evaluating patient satisfaction after urologic therapies, including treatment for lower urinary tract symptoms of benign prostatic hyperplasia, surgical repair of stress urinary incontinence, urogenital prolapse, and male perineal sling placement.3-6 The PGI-I scale was modeled after psychopharmacologic scales developed in 1976 (Clinical Global Impression).7 The Clinical Global Impression-Improvement scale (CGI-I) and the PGI-I both have a 1-question format and use a balanced Likert scale that allows clinicians to assess how much the patient's condition has improved or worsened relative to his or her baseline state. For this study, the PGI-I question was “Please rate your impression of your erectile dysfunction following your implant of a penile prosthesis,” and the response scale ranged from 1-7, with 1 being very much improved and 7 being very much worse. Therefore, lower values correlate with increased satisfaction. To date, the PGI-I has not been used to evaluate satisfaction after IPP placement. By correlating the PGI-I with 2 other established questionnaires in the erectile dysfunction (ED) literature—the Sexual Health Inventory for Men (SHIM) and the Erectile Dysfunction Inventory of Treatment Satisfaction (EDITS)—we sought to establish the construct validity of the PGI-I for use with IPP placement.
METHODS
An institutional review board–approved prospective multicenter trial was performed. Patients who elected to have an inflatable, 3-piece IPP for ED and agreed to participate were eligible for the study. Exclusion criteria included previous IPP placement, infection of the IPP, or sexual inactivity. Patients completed preoperative SHIM and EDITS questionnaires. Patients did not complete the PGI-I questionnaire preoperatively because it is designed to evaluate postoperative satisfaction. Postoperatively, patients were asked to complete the SHIM, EDITS, and PGI-I questionnaires at 3, 6, and 12 months. All questionnaires were completed at scheduled clinic visits with the physician or during telephone or personal interviews with research staff. The SHIM is an easily administered 5-question assessment often used in studies reporting ED severity and commonly reported as an outcome when baseline data are available. SHIM scores are grouped into 4 categories describing the severity of ED: severe (1-7), moderate (8-11), mild to moderate (12-16), and mild (17-21). The EDITS is a validated instrument aimed primarily at determining patient satisfaction in response to treatment.9-11 The EDITS is an 11-item questionnaire in which each question is scored on a scale of 0-4 for a maximum index score of 44.11 The EDITS questionnaire has no standardized severity scoring system, but higher values correlate with higher treatment satisfaction.
The Pearson correlation coefficient (PCC) was used to compare the postoperative EDITS and SHIM scores with the PGI-I at each time period, and the Fischer r to z transformation was used to compare differences in correlation results between device types.
RESULTS
Fifty-six patients were enrolled in the study; 39 men met the inclusion criteria, achieving a statistical power of 90%. Mean patient age was 62.6 years (±11.03). Race composition was 77% white, 18% African American, and 5% other (Table 1). All patients received a 3-piece IPP via a penoscrotal approach; 56% of patients received a Titan (Coloplast Corp.) IPP, and 44% had an AMS 700 CX (Boston Scientific Corporation) device implanted. Of the men excluded from the study, 6 were excluded because of postoperative sexual inactivity, 2 had penile implant infections requiring removal of the device at 3 and 5 weeks postoperatively, and 9 enrollees had insufficient follow-up.
Demographic Data
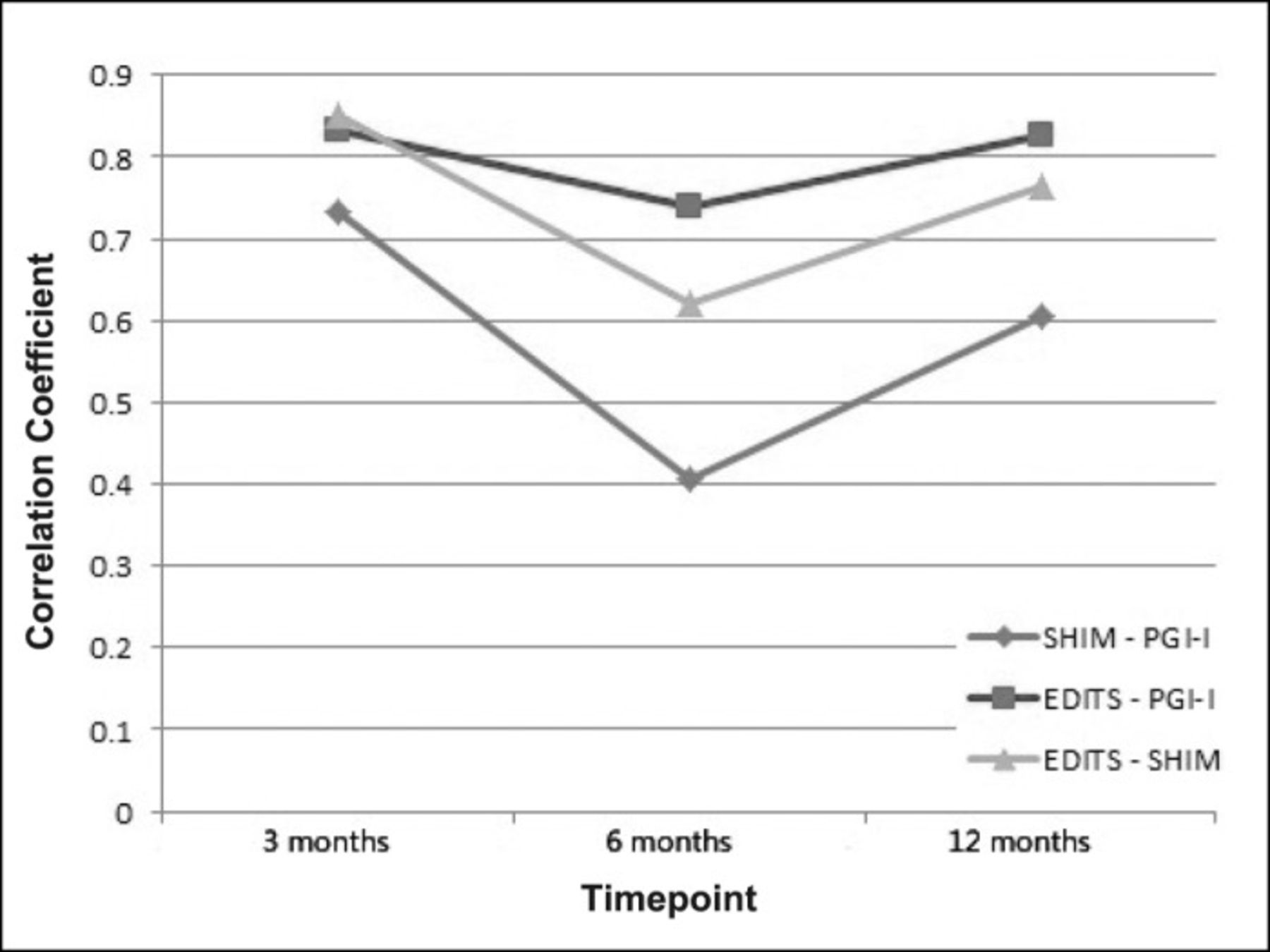
Mean PGI-I, SHIM, and EDITS scores at 3, 6, and 12 months are shown in Table 2. The PGI-I correlated strongly with both the SHIM and EDITS at all time points. At 3 months, the PGI-I correlated with the EDITS (PCC=0.83, P<0.01) and with the SHIM (PCC=0.73, P<0.01). At 6 months, the PGI-I correlated with the EDITS (PCC=0.74, P<0.01) and with the SHIM (PCC=0.41, P<0.05). At 12 months, the PCC between the PGI-I and the EDITS was 0.83 (P<0.01), and the PCC between the PGI-I and the SHIM was 0.61 (P<0.01) (Figure 1). Overall correlations of all data points were 0.76 for the SHIM to the EDITS, 0.62 for the SHIM to the PGI-I, and 0.82 for the PGI-I to the EDITS (P<0.01). Correlations between the clinically accepted questionnaires and the experimental PGI-I were similar, suggesting that use of the PGI-I alone may be clinically effective. Correlations were also performed for each device type, and no significant differences were found between the correlations of AMS vs Titan devices using a Fischer r to z transformation.
Mean Score Progression

The Pearson correlation coefficients for the SHIM vs the PGI-I, the EDITS vs the PGI-I, and the EDITS vs the SHIM at 3 months, 6 months, and 12 months. EDITS, Erectile Dysfunction Inventory of Treatment Satisfaction; PGI-I, Patient Global Impression of Improvement; SHIM, Sexual Health Inventory for Men.
DISCUSSION
Currently, no standardized method exists to measure outcomes of patients after placement of an IPP. Evaluating patients using a patient-reported outcome, a quantitative objective measure, or a patient self-assessment that eliminates physician or reporter bias is preferable.2,8 Our goal was to establish the construct validity of the PGI-I by correlating it to 2 commonly used validated ED questionnaires.
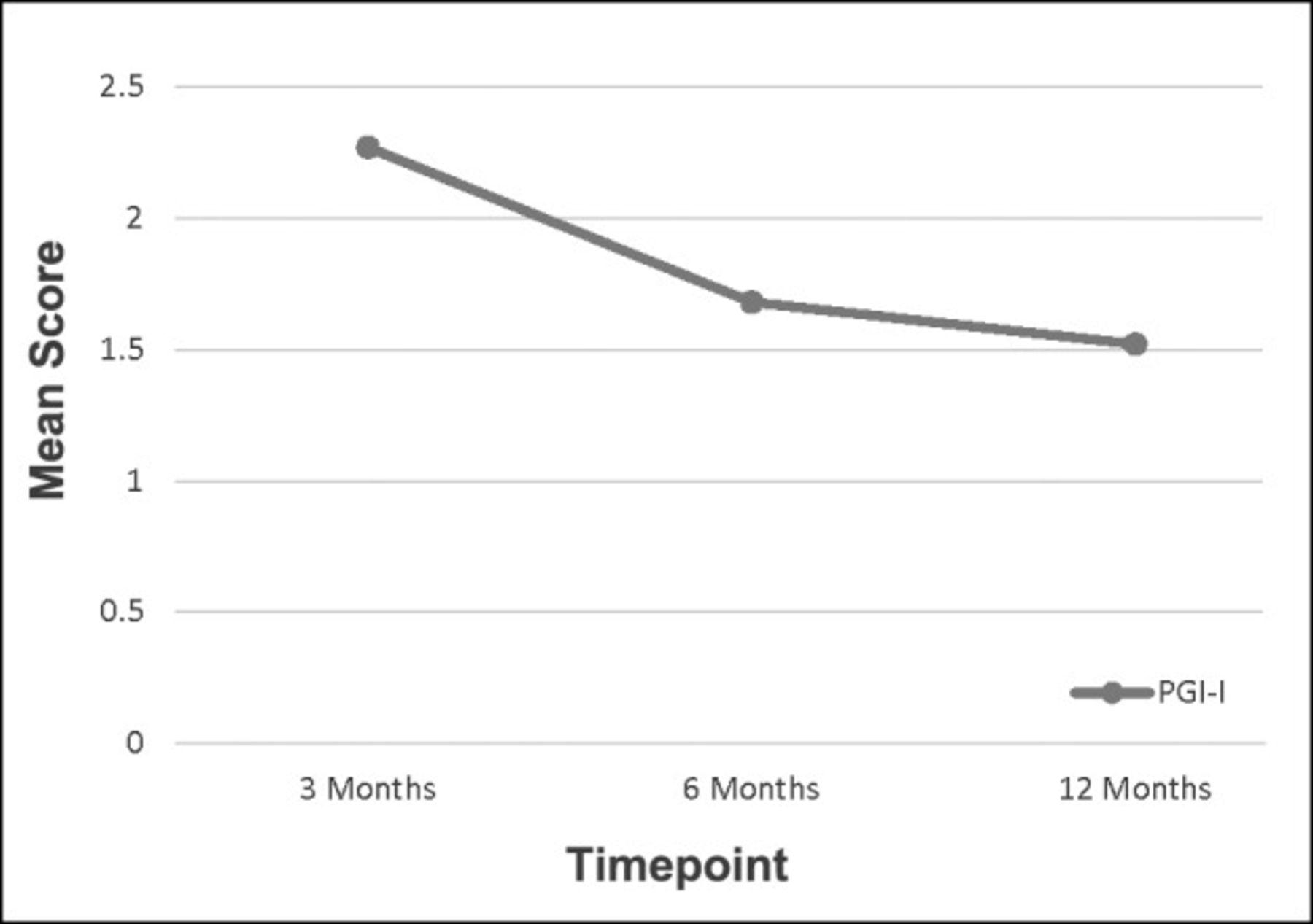
Our data show significant correlation between the commonly used ED questionnaires and the PGI-I. The EDITS, SHIM, and PGI-I show improvement of scores at all 3 data points as the postoperative interval lengthens. Mulhall et al12 showed that the International Index of Erectile Function satisfaction domain and the EDITS scores at 12 months were significantly higher than at 6 months, suggesting that continued satisfaction was achieved as patients passed into the second half of the first postoperative year. We noted a similar pattern: the EDITS and SHIM scores improved from means of 35.7 and 19.3, respectively, at 6 months to means of 37.5 and 20.5, respectively, at 12 months. The PGI-I followed the same trend, and mean scores improved from 1.68 to 1.52 during the same period (Figure 2).

The decrease in Patient Global Impression of Improvement (PGI-I) values with each time interval in the postoperative period correlating with increasing patient satisfaction scores within the first postoperative year.
We decided to exclude men who were not sexually active because both the SHIM and EDITS have questions pertaining to sexually activity. If a patient is not sexually active, the scores from these questionnaires will be misleading. For example, a patient may be very satisfied with his IPP, but if that patient is not sexually active, he will have very low SHIM and EDITS scores. To eliminate this potential for bias, these patients were excluded.
Many prior studies have only used physician assessments to assess satisfaction. In addition to introducing a large component of observer error, such reporting methods are prone to overreport success and minimize negative outcomes. For these reasons, the patient's perspective as evaluated by patient-reported outcomes (PROs) is important in clinical research because treatment efficacy is no longer solely linked to clinical outcomes such as cure, overall survival, or physician impressions. Ailments such as pain, fatigue, acceptance, and social isolation can only be assessed by a patient's direct expression without any interpretation by medical staff. PROs facilitate the disclosure of quality-of-life issues, and patients feel stronger support from improved communication. This is in contrast to the support experienced with a physician or other means of defining outcomes. PROs collected as part of the clinical routine have versatile applications: they can be used for scientific analyses, quality assurance, and health technology assessment.13
We believe this PGI-I will provide advantages to clinicians compared to the questionnaires that are currently available to quantify patient satisfaction with IPPs because it is patient centered and focused on a specific procedure. The International Index of Erectile Function (from which the SHIM was derived), SHIM, and EDITS do not specifically target a patient who has undergone IPP placement. Although the EDITS is commonly used to evaluate satisfaction after a procedure, it was originally designed to evaluate satisfaction after medical therapy for ED. The SHIM and EDITS questionnaires are not specifically designed for a postoperative patient, but they have been used historically with patients undergoing medical and surgical ED treatments. Therefore, we believe the PGI-I is better than these questionnaires because it has a simple 1-question form and is specifically designed for a patient who has undergone surgery.
Limitations of our study include the small sample size, some patients being lost to follow-up, and limitations—such as response bias—that are inherent in any questionnaire-based study.
CONCLUSION
The PGI-I is a 1-question assessment designed to evaluate the patient's impression of improvement since surgery. This brief questionnaire correlates well with traditional methods of sexual function evaluation. The brevity of the PGI-I has the potential to increase patient compliance and improves upon other common questionnaires used to evaluate satisfaction after IPP placement. The PGI-I appears to be a valid self-assessment questionnaire for use after IPP placement.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care, Medical Knowledge, and Practice-Based Learning and Improvement.
ACKNOWLEDGMENTS
The authors have no financial or proprietary interest in the subject matter of this article.
- © Academic Division of Ochsner Clinic Foundation
In this issue








{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.