
INTRODUCTION
Transjugular intrahepatic portosystemic shunt (TIPS) is currently one of the major treatment modalities for complications associated with portal hypertension in patients with cirrhosis.1 The TIPS procedure entails the formation of a low-resistance conduit between the hepatic and portal veins, thereby bypassing the liver parenchyma. One of the major complications associated with TIPS, reported to occur in 15%-30% of TIPS cases,2 is new or worsened hepatic encephalopathy (HE) which can be severely debilitating, with symptoms including confusion, disorientation, lethargy, and frank obtundation. The primary treatment for recurrent HE following TIPS is similar to the treatment provided to any encephalopathic patient and begins with a search for precipitating factors such as infection, electrolyte abnormalities, bleeding, and constipation. Medical treatment with agents such as lactulose and nonabsorbable antibiotics such as rifaximin are usually successful in reversing the problem.3 However, further intervention including shunt reduction or occlusion and organ transplantation is estimated to be required in 3%-7% of patients who continue to suffer from refractory HE.3
We present a case of refractory HE post TIPS revision that was treated with shunt reduction. TIPS revision is a safe and effective procedure for restoring shunt patency if the TIPS becomes occluded. TIPS reduction is a procedure that decreases the diameter of the lumen of the TIPS and subsequently allows less flow through the shunt.
HISTORY
A 61-year-old male undergoing outpatient evaluation for liver transplantation because of nonalcoholic steatohepatitis cirrhosis and symptomatic portal hypertension presented for recurrent debilitating encephalopathy secondary to prior TIPS procedure. His TIPS had been placed at another institution on November 9, 2015. The patient's HE had been managed medically with lactulose and rifaximin.
RADIOGRAPHIC APPEARANCE AND TREATMENT
Hepatic ultrasound with Doppler performed at Ochsner approximately 10 months after original TIPS placement showed the shunt to be patent but with potential dysfunction as evidenced by loss of expected retrograde right portal venous flow (Figure 1).

Ultrasound Doppler with spectral analysis demonstrates loss of expected retrograde flow in the right portal vein.
On September 28, 2016, TIPS evaluation and revision were performed by interventional radiology. A 5-French (Fr) MPV catheter (Merit Medical Systems, Inc.) was used to select the right hepatic vein and a Glidewire was advanced through the shunt. The catheter was placed into the portal vein. Portogram demonstrated shunt patency with adequate direction of flow within the shunt. The stent was dilated using a 10-mm balloon (Figure 2). Final images demonstrated patency of the TIPS shunt and flow of contrast material across the stent. The revision resulted in successful reduction of the portosystemic gradient to approximately 10 mmHg from 13 mmHg (Table).

Fluoroscopic image demonstrates wire extending from the inferior vena cava to the hepatic vein through the transjugular intrahepatic portosystemic shunt (TIPS) into the portal system. The TIPS stent was dilated with a 10-mm balloon, reducing the portosystemic gradient from 13 mmHg to 10 mmHg.
Preprocedure and Postprocedure Pressures
Follow-up ultrasound with Doppler performed on October 18, 2016, showed appropriate flow through the stent. However, the patient developed debilitating encephalopathy post TIPS revision, and the patient was referred for possible TIPS reduction. After discussing the risks of increasing the portosystemic gradient with the patient's family, TIPS reduction was performed on November 4, 2016.
First, two access sites were made within the right jugular vein, and two 0.035 wires were placed into the inferior vena cava. Tandem 6-Fr and 10-Fr sheaths were placed. Two wires were advanced through the TIPS. A pigtail catheter was placed into the portal vein. Images (not shown) demonstrated no stenosis within the shunt, brisk shunting through the TIPS, and the absence of collateral filling within esophageal varices. The initial portosystemic gradient across the TIPS was 12 mmHg. Through the 6-Fr sheath, a 7-mm diameter × 17-mm length balloon-expandable Genesis stent (Boston Scientific) was placed. Through the 10-Fr sheath, a new 10-mm diameter, 2-cm uncovered, 7-cm covered VIATORR stent (Gore Medical) was brought into position within the TIPS. The balloon-expandable stent was expanded in the middle of the covered portion of the existing TIPS, and the VIATORR stent was deployed over the Genesis stent with the balloon inflated. The proximal and distal ends of the TIPS were balloon dilated (Figure 3). The balloon and the wire for the balloon-expandable stent were removed. This procedure resulted in successful reduction of the TIPS with an appropriate increase in the portosystemic gradient to approximately 17 mmHg from 12 mmHg. Postreduction pressures within the portal vein and right atrium are shown in the Table. Final fluoroscopic images demonstrated patency of the TIPS. Figure 4 is a fluoroscopic image from a different patient that illustrates the same TIPS reduction procedure. Follow-up computed tomography demonstrated final Genesis stent positioning (Figure 5). At the 1-week, 1-month, and 3-month follow-ups post TIPS reduction, the patient reported significant improvement with no clinical signs of HE. Endoscopy approximately 2 months post TIPS reduction showed no evidence of esophageal variceal bleeding.
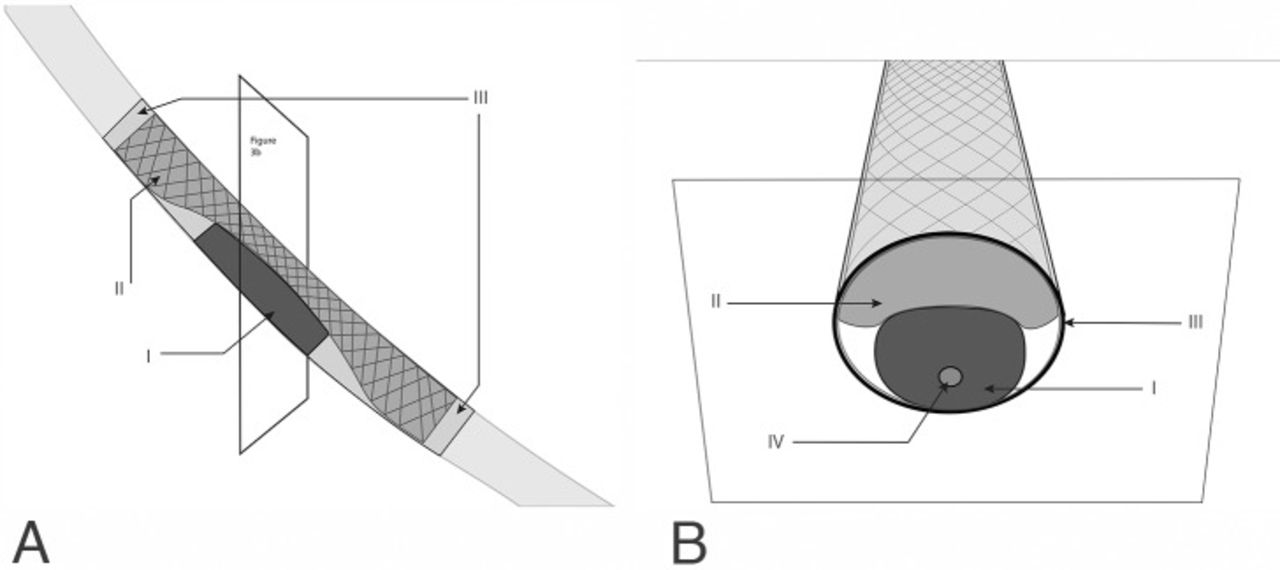
A. The new stent is deployed over a balloon-expanded Genesis stent. B. Cross-section of the reduced stent. I, balloon expandable Genesis stent; II, lumen of the new covered VIATORR stent; III, existing transjugular intrahepatic portosystemic shunt; IV, wire.

Digital subtraction angiography image from a different patient demonstrates appropriate post transjugular intrahepatic portosystemic shunt reducing stent reduction in the mid-shunt lumen.

A. Axial computed tomography (CT) image of the liver shows the deployed Genesis stent (top arrow) and the reduced patent lumen of the new VIATORR stent (bottom arrow). B. Coronal CT image demonstrates 1.7-cm total length of the Genesis stent.
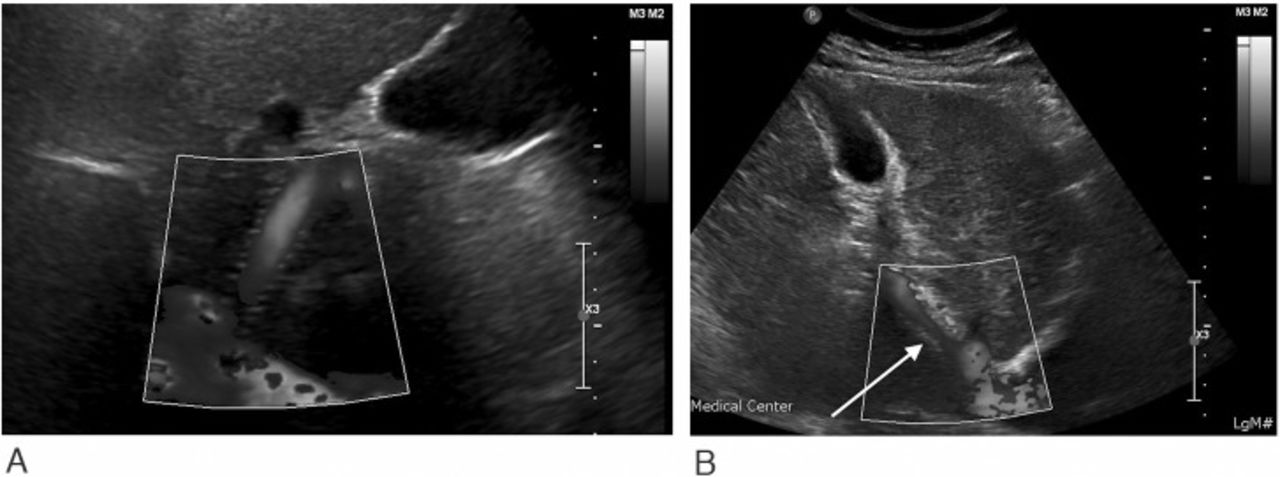
Follow-up ultrasound with Doppler (Figure 6) was performed 10 days post TIPS reduction. Ultrasound demonstrated approximately 50% narrowing of the TIPS and associated elevated velocities at the hepatic venous end consistent with successful TIPS reduction.

Ultrasound power Doppler images show flow prior to TIPS reduction (A) and the expected results with elevated velocity and 50% narrowing at the hepatic vein end of the transjugular intrahepatic portosystemic shunt (TIPS) after TIPS reduction (B).
DISCUSSION
This case demonstrates the common complication of refractory HE following TIPS and is also an example of how shunt reduction has become a key element in TIPS-related refractory HE treatment.3 Previous studies have demonstrated 58%-71% clinical success in treatment of refractory HE via shunt reduction.3-5 While this success rate clearly shows the clinical value in shunt reduction for a potentially debilitating process, caution is advised prior to pursuing reduction because the initial indication for TIPS may recur postprocedure. In particular, ascites may recur in 60% of cases after shunt reduction, risking the development of spontaneous bacterial peritonitis.1 Less commonly, recurrent variceal bleeding has been reported in 9.3% of cases after shunt reduction; consequently, prereduction variceal banding is advised to reduce this complication.1 While the recurrent sequela of portal hypertension is a risk, patients with refractory HE who are not transplant candidates have limited options for treatment after failing medical therapy.1 Proven options such as TIPS-reducing stents provide benefit and can significantly improve quality of life.
As discussed above, endovascular management, such as shunt reduction or occlusion, is often successful for treating patients with TIPS-related refractory HE; however, management pathways need to be adopted for patients in whom the procedure is unsuccessful.3 Pereira et al identified the major mechanisms involved in unsuccessful endovascular management as liver failure or the presence of spontaneous portosystemic shunts (SPSS).3 When liver failure is the cause of HE, liver transplantation is the remaining treatment option. When SPSS is the cause of HE, treatment options before transplantation need to be considered. SPSS result from an increased portosystemic gradient causing intrahepatic or extrahepatic collateral flow and are found in 40% of patients with cirrhosis and in 46%-70% of patients with HE.3 The collateral flow bypasses the liver and shunts blood into the systemic circulation; the resulting decreased hepatic clearance of ammonia and other neurotoxins can lead to HE.2 Treatment options for SPSS include balloon-occluded retrograde transvenous obliteration (BRTO), balloon-occluded antegrade transvenous obliteration (BATO), or a modified retrograde approach from a variety of systemic vascular access points.2 BRTO is an endovascular technique that has been used to occlude gastric varices.2 A balloon is introduced into the outflow vein by a retrograde approach through the shunt and is used to occlude blood flow. A sclerosant is then placed proximal to the site of balloon occlusion.6 As its name suggests, BATO is similar to BRTO but takes an antegrade approach, usually from the portal veins.3
Splenic artery embolization (SAE) has become an option for the management of complications caused by portal hypertension as both an adjunct to BRTO and as a salvage option after previous treatments have failed.3,7 Yoshida et al showed that a combination of BRTO and SAE correlated with a greater reduction in HE episodes compared to BRTO alone.7 While BRTO successfully treats the SPSS, it is not without complications as it can lead to increased portal venous pressure and portal congestion.3 In these cases, SAE has been successful in preventing new SPSS formation by reducing portal flow and pressure.3 Simultaneously, SAE likely increases blood flow to the liver, aiding HE resolution through improved hepatic function.3
We agree with Pereira et al that their proposed clinical practice algorithm and guidelines should be adopted for the optimal endovascular management of TIPS-related refractory HE.3 In addition to adopting this treatment algorithm and future technique improvement, early identification and management of potential complications of SPSS prior to TIPS procedure could result in less posttreatment HE and reduced risk for patients. Because postprocedure complications are significant in number, continued efforts to reduce complications must be pursued. In the meantime, this clinical management algorithm should be applied when these complications occur.
ACKNOWLEDGMENTS
The authors have no financial or proprietary interest in the subject matter of this article.
- © Academic Division of Ochsner Clinic Foundation 2017
In this issue








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.