
Beware of Right Renal Vein Valves in Transplanted Kidneys: Renal Vein Valvuloplasty in a Donor Kidney
To the Editor
Here we present an unusual case of renal vein thrombectomy after renal allograft reperfusion secondary to venous outflow obstruction (VOO). While VOO is an unfortunate complication of kidney transplantation, it is not unforeseen and is chiefly attributable to venous anastomotic issues. However, in this case, we describe donor hilar vein venotomy, thrombolysis, and renal vein valvuloplasty. To our knowledge, this description is the first report of a renal vein valve in kidney transplantation resulting in VOO and the strategy used to remedy this problem.
CASE REPORT
The patient is a 58-year-old male with end-stage renal disease secondary to hypertension and polycystic kidney disease on hemodialysis. The donor was a 34-year-old female with a Kidney Donor Profile Index of 89%, a terminal serum creatinine of 1.4 mg/dL, and an unremarkable biopsy.
The right kidney was selected, and the renal vein was elongated by firing a vascular stapler obliquely from the superior edge of the right renal vein to the inferior edge of the left renal vein orifice. The inferior vena cava (IVC) became the common venous outflow channel, and the bottom portion was anastomosed to the left external iliac artery. Reperfusion after arterial anastomosis was initially uneventful with robust flow noted, but the kidney quickly began to exhibit congestion and edema.
VOO was suspected, and the venous anastomosis was taken down after reclamping the vasculature, but no obvious problem was visualized. Moreover, when the arterial clamp was opened, no venous bleeding was seen, suggesting a problem proximally. Observation of the donor renal vein demonstrated discoloration proximal to the staple line in the renal hilum. A longitudinal venotomy was made at this level, and inexplicably a renal vein valve was noted with fresh clot (Figure). Valvuloplasty and mechanical thrombolysis resulted in immediate venous outflow. The artery was reclamped, and the venotomy was closed transversely. The kidney was reperfused and noted to be normal color with normal arterial and venous waveforms on ultrasound. Notably, 3 months after transplantation, the patient had a serum creatinine value of 1.7 mg/dL.

Forceps on the left are grasping the renal vein valve. K, kidney allograft; *, donor renal vein. Intraoperative photograph taken by John Bosworth, PA.
DISCUSSION
Discussion about renal vein valves has principally been consigned to history; however, awareness of renal vein valves is of utmost importance when managing vasculature related to transplantation. While the relevance of renal vein valves is unclear, early postmortem reports have demonstrated that their presence is not infrequent.1,2 Moreover, venograms have validated their occurrence bilaterally anywhere along the course of the renal vein.3 In our case, it is highly likely that stapling the top portion of the IVC juxtaposed to the renal vein inadvertently entrapped the valve. Consequently, the back-table surgeon must fully interrogate the lumen of the renal vein—especially true when creating an elongated venous outflow conduit for right kidney allografts—to offset the chance occurrence of VOO.
Seizure Caused by Tumor Necrosis Factor-Alpha Inhibitor-Induced Central Nervous System Demyelination
To the Editor
Adverse neurologic events are rare yet concerning complications of tumor necrosis factor-alpha inhibitors (anti-TNF-α) used to treat autoimmune conditions such as rheumatoid arthritis. The most commonly reported adverse neurologic events include peripheral neuropathy followed by central nervous system (CNS) and/or spinal cord demyelination.1 The anti-TNF-α agents most commonly reported in association with these events include etanercept and infliximab.1 Here, we report a patient with rheumatoid arthritis who developed cerebral demyelination while on adalimumab therapy.
CASE REPORT
A 36-year-old female with aggressive, treatment-resistant polyarticular juvenile idiopathic arthritis who was taking multiple medications presented to the emergency department after experiencing what was determined to be 2 back-to-back seizures. At the time of admission, her prescriptions were adalimumab, methotrexate, folic acid, sulindac, prednisone, vitamin D2, quetiapine, mixed amphetamine salts (Adderall), and zoledronic acid (Reclast). She denied any personal or family history of seizures or other neurologic disease except migraine headaches. Her neurologic examination was normal, and laboratory findings did not demonstrate any significant abnormalities to suggest metabolic, toxic, or infectious causes. Magnetic resonance imaging (MRI) of the brain demonstrated numerous white matter lesions on T2-weighted imaging consistent with demyelination. Electroencephalogram did not detect a seizure but documented the presence of sharp wave discharges in the right temporal region. Lumbar puncture was normal. No oligoclonal bands or significant levels of myelin basic protein were detected in her cerebrospinal fluid. Considering her clinical history, laboratory results, and imaging findings, drug-induced cerebral demyelination was suspected, and adalimumab was discontinued. The patient has been seizure-free ever since. Repeat brain MRI 1 year later revealed reduced areas of demyelination, although some new areas of demyelination were present.
DISCUSSION
Demyelination is a rare complication associated with anti-TNF-α therapy; however, the rate of total adverse neurologic events in patients treated with anti-TNF-α has been estimated to be as high as 4%.2 The average lifetime risk of developing demyelinating disease while on anti-TNF-α therapy for psoriasis has been calculated to be 0.1%-1.7%, demonstrating that risk of demyelination may actually range from protective to marginally increased when compared to the general population.3 Mechanisms underlying increased susceptibility to demyelination with anti-TNF-α are not well understood. Some authors have suggested that the nonselective inhibition of TNF can lead to a decrease in certain immunosuppressive effects of TNF signaling,4 while others claim a decrease in antiinflammatory cytokines with a concomitant influx of proinflammatory cytokines is specifically associated with demyelination.5
While several adverse neurologic events have been reported to the US Food and Drug Administration, most are described as possible or probable adverse events. Thus, definitive association between exposure to anti-TNF-α and the development of a neurologic complication cannot not be established.1 Furthermore, neurologic complications can be a direct manifestation of rheumatic disease activity.6,7
In our patient, a definitive causal relationship between the development of CNS demyelinating lesions and anti-TNF-α cannot be determined. Multiple sclerosis (MS) is also a possibility in our patient given the high prevalence of MS as a comorbid condition in patients with rheumatoid arthritis and the potential of anti-TNF-α to unmask preclinical neurologic disease.1,8 However, in this case, the patient has had no neurologic symptoms and has been seizure-free since discontinuing adalimumab.
Positron Emission Tomography-Positive Pleural-Based Nodule Following Talc Pleurodesis
To the Editor
The fluorodeoxyglucose positron emission tomography (FDG-PET) scan is frequently used for evaluation and staging of pulmonary malignancy. False-positive PET results can occur. The most common causes of false-positive PET results include pulmonary-pleural inflammation (such as tuberculosis, sarcoidosis, or rheumatoid nodule) and a PET artifact caused by the FDG containing a blood clot microembolism produced during FDG injection. We describe a case of a PET-positive pleural-based nodule after talc pleurodesis mimicking pleural malignancy and discuss the pathophysiology of reactive pleural inflammation after talc pleurodesis.
CASE REPORT
A 48-year-old female was referred to the pulmonary clinic for evaluation of a pleural-based nodule. She complained of a dull, right-sided chest pain with exertion that spontaneously resolved. She was a previous smoker of 25 pack years and had quit smoking 2 months before this evaluation. The patient had had recurrent episodes of primary spontaneous right-sided pneumothoraces 15 years earlier and underwent right-sided talc pleurodesis. She denied significant occupational exposures or traveling in the past few years. Cardiopulmonary examination was unremarkable. Pulmonary function testing was normal. Computed tomography (CT) of the chest from an outside facility demonstrated nodular pleural thickening 12 × 77 mm in diameter along the lateral aspect of the right major fissure (Figure 1). FDG-PET from an outside facility demonstrated an intensely hypermetabolic nodule with a standardized uptake value of 14.4 (Figure 2). Upon review, a CT chest report that had been done at our facility 10 years prior (no image available) revealed that the size of the patient's lesion had not changed. The diagnosis of reactive inflammation of the pleural-based nodule after talc pleurodesis was established. The patient was treated conservatively without further invasive diagnostic testing.

The computed tomography (CT) scan of the chest from an outside facility demonstrated nodular pleural thickening 12 × 77 mm in diameter along the lateral aspect of the right major fissure. The radiographic appearance and the size of this lesion had not changed compared to a CT chest done 10 years prior.
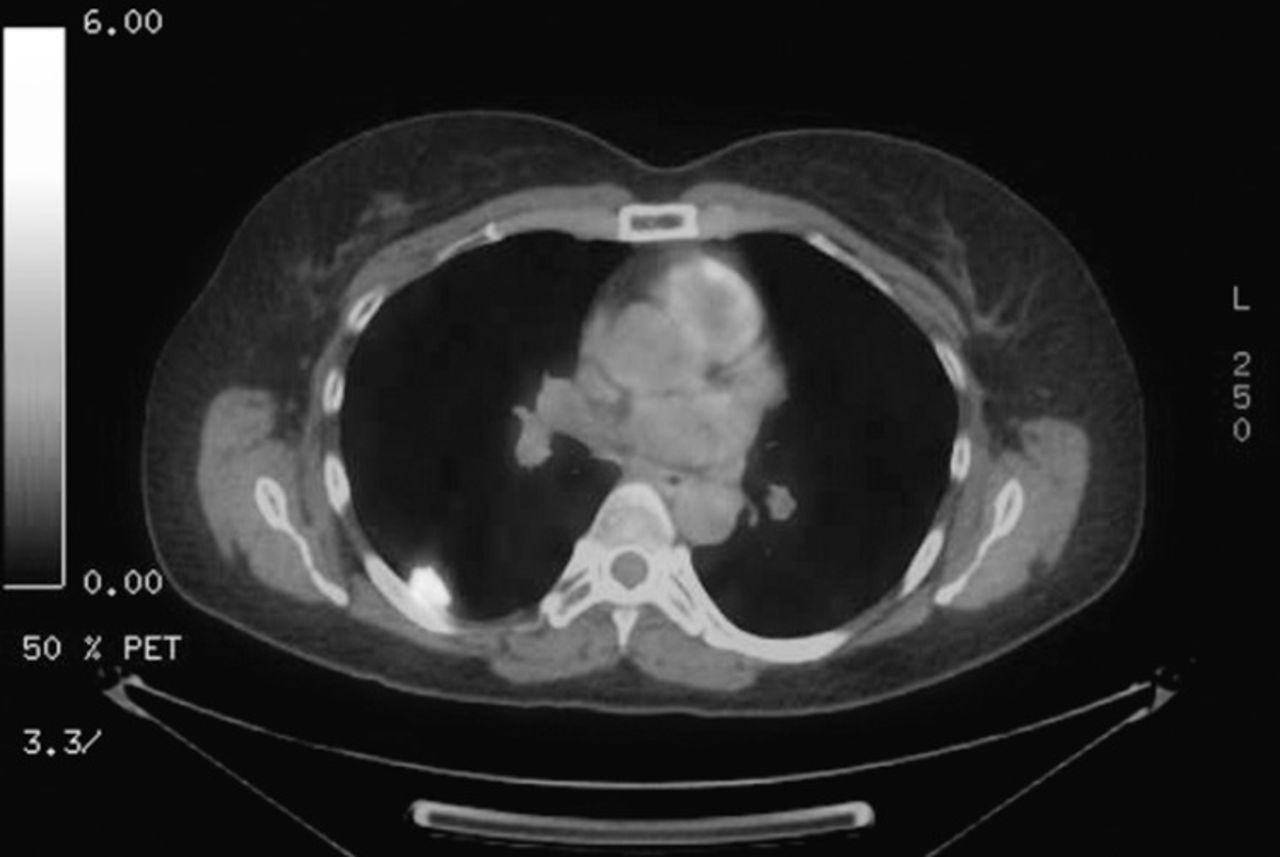
The fluorodeoxyglucose positron emission tomography from an outside facility demonstrated intense hypermetabolic activity corresponding to the right pleural-based nodule on anatomical computed tomography of the chest.
DISCUSSION
Positive FDG-PET pleural nodularity from talc pleurodesis has been reported in the literature.1 Talc pleurodesis induces an inflammatory response that leads to intensive proliferation of fibroblasts in the pleural surface within 3 days of the procedure and subsequently leads to pleural adhesions and a chronic granulomatous reaction.2 An increased FDG uptake within the thickened pleura starts within 5 months after pleurodesis and continues until pleural calcification has developed.3 The inflammatory process decreases with time. Because talc is not metabolized by the body, the FDG-PET scan can remain positive for up to 20 years after the procedure.2 In our case, no radiographic change in size and location of the pleural lesion occurred for 10 years, suggesting benign granulomatous reaction after talc pleurodesis. The PET-positive pleural-based nodule/thickening could be misinterpreted as pleural malignancy. Determining if the patient has a history of pneumothorax requiring talc pleurodesis and reviewing previous chest images are mandatory to avoid unnecessary invasive diagnostic procedures.
- © Academic Division of Ochsner Clinic Foundation
In this issue








{kind=link}
{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.