
Abstract
The 1996 Bethesda Conference acknowledged the following conditions as possible new cardiac risk factors: left ventricular hypertrophy, homocysteine, lipoprotein(a), hypertriglyceridemia, oxidative stress, and fibrinogen. Left ventricular hypertrophy is an independent risk factor for vascular disease, the improvement or progression of which influences subsequent cardiovascular complications. Clinical trials are currently underway to assess potential benefit from lowering homocysteine levels. The role of lipoprotein(a) excess in vascular disease is controversial; its atherogenic potential seems to be neutralized by effective lowering of LDL-cholesterol. Increasing evidence supports the independent role of hypertriglyceridemia in cardiovascular disease and possible clinical benefit from lowering triglyceride levels. Among antioxidant micronutrients, supplementation with vitamin E has been shown to be beneficial in some but not all primary and secondary prevention studies, but data to support use of other antioxidants are much weaker. Preliminary evidence suggests that the reduction of fibrinogen levels in patients with high baseline levels and coronary disease may be beneficial.
Despite the potential relation between new risk factors and cardiovascular disease, routine clinical application of these conditions as cardiovascular risk factors would be premature. We first need evidence that these conditions extend prognostic ability beyond conventional risk factors and that modification of these conditions can decrease the risk of cardiovascular events.
Risk factor modification is an integral part of the management of patients with or at risk for cardiovascular disease. In addition to established cardiovascular risk factors, clinical research has identified more than 100 other conditions that may be associated with an increased risk of cardiovascular disease. An abbreviated list of these new risk factors is shown in Table 1. Clinicians involved in the care of patients with cardiovascular disease should become aware of these new risk factors for several reasons. First, nearly 25% of patients with premature cardiovascular disease do not have any established risk factors. Second, as a result of reductions in morbidity and mortality attributable to hypertension, smoking, and dyslipidemia, the relative contribution of new risk factors to the total burden of cardiovascular disease is likely to increase. Third, significant associations exist between established and new risk factors (Table 2). Better understanding of the new risk factors may shed light on the pathogenetic mechanisms of the established risk factors.
New cardiovascular risk factors
Associations between new and established risk factors
Based on a growing body of evidence, the 1996 Bethesda Conference acknowledged the following conditions as possible risk factors for coronary disease: left ventricular hypertrophy, hyperhomocysteinemia, lipoprotein(a), hypertriglyceridemia, hyper-fibrinogenemia (among other thrombogenic factors), and oxidative stress (1). The following discussion will review the role of these selected new risk factors in cardiovascular disease. Other potential new risk factors, such as infectious agents, inflammatory markers, and procoagulant substances, while probably equally promising, are not the subject of this review.
Left Ventricular Hypertrophy
Left ventricular hypertrophy is the response of the heart to chronic pressure or volume overload and is defined as left ventricular mass exceeding 131 g/m2 of body surface area in men and 100 g/m2 in women. Echocardiography is accepted as the method of choice for estimating left ventricular mass.
In the Framingham Heart Study (2), left ventricular hypertrophy was present in 16% and 19% of men and women, respectively. Age, blood pressure, obesity, valve disease, and myocardial infarction are independently associated with left ventricular hypertrophy (2). Sodium intake, hereditary factors, and neurohumoral factors are also thought to play a role in determining left ventricular mass.
Three distinct patterns of left ventricular hypertrophy have been identified depending on left ventricular mass index (LVMI), expressed in g/m2, and relative wall thickness (RWT = 2 x posterior wall thickness/left ventricle end-diastolic diameter) (Figure 1) (3).
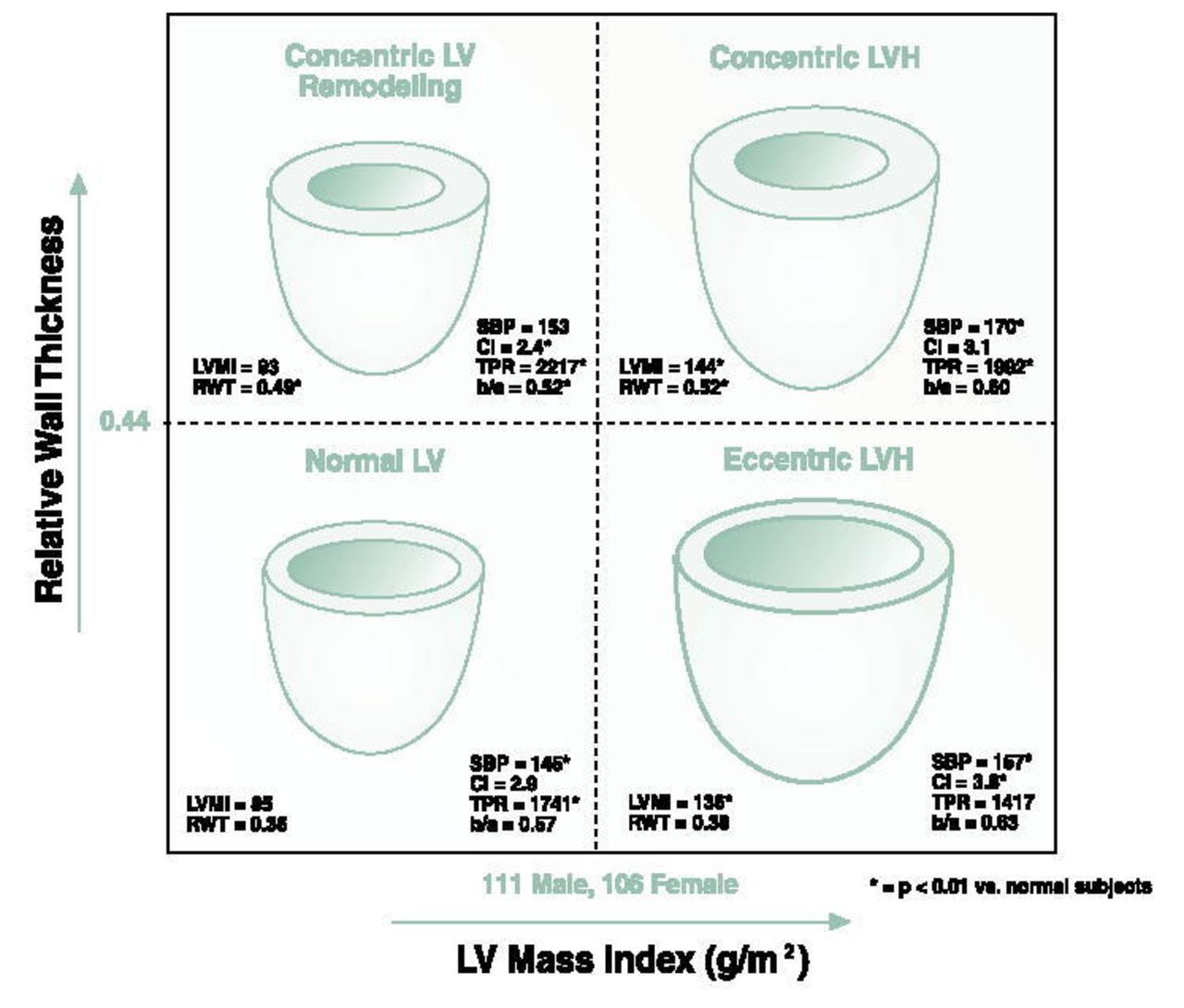
Hemodynamic and geometric profiles in hypertensive patients with the four patterns of left ventricular (LV) geometry. The short-axis/long axis ratio (b/a) was derived by two-dimensional echocardiography. CI = cardiac index (liters/min per m2); LVH = left ventricular hypertrophy; LVMI = left ventricular mass index (g/m2); RWT = relative wall thickness; SBP = systolic blood pressure; TPR = total peripheral resistance (dynes·s·cm−5). (Reprinted with permission from the American College of Cardiology [J Am Coll Cardiol 1992; 19:1550–1558]. [3])

Dr. Harjai is a staff Cardiologist at Ochsner Clinic at Lady of the Sea Hospital in Cut-Off, Louisiana
Left ventricular hypertrophy is independently associated with increased incidence of cardiovascular disease, cardiovascular and all-cause mortality (4), and stroke (5). The adjusted odds ratios for morbid events among patients with left ventricular hypertrophy compared with those without ranges from 1.4 to 5.4 (6). Among patients with essential hypertension, those with concentric left ventricular hypertrophy have a higher risk of death and morbid events compared with those suffering from eccentric hypertrophy or concentric remodeling (7). In a pooled analysis of 1145 patients in four studies, the incidence of morbid events in patients with left ventricular hypertrophy progression was 13–59 % compared with 7–12 % in those with left ventricular hypertrophy regression (6). Diminished coronary vasodilator reserve, increased myocardial oxygen demand, subendocardial ischemia, lethal arrhythmias, and diminished ventricular performance may explain the increased risk associated with left ventricular hypertrophy (8).
Nonpharmacological interventions such as weight reduction, sodium restriction, and aerobic physical exercise can reduce left ventricular mass. In essential hypertension patients, effective blood pressure control is the most important intervention to reduce left ventricular mass (9). It is suspected that different antihypertensive medications may have disparate effects on left ventricular mass, independent of blood pressure reduction. In a meta-analysis of 39 clinical trials performed through June 1995, the use of angiotensin-converting enzyme inhibitors, calcium channel blockers, diuretics, and beta-blockers was associated with 13%, 9%, 7%, and 6% reductions in left ventricular mass, respectively (9).
The lack of standard, universally accepted echocardiographic criteria for left ventricular hypertrophy and the absence of definitive, prospective evidence that reversing left ventricular hypertrophy will improve clinical outcomes over and above that achievable with blood pressure control alone have limited the application of left ventricular hypertrophy as a risk factor in routine clinical practice.
Homocysteine
Homocysteine is an intermediate compound derived from methionine. Fasting total homocysteine concentrations of 5–15 mmol/L are considered normal. Some patients with normal fasting homocysteine levels have a latent abnormality of homocysteine metabolism, which can be diagnosed by measuring homocysteine levels after a methionine load.
The association of hyperhomocysteinemia with atherosclerotic and thrombotic vascular disease was first seen in patients with homocystinuria, a rare autosomal recessive disease due to deficiency of cystathionine beta-synthetase, characterized by exceedingly high blood levels of homocysteine and presence of homocysteine in urine, along with skeletal defects, mental retardation, and lens dislocation (10). In recent investigations, mild-to-moderate hyperhomocysteinemia has been independently associated with coronary artery disease, myocardial infarction, peripheral vascular disease, cerebrovascular disease, stroke, cardiac allograft vasculopathy, and mortality from coronary artery disease. The relation between homocysteine levels and vascular disease is suspected to be graded. Each 5 micromol/L increase in fasting homocysteine level is estimated to lead to a 1.6 to 1.8-fold increase in the incidence of coronary disease (11). In the Physicians' Health Study, the adjusted relative risk of subsequent myocardial infarction among subjects with homocysteine levels in the top 5th percentile (>15.8 mmol/L) was 3.4 compared with those with levels in the bottom 90th percentile (12). In contrast to cross-sectional studies, results from prospective studies have been less consistent. Only two (12, 13) of five prospective studies (12–16) have found a positive relation between homocysteine levels and coronary disease, raising doubts about a cause-effect relation between hyper-homocysteinemia and vascular disease.
Several effects of homocysteine may contribute to its role in vascular disease. Homocysteine promotes endothelial dysfunction, endothelial cell injury, and smooth muscle cell proliferation. Additionally, it enhances thromboxane A2 formation and platelet aggregation, reduces the protective effect of endothelium-derived relaxing factor, increases binding of lipoprotein(a) to fibrin, and has procoagulant effects.
Genetic, nutritional, and other factors are involved in the development of hyperhomocysteinemia. Up to 80% of patients with hyperhomocysteinemia have low cystathionine beta-synthase activity. Low levels of folate, vitamin B12, and vitamin B6 are commonly seen in patients with hyperhomocysteinemia. Whether nutritional deficiency of these vitamins by itself can raise homocysteine levels or whether this response occurs only in subjects with a genetic predisposition to hyperhomocysteinemia is unknown.
In subjects with hyperhomocysteinemia, supplementation with folate, vitamin B12, and vitamin B6 is effective in reducing homocysteine levels. Folate is the single most powerful homocysteine lowering agent and is effective in doses as low as 0.65 mg/d. Higher doses are required in subjects with renal insufficiency. The exact dose and duration of folate therapy remain to be defined, especially in view of the recent folate fortification of cereal-grain products in the United States, which may increase plasma folate levels and decrease homocysteine levels. The concern that folate therapy may unmask underlying vitamin B12 deficiency in the elderly may be addressed by additional supplementation with 1 mg/d vitamin B12. In small studies, the use of oral estrogen in men and postmenopausal women is associated with a 11–14 % reduction in fasting homocysteine levels.
Despite the potential relation between hyper-homocysteinemia and vascular disease seen in epidemiologic and observational studies, there are no prospective data yet that support benefit from reduction in homocysteine levels. Large prospective, randomized, clinical trials are underway to address the impact of lowering homocysteine levels on vascular risk.
Lipoprotein(a)
The lipoprotein(a) [Lp(a)] molecule is structurally similar to low-density lipoprotein cholesterol (LDL-C) with the addition of a large glycoprotein, designated as apo(a). Lp(a) competes with plasminogen for binding sites, resulting in decreased synthesis of plasmin and inhibition of fibrinolysis. Other Lp(a) effects include increased cholesterol deposition in the arterial wall, enhanced foam cell formation, generation of oxygen-free radicals in monocytes, promotion of smooth muscle cell proliferation, and induction of monocyte chemotactic activity in endothelial cells.
Significant controversy surrounds the role of elevated levels of Lp(a) as a risk factor for vascular disease. On the one hand, prospective and retrospective studies have suggested an independent association between high levels of Lp(a) (>30 mg/dL) and presence and extent of coronary artery disease, premature coronary artery disease, myocardial infarction, restenosis after balloon angioplasty, cerebrovascular disease, saphenous vein bypass graft disease, and cardiac allograft vasculopathy (17, 18). This association has been documented in men, women, Caucasians, African-Americans, and Asian-Indians. Up to 20% of patients with premature coronary artery disease have elevated Lp(a) levels (19), making Lp(a) the most common inherited lipoprotein disorder in these patients.
However, other studies, such as the Physicians' Health Study and the Helsinki Heart Study, have shown no association between Lp(a) levels and vascular disease (20–22). Based on current evidence, the value of screening for and treating Lp(a) excess is debatable, especially given the many other risk factors for which modification is known to be beneficial. Treatment of Lp(a) excess could be considered for subjects with a history of premature vascular disease not attributable to other risk factors, only with the clear understanding that no trial data exist to show clinical benefit from lowering Lp(a) levels. In men with high LDL-C and high Lp(a) levels, the atherogenic potential of Lp(a) is neutralized by effective lowering of LDL-C. Most dietary interventions, anti-lipid drugs, and exercise do not affect Lp(a) levels; recent evidence suggests that a fish diet may reduce Lp(a) levels. Of currently available antilipid measures, only estrogens (in postmenopausal women) and nicotinic acid (3–4 g/d) are associated with reduction in Lp(a) levels.
Hypertriglyceridemia
The exact role of hypertriglyceridemia as a risk factor for atherosclerosis remains elusive. Although high fasting triglyceride levels are generally predictive of cardiovascular risk, multivariate adjustment for other risk factors diminishes this association. Further, significant intraindividual variation exists in fasting plasma triglyceride levels and likely leads to substantial bias in epidemiological studies.
Nevertheless, there is a growing body of evidence to support hypertriglyceridemia as an independent cardiac risk factor. In a meta-analysis of 17 population-based, prospective studies involving over 57,000 subjects (23), each increase in serum triglyceride level by 1 mmol/L (88.6 mg/dL) was associated with crude relative risks of 1.32 and 1.76, for men and women, respectively, for the development of cardiovascular disease. After adjustment for other risk factors, the relative risks remained significant at 1.14 and 1.37, respectively. Other recent studies concluded that fasting and nonfasting triglyceride levels are significant, independent predictors of the future risk of myocardial infarction.
Hypertriglyceridemia frequently coexists with low levels of HDL-C, high levels of atherogenic lipids (such as small, dense LDL particles), insulin resistance, diabetes mellitus, obesity, and sedentary lifestyle. Hypertriglyceridemia may represent a procoagulant state mediated by increased levels of factors 1, 7, 8, 10, and plasminogen activator inhibitor 1, and reduced tissue plasminogen activator activity. Triglyceride-rich lipoproteins may also be directly atherogenic.
While definitive data are lacking, clinical studies seem to suggest a beneficial effect from lowering triglyceride levels. The Bezafibrate Infarction Prevention Study (BIP) enrolled 3122 patients with coronary artery disease (serum total cholesterol 180–250 mg/dL, LDL-cholesterol ≤ 180 mg/dL, HDL-cholesterol ≤ 45 mg/dL, triglycerides ≤ 300 mg/dL) to evaluate the efficacy of bezafibrate-induced reduction in serum triglycerides and increase in HDL-cholesterol on the incidence of fatal and nonfatal myocardial infarction and sudden death (24). Among patients with high baseline triglycerides (>200 mg/dL), bezafibrate reduced the incidence of study endpoints. In the Bezafibrate Coronary Artery Intervention Trial (BECAIT) of patients with coronary artery disease, bezafibrate decreased the incidence of acute coronary events and the progression of angiographic disease (25). The magnitude of benefit was similar to that seen with simvastatin and pravastatin. Since LDL levels were essentially unchanged in BECAIT, benefit from bezafibrate likely relates to other effects of this drug, such as triglyceride reduction. However, patients on bezafibrate also had reduction in fibrinogen and increase in HDL levels, which could explain some of the benefit from this drug.
Benefit from lowering triglyceride levels, while suggestive, remains largely indirect. It may be reasonable to attempt triglyceride reduction in hypertriglyceridemic subjects with documented or at high-risk for atherosclerosis. Measures like weight loss, caloric restriction, physical activity, decreased alcohol consumption, and smoking cessation, which reduce triglyceride levels, may also lower cardiovascular risk independent of their effect on triglycerides.
Oxidative Stress
Oxidative modification of LDL-C plays a central role in atherogenesis. Oxidized LDL acts as chemo-attractant for T-lymphocytes and monocytes, immobilizes macrophages within the cell wall, increases LDL uptake by the macrophages, and promotes the formation of foam cells. Additionally, oxidized LDL is directly cytotoxic to subendothelial and smooth muscle cells. “Oxidative stress,” while not a readily measured entity, underlies the current enthusiasm regarding antioxidants in preventive cardiology.
Primary Prevention Studies
Epidemiological and observational studies have suggested that high intakes of certain micronutrients (vitamins E, C, and A) may provide primary protection against cardiovascular disease. The First National Health and Nutrition Examination Survey (NHANES I) (26) suggested that daily vitamin C intake was inversely related to cardiovascular and all-cause mortality. In almost 40,000 middle-aged US male health professionals, the consumption of supplemental vitamin E (≥100 IU daily) for ≥2 years was associated with a 37% reduction in the incidence of coronary disease (27). In the Nurses' Health Study, supplemental vitamin E was associated with a 41% reduction in the incidence of coronary disease over 8 years of follow-up (28).
Optimism regarding the role of antioxidant vitamins in primary prevention was blunted by the results of placebo-controlled, primary prevention trials. In the Alpha-Tocopherol Beta Carotene Cancer Prevention Study (29), the use of vitamin E 50 mg/d) was associated with a slight reduction in deaths from coronary disease (crude relative risk reduction of 5%), but a greater number of deaths from cancers and hemorrhagic stroke, resulting in a nonsignificant 2% higher mortality in subjects who received vitamin E. Among participants who received beta-carotene, there was an increased incidence of deaths from lung cancer, coronary disease, and ischemic and hemorrhagic stroke, resulting in a significant 8% increase in total mortality over 5–8 years of follow-up. Similarly, in the Beta-Carotene and Retinol Efficacy Trial (30), a double-blind placebo-controlled trial of 30 mg beta-carotene and 25,000 IU of retinyl palmitate vs. placebo in >18,000 subjects, higher incidence of and mortality from lung cancer were seen in the active intervention group (30). In the Physicians' Health Study of 22,071 healthy US male physicians, supplementation with beta-carotene (50 mg on alternate days) produced no significant change in the incidence of malignant neoplasms, cardiovascular disease, or death from all causes (31).
Secondary Prevention Studies
In the Cambridge Heart Antioxidant Study (32), over 2000 patients with documented coronary disease were randomized to receive placebo or vitamin E (400 IU or 800 IU daily). Over a median follow-up of 1.4 years, patients randomized to receive vitamin E had a 77% reduction in the risk of nonfatal myocardial infarction but no reduction in cardiovascular deaths. In the Cholesterol-Lowering Atherosclerosis Study (CLAS) (33), supplemental vitamin E (≥100 IU daily) lead to a decrease in the rate of progression of angiographically diagnosed coronary disease. However, in the recently published Heart Outcomes Prevention Evaluation (HOPE) Study , the use of supplemental vitamin E for a mean period of 4.5 years did not provide any benefit in patients at high risk for cardiovascular events (34).
Oxidative Stress Summary
Definitive results of ongoing prospective clinical trials will hopefully clarify the ambivalence regarding the use of vitamin supplements. In the meanwhile, daily supplementation with vitamin E (400 IU) may be considered in patients with documented coronary artery disease, with the caveat that such treatment may reduce the incidence of nonfatal myocardial infarction but does not reduce cardiovascular mortality. Data to support the use of vitamins A and C are much weaker.
Oxidative stress can also be modified by specific dietary measures. Two diets that have received attention are the “Mediterranean Diet,” which is rich in oxidation-resistant monounsaturated fat, and diets rich in omega-3 fatty acids. The beneficial effects of these diets may be related to their antioxidant properties. Additionally, flavonoids, present in red wine, fruits, vegetables, and tea, have strong antioxidant properties and may have cardioprotective effects.
Hyperfibrinogenemia
Several recent studies have established the association of plasma fibrinogen levels with cardiovascular disease. In one pooled analysis (35), the odds ratio for coronary disease for the highest vs. the lowest tertile of fibrinogen level was 2.3. In patients with established coronary disease, fibrinogen levels are associated with angiographic severity of disease, recurrent ischemic events, and risk of restenosis following coronary angioplasty. In male nonsmokers, fibrinogen levels show a strong association with all cause and cardiovascular mortality. In patients presenting with unstable angina or non-Q wave infarction, hyperfibrinogenemia is associated with a higher chance of death or myocardial infarction. Preliminary results of the BIP Study suggest that reduction of plasma fibrinogen levels in patients with high baseline fibrinogen levels and preexisting coronary artery disease leads to a decrease in the incidence of cardiac death and ischemic stroke (36).
In addition to its role in the coagulation cascade, fibrinogen stimulates smooth muscle cell migration and proliferation, promotes platelet aggregation, increases blood viscosity, and may have mitogenic and angiogenic properties. Furthermore, fibrin binds to lipoprotein in the vascular intima and may enhance accumulation of extracellular lipid in fibrous plaques. Hyperfibrinogenemia may also be a marker of the inflammatory activity associated with the atherosclerotic process.
High fibrinogen levels are associated with increased age, female sex, obesity, smoking, physical inactivity, family history of premature coronary disease, high levels of LDL-C and triglycerides, low levels of HDL-C, and personal history of hypertension or diabetes. Socioeconomic factors, such as lower social and educational class, lack of control over work, lower body height, and acute mental stress are also associated with higher fibrinogen levels. Additionally, substantial variability in fibrinogen level exists within patients, and it has been suggested that a single fibrinogen reading is not adequate for prediction of vascular risk.
Smoking cessation, weight loss, regular exercise, and moderate alcohol consumption are known to reduce plasma fibrinogen levels. Therapy with bezafibrate, ciprofibrate, and phenofibrate, but not gemfibrozil, may reduce fibrinogen levels by up to 40%. In postmenopausal women and elderly men, estrogen replacement is associated with significant reduction of plasma fibrinogen levels. Ticlopidine, but not aspirin, is known to reduce fibrinogen levels.
The lack of a single standardized assay, the presence of intraindividual variability in levels, and lack of conclusive evidence that reduction in fibrinogen levels would improve cardiovascular risk have limited the wide application of fibrinogen level reduction in clinical practice.
Implications
In an effort to better predict the development of vascular disease, recent studies have identified a host of new risk factors. The success of preventive measures against established risk factors (hypertension, hypercholesterolemia, and smoking) seen in the last 3 decades, and the sheer magnitude of vascular disease burden justify the enthusiasm surrounding new risk factors. For several reasons, however, definite recommendations for screening and modification of new risk factors cannot yet be made. First, despite the abundance of data associating new risk factors with cardiovascular disease (Table 3), there is a dearth of definitive information regarding the impact of modifying new risk factors on the course of cardiovascular disease. Second, we need evidence that assessment of new risk factors will extend our prognostic ability beyond strategies using established risk factors alone (37). Additionally, measurement techniques for some new risk factors need better standardization [e.g. Lp(a), fibrinogen]. Further, the cost implications of screening for and modifying new risk factors, including those discussed in this review as well as other equally promising risk factors (inflammatory markers, infectious agents, and prothrombotic states) need to be determined (37). Clinical trials that address the effect of modifying new risk factors on cardiovascular outcomes will help in selecting risk factors with potential for clinical use.
Summary of evidence supporting the pathogenetic role of new cardiovascular risk factors
- Ochsner Clinic and Alton Ochsner Medical Foundation
References
In this issue








{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.